Hatamleh MM, Ong J, Hatamleh ZM, Watson J, Huppa C. Developing an in-house interdisciplinary three-dimensional service: challenges, benefits, and innovative health care solutions. J Craniofac Surg. 2018; 29:1870-1875 https://doi.org/10.1097/scs.0000000000004743
Al Mortadi N, Eggbeer D, Lewis J, Williams RJ. CAD/CAM/AM applications in the manufacture of dental appliances. Am J Dentofacial Orthop. 2012; 142:727-733 https://doi.org/10.1016/j.ajodo.2012.04.023
Alcan T, Ceylanoğlu C, Baysal B. The relationship between digital model accuracy and time-dependent deformation of alginate impressions. Angle Orthod. 2009; 79:30-36 https://doi.org/10.2319/100307-475.1
Taneva E, Kusnoto B, Evans CA. 3D scanning, imaging, and printing in orthodontics. Contemp Orthod. 2015; 3 https://doi.org/10.5772/60010
Groth CH, Kravitz ND, Shirck JM. Incorporating three-dimensional printing in orthodontics. J Clin Orthod. 2018; 52:28-33
Westerlund A, Tancredi W, Ransjö M, Bresin A, Psonis S, Torgersson O. Digital casts in orthodontics: a comparison of 4 software systems. Am J Dentofacial Orthop. 2015; 147:509-516
Rheude B, Lionel Sadowsky P, Ferriera A, Jacobson A. An evaluation of the use of digital study models in orthodontic diagnosis and treatment planning. Angle Orthod. 2005; 75:300-304 https://doi.org/10.1043/0003-3219(2005)75[300aeotuo]2.0.co;2
Richmond S, Shaw WC, O'Brien KD, Buchanan IB, Jones R, Stephens CD, Roberts CT, Andrews M. The development of the PAR Index (Peer Assessment Rating): reliability and validity. The Eur J Orthod. 1992; 14:125-139 https://doi.org/10.1093/ejo/14.2.125
Mayers M, Firestone AR, Rashid R, Vig KW. Comparison of peer assessment rating (PAR) index scores of plaster and computer-based digital models. Am J Dentofacial Orthop. 2005; 128:431-434 https://doi.org/10.1016/j.ajodo.2004.04.035
Luqmani S, Jones A, Andiappan M, Cobourne MT. A comparison of conventional vs automated digital Peer Assessment Rating scoring using the Carestream 3600 scanner and CS Model+ software system: A randomized controlled trial. Am J Dentofacial Orthop. 2020; 157:148-155 https://doi.org/10.1016/j.ajodo.2019.10.011
Wiechmann D, Rummel V, Thalheim A, Simon JS, Wiechmann L. Customized brackets and archwires for lingual orthodontic treatment. Am J Dentofacial Orthop. 2003; 124:593-599
Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. 2015; 85:881-889 https://doi.org/10.2319/061614-436.1
Nasef AA, El-Beialy AR, Eid FH, Mostafa YA. Accuracy of orthodontic 3D printed retainers versus thermoformed retainers. Open J Med Imaging. 2017; 7:169-179 https://doi.org/10.4236/ojmi.2017.74017
Cole D, Bencharit S, Carrico CK, Arias A, Tüfekçi E. Evaluation of fit for 3D-printed retainers compared with thermoform retainers. Am J Dentofacial Orthop. 2019; 155:592-599 https://doi.org/10.1016/j.ajodo.2018.09.011
Baan F, de Waard O, Bruggink R, Xi T, Ongkosuwito EM, Maal TJ. Virtual setup in orthodontics: planning and evaluation. Clin Oral Investig. 2019; 12:1-9 https://doi.org/10.1007/s00784-019-03097-3
Czolgosz I, Cattaneo PM, Cornelis MA. Computer-aided indirect bonding versus traditional direct bonding of orthodontic brackets: bonding time, immediate bonding failures, and cost-minimization. A randomized controlled trial. 2020; 34:144-151 https://doi.org/10.1093/ejo/cjaa045
Brown MW, Koroluk L, Ko CC, Zhang K, Chen M, Nguyen T. Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am J Dentofacial Orthop. 2015; 148:1067-1074 https://doi.org/10.1016/j.ajodo.2015.07.029
Digital workflows part 1: applications of digital technology in orthodontics Chris Keating Jennifer Haworth Farnaz Parvizi Dental Update 2024 16:4, 707-709.
Authors
ChrisKeating
BA (Hons) FdSc MOTA
Advanced Digital OMFS & Orthodontic Technologist, Royal United Hospitals NHS Foundation Trust, Bath, United Kingdom
This is the first article in a two-part series considering the relevance and clinical uses of digital technologies in relation to orthodontics. The aim is to take a closer look at a ‘point-of-care’ digital service and highlight the key areas in which digital workflows have been employed, along with areas of future development. The second article will document the application of digital workflows in joint orthodontic/orthognathic treatment and present two clinical cases which have undergone treatment by means of a digital workflow.
CPD/Clinical relevance: Digital technologies can enhance orthodontic clinical care.
Article
The integration of digital technologies and three-dimensional (3D) printing in healthcare has risen drastically over the course of the past decade. Once reserved for industrial processes such as tooling design and fabrication, as well as visual and functional rapid prototyping methods, these technologies have since been developed and applied to several areas of dentistry, including orthodontics. While digital technologies might initially be more expensive, requiring relatively high levels of investment compared to more conventional methods, they offer distinct advantages. These include the ability to digitally replicate, modify and print human anatomical structures or appliances in 3D, with the potential to improve reproducibility, efficiency and the overall quality of orthodontic treatment.1,2,3
Current applications of computer-aided design (CAD) and computer-aided manufacturing (CAM) include a number of tasks specific to orthodontics.3,4 In their simplest form, these digital workflows can be divided into data acquisition (scanning) and data usage or outputs, including 3D printing. This article will describe the use of intra-oral scanning and 3D printing before turning to specific orthodontic applications of digital technology.
