Abstract
CPD/Clinical Relevance: The reader will learn a method of simplifying the process of taking a lateral skull radiograph with the mandible in a reproducible position in patients who have a variable jaw closure position.
From Volume 17, Issue 2, April 2024 | Pages 77-79
CPD/Clinical Relevance: The reader will learn a method of simplifying the process of taking a lateral skull radiograph with the mandible in a reproducible position in patients who have a variable jaw closure position.

The technique of taking a lateral skull radiograph is standardized with the patient positioned in the cephalostat, the sagittal plane of the head parallel to the film, the X-ray source 1.5 m from the midsagittal plane of the patient and the film 30 cm behind the midsagittal plane, the Frankfort plane horizontal, ear rods in the external meatus, and teeth in maximum intercuspation.1 The final step of biting into maximum intercuspation can be problematic for some patients and lead to errors in jaw positioning recorded on the radiograph. Techniques to avoid repositioning errors reduce the need for imaging to be repeated and reduce X-ray exposure.
Most patients when asked to bite their teeth together, close into a comfortable, reproducible position where the maximum number of tooth contacts occur, the intercuspal position (ICP). Movement of the mandible into this position is guided by the tooth morphology, but may also be a learned habit as patients may posture their jaw to mask a malocclusion or avoid a displacement. A reproducible jaw position is important to plan treatment. To find the true occlusal discrepancy, the clinician must find the patient's centric relation, the occlusion when the teeth are in contact during closure on the hinge axis, with the condyles maximally seated in their fossae.2 It can be challenging to manipulate the patient into this position, and even harder again to then take a lateral skull radiograph in this position.
The aim of this clinical tip is to provide a method of simplifying the process of taking a lateral skull radiograph with the mandible in a reproducible position in patients who have a variable jaw closure position.
A 14-year-old male was referred to the orthodontic department with a Class III incisor relationship on a Class III skeletal pattern and a chin point deviated to the right. There was an associated right-sided cross bite without displacement, and a right-sided lateral open bite. It was challenging to get the patient to bite in a reproducible position of centric relation (Figure 1). Unknown to the authors, he habitually held his lower jaw slightly open (Figure 2). Achieving a reproducible centric relation was such a challenge that the occlusion was incorrect on his lateral lateral skull radiograph (Figure 3).


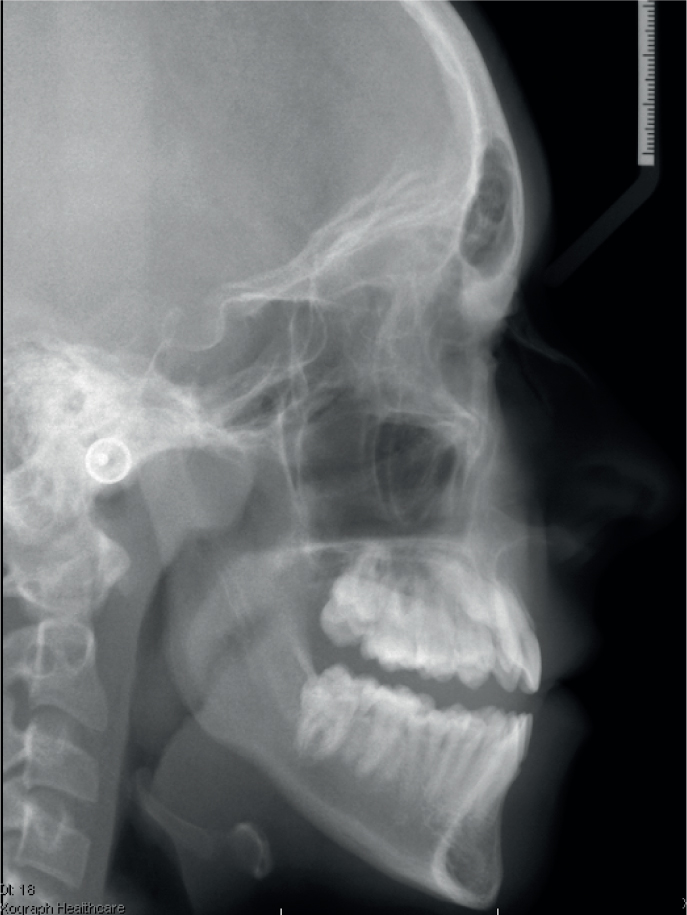
To ensure the patient was biting correctly into centric relation, a wax bite was used to record this occlusion, this was cooled and then replaced in the mouth (Figures 4 and 5). The patient was asked to continue to bite into the wax until the radiograph was taken. If he happened to open his mouth, the wax would guide his mandible back to the correct occlusion. Wax is radiolucent and will not show up on the radiograph. Polyvinylsiloxane (putty) was considered, but should not be used for this technique because it is radiopaque. The radiograph was retaken in the patient's correct occlusion (Figure 6).