Intra-oral scanning
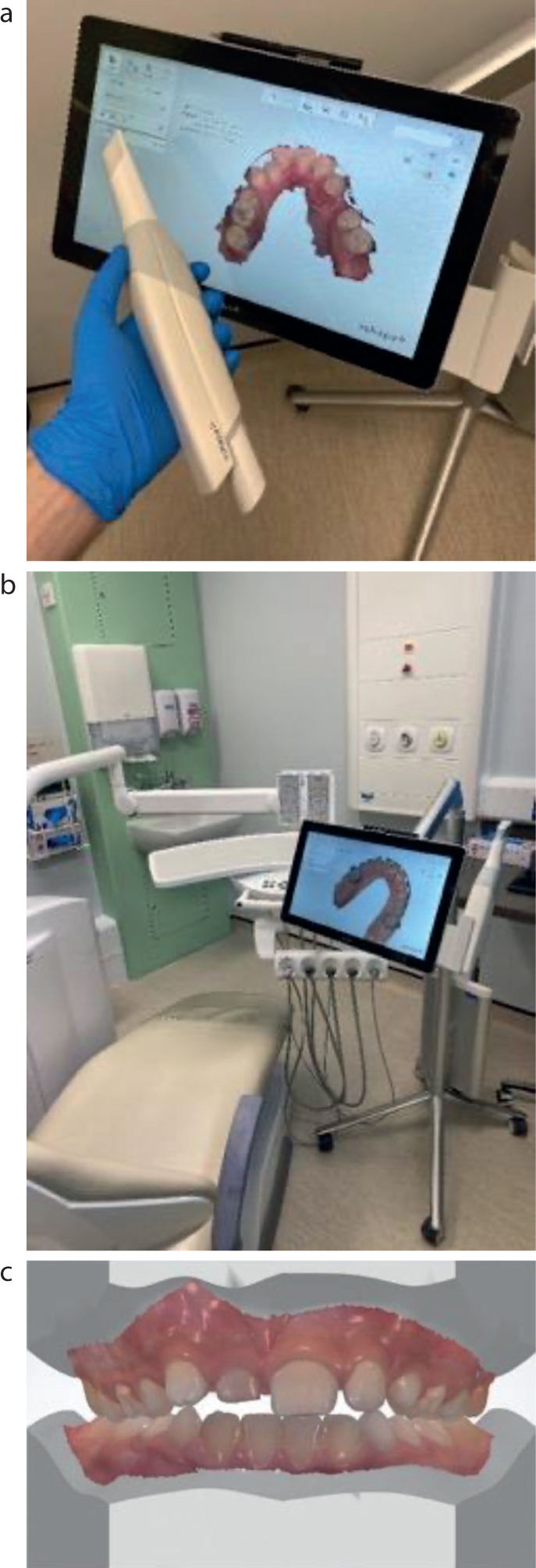
It is possible to capture accurate representations of the teeth and occlusion, create digital 3D models, and improve the patient experience by replacing traditional alginate impressions with intra-oral scans (Figure 1). Although alginate is an easy to use and cost-effective impression material, it is susceptible to syneresis (distortion) after impressions are taken, and taking impressions can be an uncomfortable experience for some patients.5 As with any new technique, intra-oral scanning can initially take longer to perform than conventional methods of taking impressions, although this typically improves with repetition. Intra-oral scanning is also associated with reduced levels of patient discomfort and fewer inconsistencies compared with traditional impression techniques, and can eliminate the need for subsequent transport and packaging.6 The relative merits of both the conventional analogue and newer digital impression techniques are outlined in Table 1.
Figure 1. 3Shape TRIOS 3 intra-oral scanner. (a) The wireless handheld intra-oral scanner and the 3Shape Move+ scanning unit displaying a maxillary arch obtained by intra-oral scanning. (b) The intra-oral scanner in a clinical environment. (c) A colour orthodontic study model obtained by intra-oral scanning.
Table 1. A comparison of analogue and digital impression taking techniques.
Intra-oral scanning
Analogue impression taking
Benefits
Drawbacks
Benefits
Drawbacks
Hygienic handling
High acquisition costs
Low cost
Susceptible to distortion if unsupported
Increased level of patient comfort
On-going financial commitment through software licensing and equipment warranty
Reasonable surface detail
Poor dimensional stability
Increased precision in impression taking
Additional staff training required
Non-toxic
Uncomfortable for the patient
Improved accuracy and treatment outcome
Neutral taste
Easy to transfer and store
Limited working time (temperature dependant)
Digital models constructed from the intra-oral scans are saved in a commonly used standard tessellation language file format that can recreate accurate surface geometry in the case of both intra-oral 3D images and models. These files can be modified chair-side or sent remotely to a laboratory, where they can be used to design and manufacture study models and orthodontic appliances, including retainers, aligners and indirect bonding trays.7, 8
3D printing
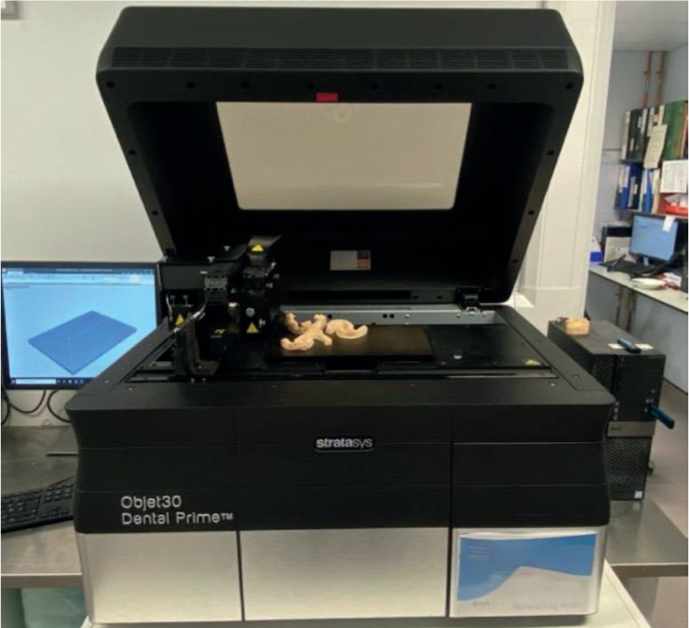
3D printing technology (Figure 2) can produce a wide variety of products to a high level of precision9, as the printed horizontal layer thickness is typically in the range of just 16–36µm. Such products include printed dental study and working models, removable appliances, customised orthodontic appliances and surgical guides.4,10 3D printers can also produce anatomical maxillofacial models, custom implants, osteotomy cutting guides and orthognathic wafers2. However, it should be noted that implementing 3D printing technology can be both time consuming and costly.1 The role of 3D printing will be discussed further in the following sections of the paper.
Figure 2. Stratasys Objet 30 Dental Prime 3D Printer situated in the oral and maxillofacial and orthodontic laboratory at the Royal United Hospital in Bath.
Records
Digital study models
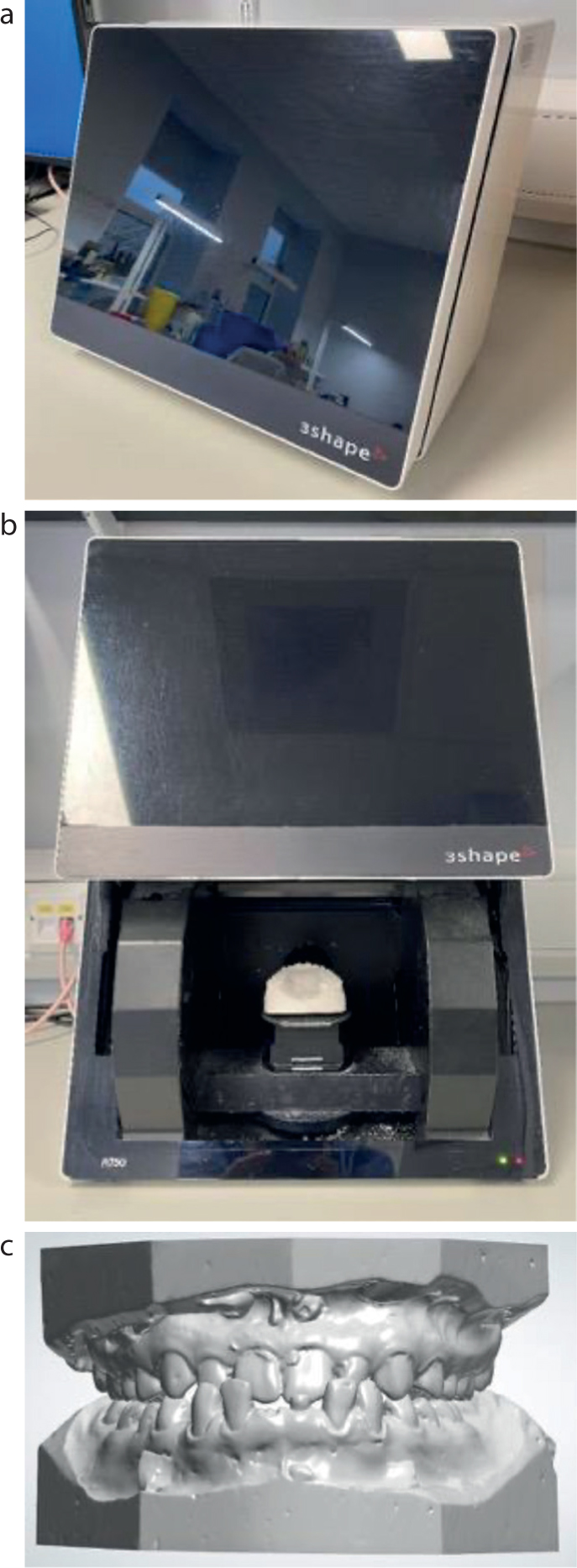
Plaster study models have been traditionally viewed as the ‘gold standard’ in orthodontics, mainly due to their accuracy, ease of production and cost effectiveness. However, they also have many drawbacks including fragility, degradation over time, demands on space, cost of storage and difficulties of transfer11. For these reasons, digital study models are becoming increasingly popular as a way of capturing clinical information6, with many clinicians now archiving their study models along with other patient records digitally for ease of immediate access, storage and transfer of patient data. The advantages and disadvantages are described in Table 2. Digital study models can be obtained by either using a 3D model scanner to scan gypsum casts (Figure 3) or by direct intra-oral scanning. 4,9
Table 2. Summary of the advantages and disadvantages of digital study models.
Advantages
Disadvantages
Easy to store, organise and retrieve
Investment in a digital technology system
Durable
On-going financial commitment through software licensing and equipment warranty
Easily transferable
Additional staff training
Diagnostic versatility
Patient data is stored securely behind a firewall
Figure 3. The 3Shape R750 gypsum model scanner situated in the oral and maxillofacial and orthodontic laboratory at the Royal United Hospital in Bath (a and b); c) digitised gypsum study model.
Analysis
PAR Scoring
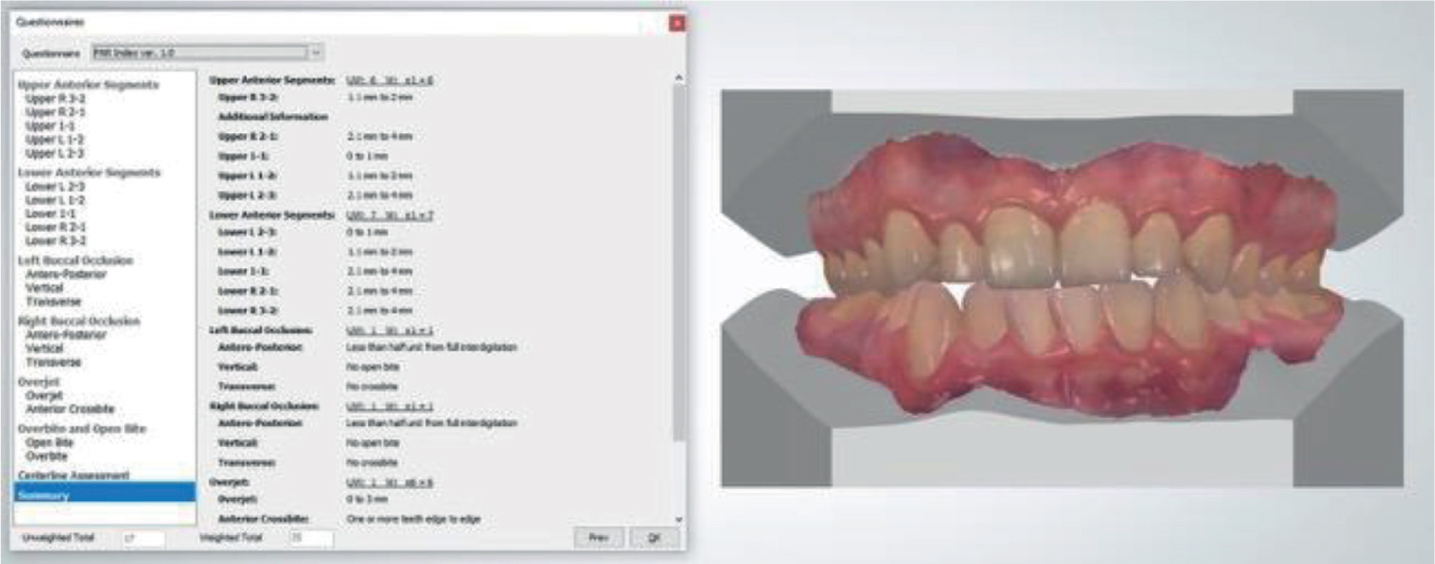
The peer assessment rating (PAR) index is an objective method for evaluating treatment outcome (Richmond et al, 1992), which is valid and reliable. PAR scores derived from both digital models and intra oral scans are valid and reliable measures of treatment change (Figure 4). However, the current method used for obtaining a PAR score from a digital record can be time consuming13.
Figure 4. The 3Shape OrthoAnalyzer peer assessment rating score questionnaire module and a digital pre-treatment orthodontic study model.
The integrated workflow consists of multiple stages of model preparation to attain each score, with the operator using a number of tools within the software to assess each occlusal anomaly before a final PAR score is calculated. Currently, the conventional method of PAR scoring using plaster models appears more efficient. Carestream Dental have developed an automated PAR score module that forms part of their CS Model+ software. The module automatically detects anatomical landmarks and allows for automated PAR scoring. It has been reported that PAR scores derived from automated methods are both valid and reliable.14 Nevertheless, the conventional PAR scoring method was more time efficient. However, this may change as automated PAR scoring modules are developed further and become more readily available across multiple digital orthodontic systems.