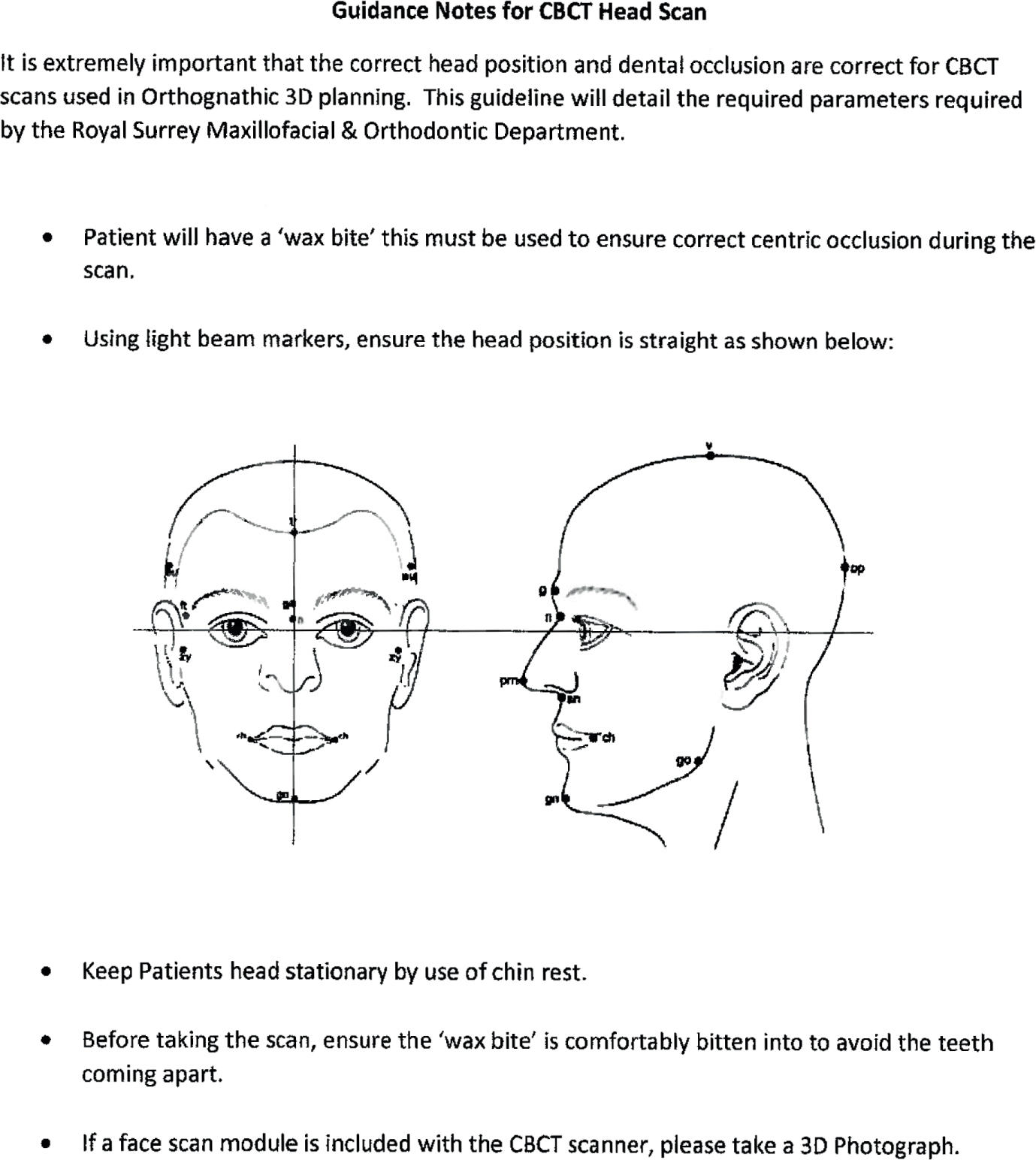
This wax bite technique to position the mandible correctly prior to a lateral skull radiograph is easy and cheap, and may avoid repeating a radiograph. It is especially useful where radiographs may be taken outside the clinic, or even in a different location. The authors also routinely use the wax bite technique for an accurate occlusal record of the CBCT scans for orthognathic 3D planning (Figure 7). These images are taken at a separate site.