Virtual set-ups
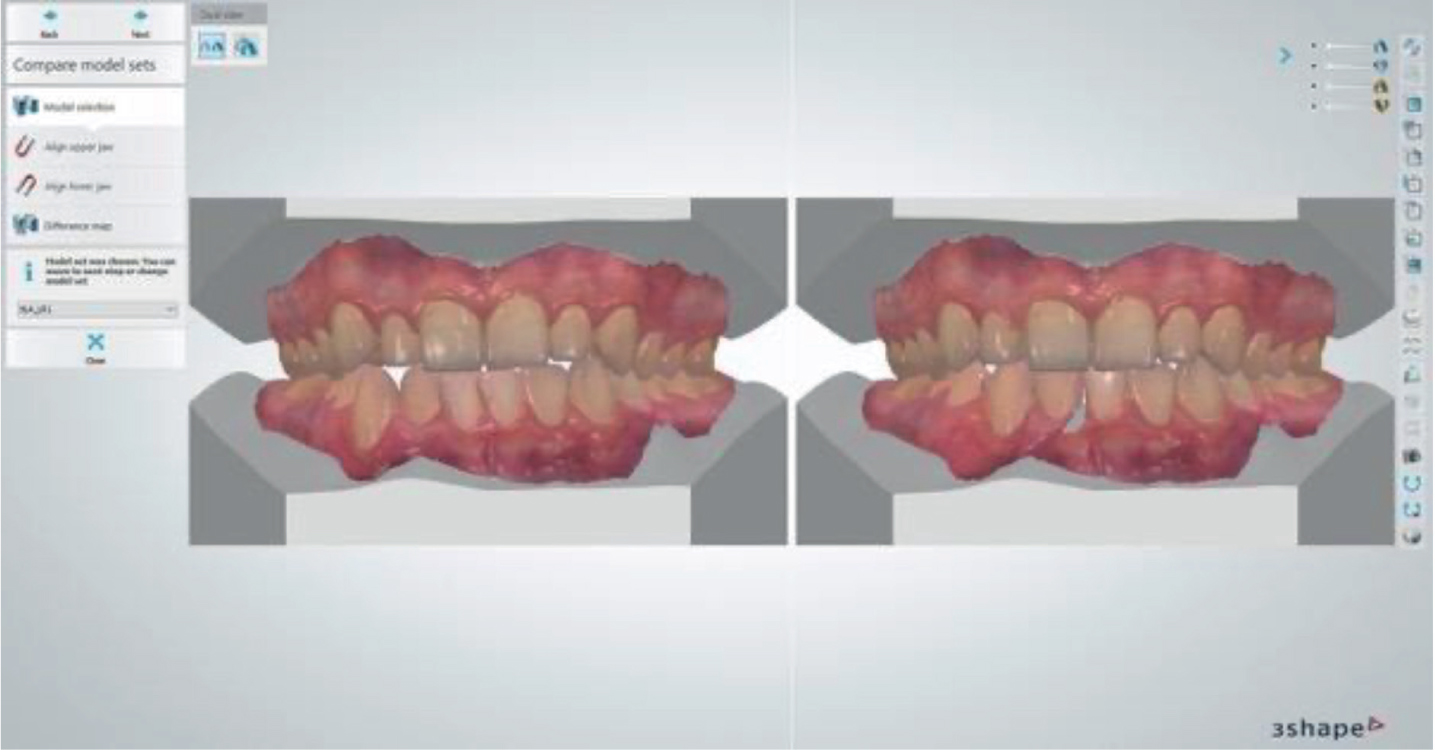
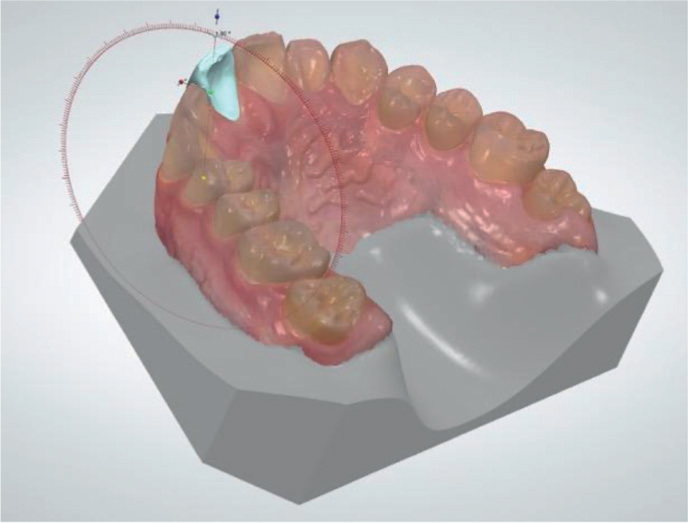
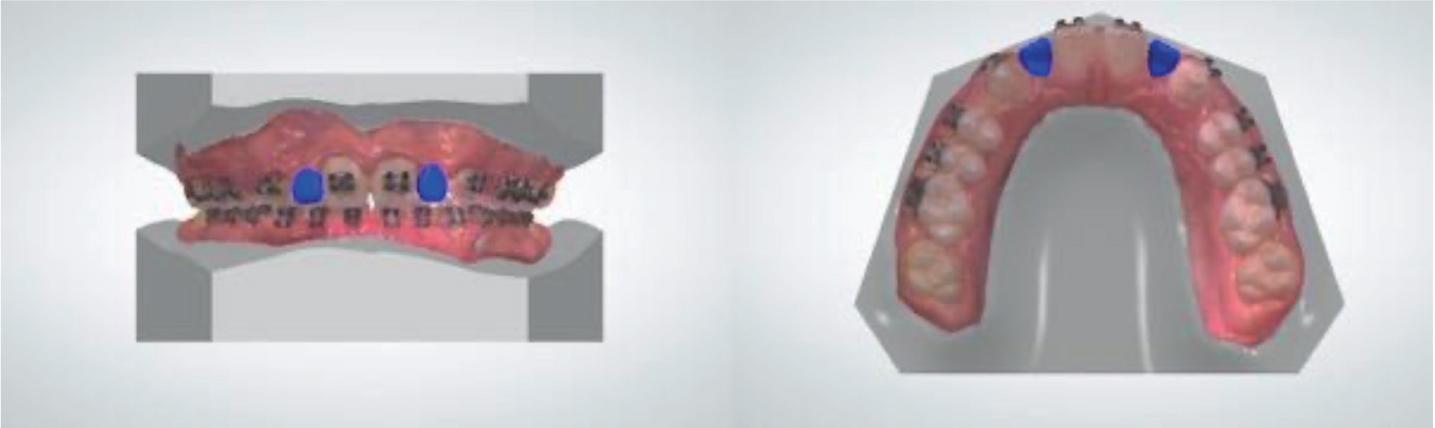
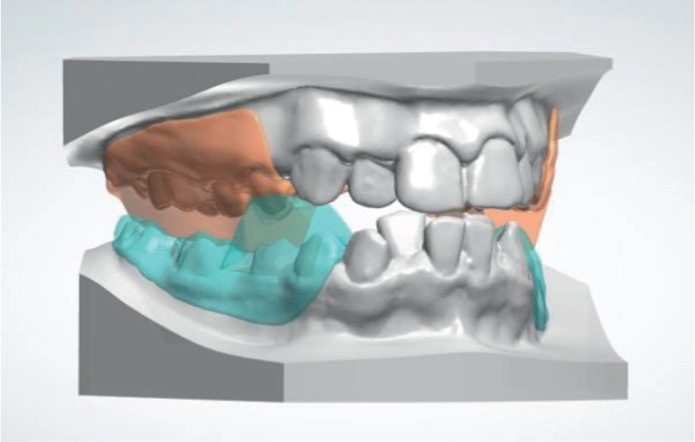
Virtual set-ups can be used to aid diagnosis and treatment planning. They can also be shared with the patient (Figure 5) to improve communication, manage expectations and assist informed consent.3,15 The advances in clinical imaging have allowed clinicians and technicians to use virtual treatment planning software to help determine treatment outcomes and case objectives. 3D virtual setups are created by segmenting individual teeth from a digital model and moving them into the desired position (Figure 6). Multiple treatment plan options can be compared virtually, such as space opening for prosthetic replacement of missing teeth versus orthodontic space closure (Figure 7), or extraction versus non-extraction. Furthermore, the effect of different amounts of inter-proximal reduction can also be more easily visualised.
Figure 5. Treatment plan comparison. The pre-treatment study models (left) and predicted post-treatment outcome following extraction of LR1 (right).Figure 6. Moving a segmented tooth into its desired position using the virtual setup module of the 3Shape OrthoAnalyzer.Figure 7. The planned placement of a prosthetic UL2 and UR2 in the virtual setup module of the 3Shape OrthoAnalyzer.
Arch analyses
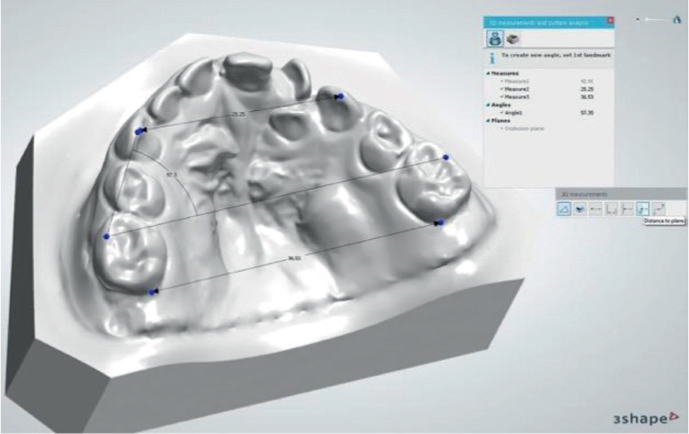
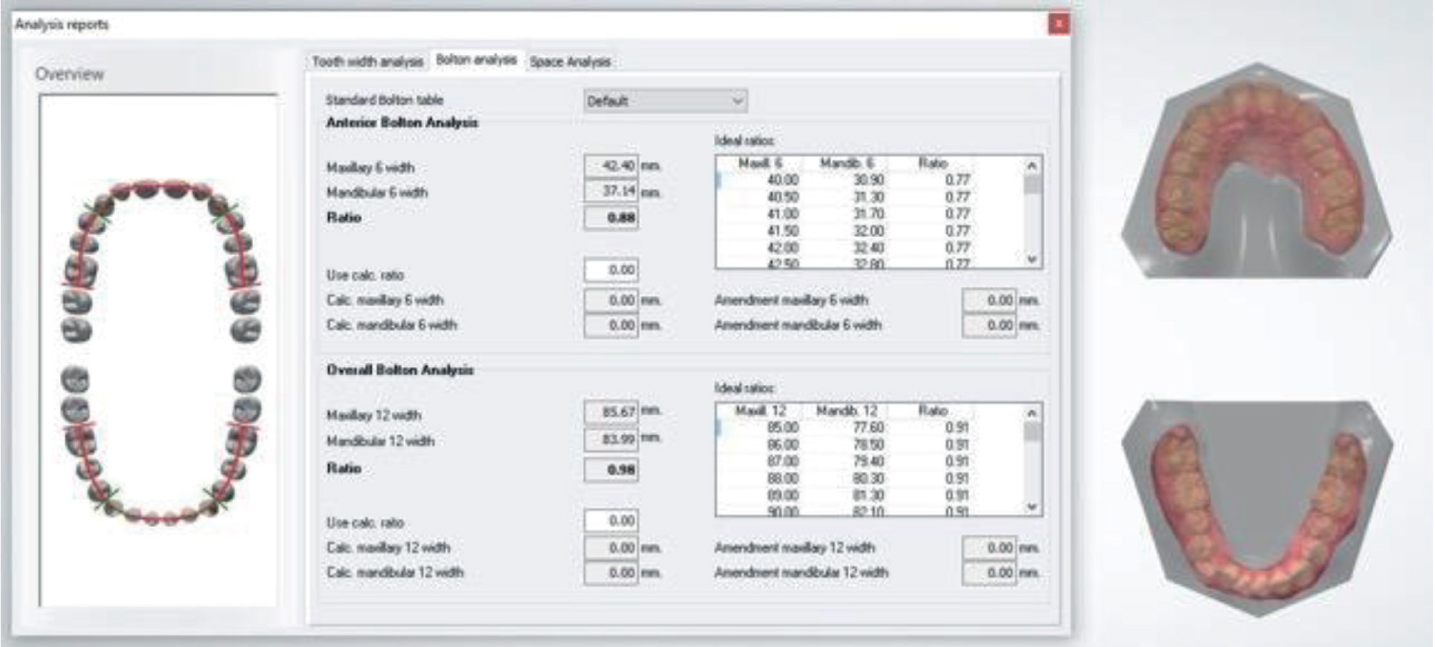
A number of digital orthodontic systems, such as 3Shape Ortho System or Carestream Dental CS Model+ software, feature analysis workflows. These modelling systems can be used to measure angular and linear distances such as: arch widths, midline discrepancy, overjet and overbite as well as carry out space and Bolton tooth-size analysis (Figures 8 and 9). These various workflows have been evaluated and deemed to be as accurate as plaster model analysis and therefore suitable for clinical use.8, 16
Figure 8. Linear measurement tool capturing the inter-molar, inter-canine, disto-palatal and side angle.Figure 9. 3Shape OrthoAnalyzer Bolton Analysis module and a digital pre-treatment orthodontic study model.
Cephalometric analyses
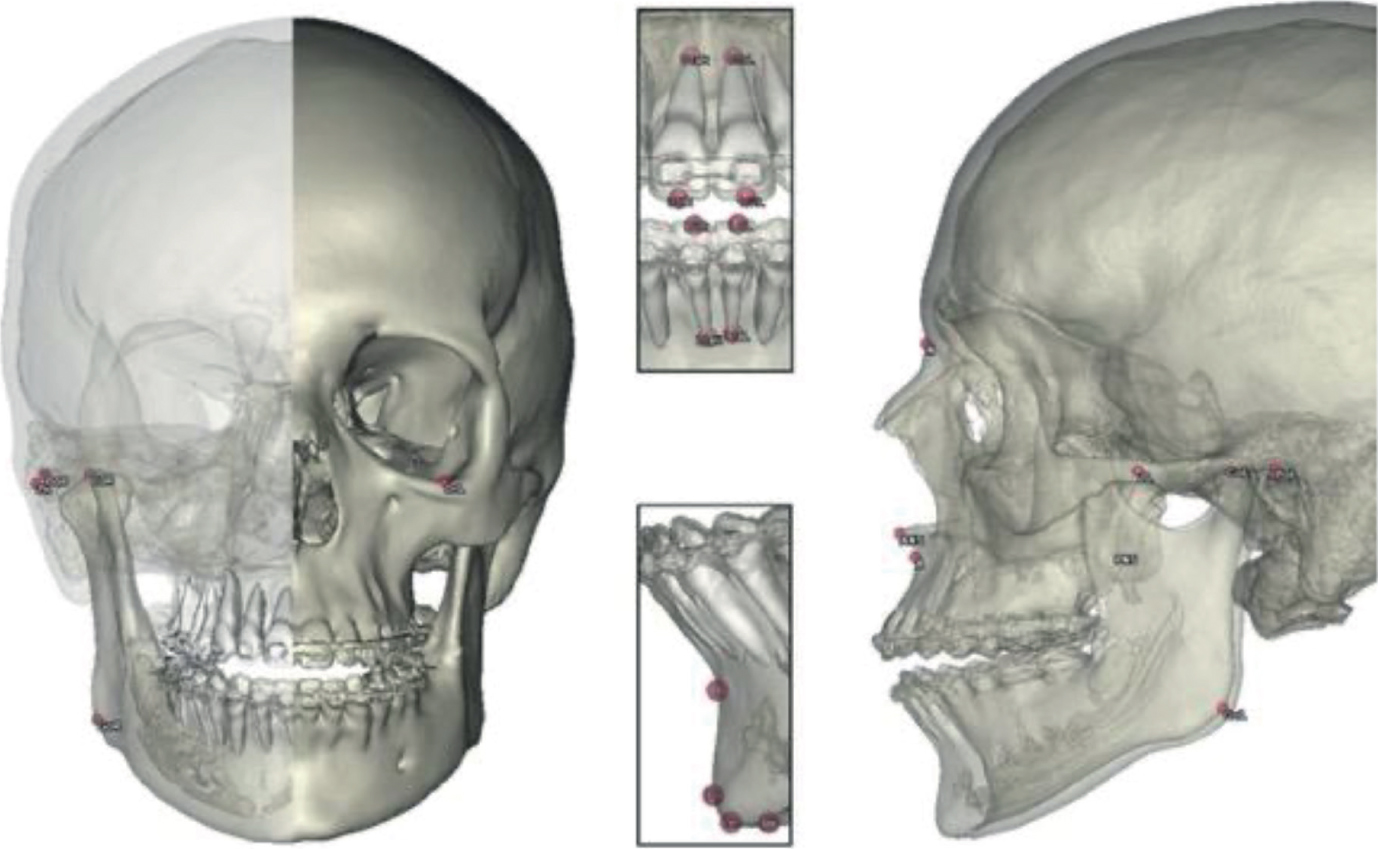
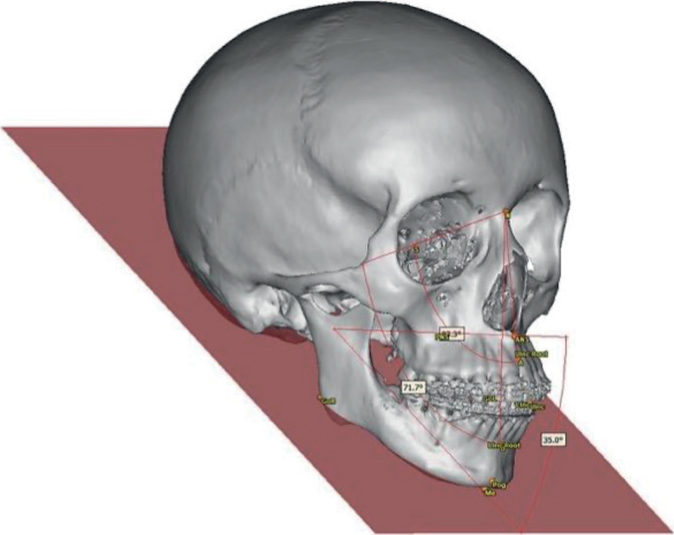
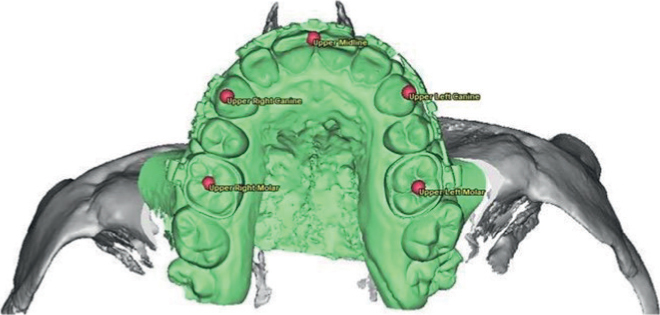
Aside from arch analysis there are also computer programs able to assist with cephalometric analysis. One such cephalometric tracing programme, is OPAL, which has been available for many years and uses a simple 2D lateral cephalogram. More recently, computer-assisted digital cephalometric analysis systems have become available which allow the user to manually identify anatomical regions of interest (for example the anterior nasal spine, nasion or menton) on a digital model typically reconstructed from a cone-beam computed tomography (CBCT) scan (Figure 10). The computer software is then able to determine the cephalometric measurements (Figure 11). The need to plot the landmarks manually on the 3D virtual model is unlikely to improve efficiency but registration of the landmarks using the cross sectional slices (such as sagittal, coronal and axial planes) of the CBCT scan alongside a 3D virtual model could improve accuracy. This computer-assisted process is typically used in the stages of virtual surgical planning for joint orthodontic/orthognathic cases and forms part of the surgical workflow. Occlusal points are also plotted and used to track the distance/degree of intra-operative maxillary and mandibular movement during virtual surgical planning. The occlusal points commonly identified in our department are illustrated in Figure 12. The analysis can then be saved and stored within the digital filing system, where it may be recalled for auditing post-surgical results or for research purposes.
Figure 10. Manually plotted cephalometric points registered on a 3D reconstruction from cone-beam computed tomography.Figure 11. Computer generated Eastman cephalometric measurements taken from a 3D reconstruction from cone-beam computed tomography.Figure 12. Occlusal registration points plotted on the upper midline, UL3, UL6, UR3 and UR6. These points are used to track the distance/degrees of intra-operative maxillary and mandibular movement. The movements are logged in an ‘overview table’ during orthognathic virtual surgical planning.
Removable appliances
To date, the application of 3D technology to the production of removable/functional orthodontic appliances has largely been limited to clear retainers and aligners. While it is possible to produce a customised appliance within a digital platform by allowing the user to have accurate control of material thickness and design precision (Figure 13), the present techniques used to incorporate orthodontic wires into digitally designed appliances are slow and expensive4.
Figure 13. Digitally designed custom twin block appliance.
Aligners
Recently the demand for orthodontic appliances that are more aesthetically pleasing than conventional fixed appliances has increased.17 Clear aligner technology was initially introduced to treat minor discrepancies in tooth position, although some aligner systems now claim to target complex malocclusions. Clear aligner technology has naturally evolved from Dr H Kesling's tooth positioner appliance, first used in 1945.18 Recent developments in transparent thermoplastic materials and digital technology involving tooth movement simulation, CAD/CAM and 3D printing have resulted in increased availability, rendering them an effective system for tooth alignment in a variety of malocclusions.18 Despite increased availability, clinicians must still rely on their own experience to navigate the treatment planning process, and the ultimate responsibility for the treatment lies with the prescribing clinician rather than a third party digital laboratory.
Retainers
Orthodontic retention is one of the most important phases of orthodontic treatment. Without retention, orthodontic treatment is likely to suffer a degree of relapse19. Orthodontic retainers are commonly fabricated over a gypsum dental cast using transparent thermoplastic materials and vacuum forming technology, but they can now either be made using a 3D printed model, or directly 3D printed without the need for models. At present there are a finite number of clear and aesthetic curable resins deemed to be both biocompatible and capable of withstanding the natural forces of occlusion. A study conducted on the use of ultraviolet-sensitive polymethyl methacrylate as a printable retainer material, anecdotally considered it to be much more rigid than the traditional thermoforming materials.19 This increased rigidity would likely cause issues in the clinic, particularly with respect to undercuts in the dentition. Limited research has been carried out on the suitability and accuracy of 3D printed retainers in the longer term. Although one recent study reported that in the short-term there was little difference between commercially available and in-house printed clear aligners, further development in printing materials is needed before 3D printed orthodontic retainers supersede the conventional thermoformed retainer for longer term use. Moreover, the cost pressure associated with directly 3D printing orthodontic retainers must decrease if the workflow is to become commercially viable for clinicians and laboratories alike.
Computer-aided indirect bonding
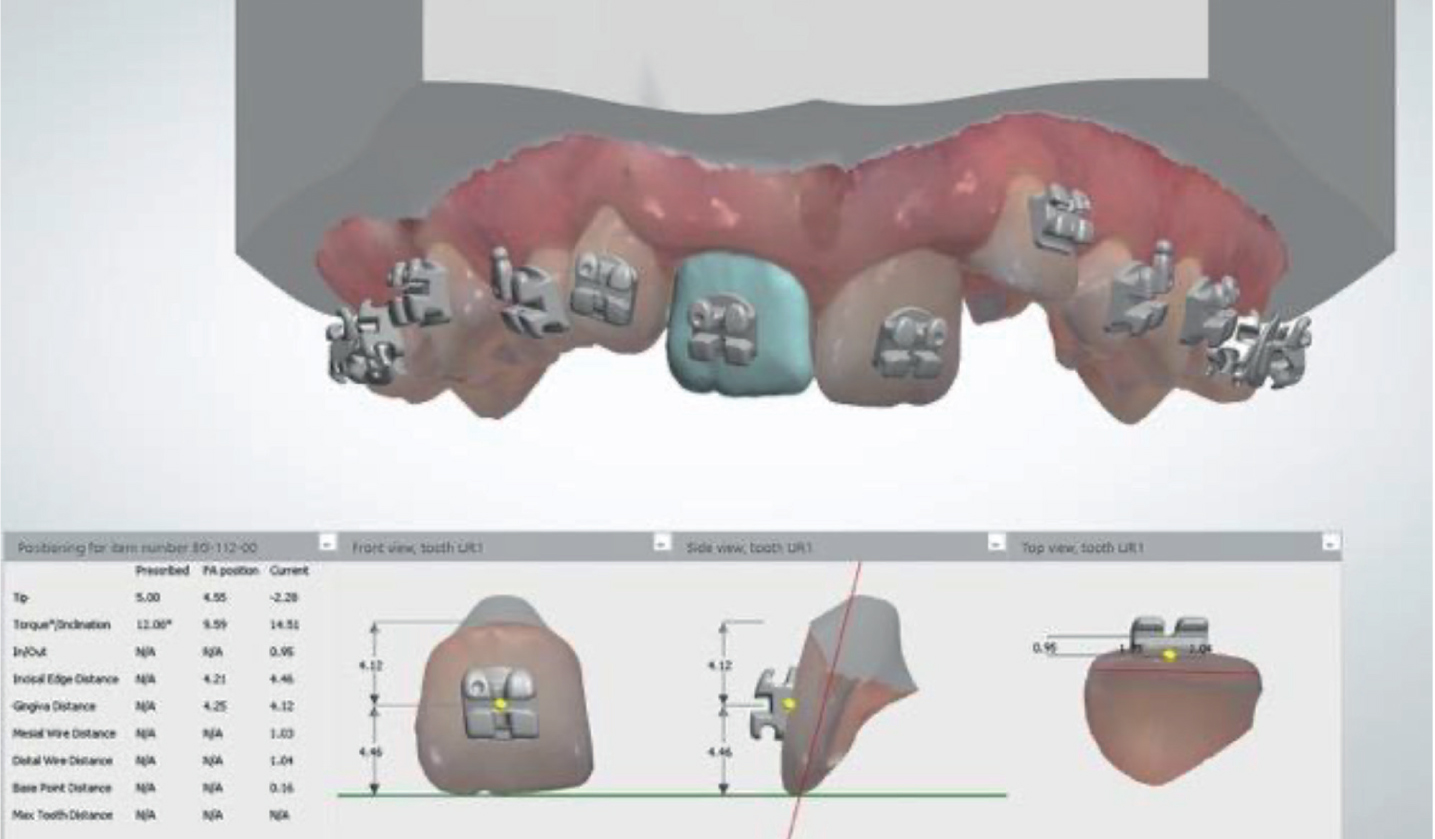
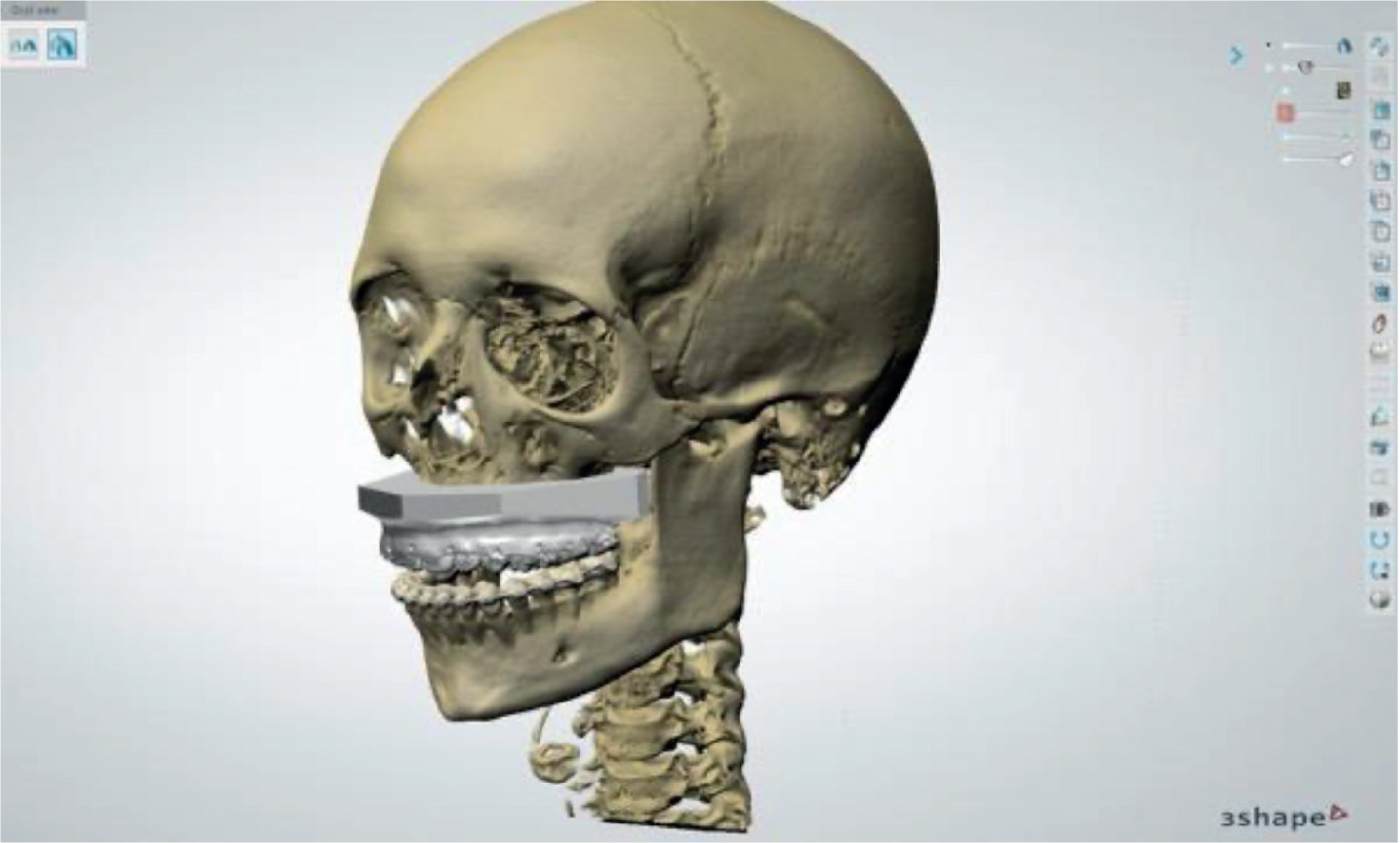
Indirect bonding is a process that allows the clinician to introduce a full arch of brackets onto the dentition at once. Traditionally, this is achieved by obtaining a stone model of the patient's dentition and correctly positioning the brackets onto the labial surfaces according to clinical height and angulation. Once the ideal bracket position has been obtained and the brackets fixed to the model, a flexible custom transfer tray is formed over the stone model and attached brackets. Once removed from the model, adhesive is applied to the bracket bases and the tray introduced onto the previously etched and dried teeth in the patient's mouth, where curing takes place20. The tray is then peeled out of the mouth, leaving the brackets in place on the teeth. Previous studies have found that indirect bonding improves the positioning and bonding of orthodontic appliances.14,21 However, it has been reported that patients who have undergone treatment by means of computer aided indirect bonding were found to have no significant difference in treatment outcome compared to those who had been treated using conventional methods.22 As intra-oral scans and 3D models are increasingly being used for diagnosis and treatment planning, a new form of indirect bonding has emerged whereby the brackets are positioned virtually onto each tooth and an indirect bonding tray is digitally designed and 3D printed in a flexible, transparent biocompatible material (Figure 14). The orthodontic brackets are then manually loaded into the 3D printed transfer tray and bonded to the teeth, as in the conventional method. The digital workflow also allows the operator to import the patient's CT or CBCT image and overlay this onto the digital models (Figure 15). Using an extensive bracket library within the 3D software, the user can select, place and determine an accurate bracket position while viewing the dental anatomy from all angles at increased magnification. Some software packages will produce an estimated post-treatment outcome for the clinician to review (Figure 16), where final tooth positions can be checked as the digital brackets are placed on the teeth.21,23 It has been reported that clinical chairside time is shorter for computer-aided indirect bonding compared to traditional direct bonding, although the entire computer-aided process (including digital bracket placement) is currently more time consuming than traditional methods.21 The digital indirect bonding technique has been extensively tested against direct bonding for both precision and efficiency. However, research comparing the efficiency of conventional indirect bonding processes with the computer-aided indirect bonding processes is limited. Table 3 illustrates the benefits and drawbacks of computer-aided indirect bonding.
Figure 14. Computer-aided indirect bonding workflow: reviewing the bracket position.Figure 15. Imported 3D reconstruction of computed tomography imaging with digital orthodontic study models superimposed.Figure 16. Computer aided indirect bonding workflow: A comparison between the pre-treatment position and the predicted post-treatment outcome.
Table 3. A summary of the benefits and drawbacks of computer aided indirect bonding.
Benefits
Drawbacks
Reduction in chair time
The digital process is more time consuming than the traditional indirect bonding method
Increased patient comfort
Increased number of immediate bracket bonding failures
Improved precision
An expensive system to implement due to the amount of specialist equipment required
Reduction in number of stages of manufacture associated with traditional indirect bonding methods
Further staff training
On-going licensing costs for software
Customised brackets
One of the more advanced orthodontic applications of CAD/CAM technology is the production of customised brackets. The workflow begins with an intra-oral scan of the patient followed by the segmentation of the individual teeth. This defines their virtual mesio-distal/buccal-lingual boundaries. An ideal arch form and occlusion is then setup virtually by a technologist and then sent to the clinician for approval. Once the treatment plan has been approved, the prescription is sent to a third-party manufacturer where the brackets are then customised. Depending on the clinician's choice of bracket this can be achieved in a number of ways. For example, metal self-ligating brackets are customised by varying the angle and thickness of the bracket base, while metal twin brackets can be customised by ‘precision cutting’ the archwire slots. One such system, the Ormco Insignia allows for limited customisation of ceramic brackets, whereas various lingual appliance systems, such as Incognito, use virtually designed lingual brackets that are 3D printed as wax patterns. These patterns are then invested, burned out and cast using a dental gold alloy.24
Following approval from the clinician, the fabricated customised brackets are positioned in a patient-specific indirect bonding tray designed around the virtual setup. Indirect bonding is then used to place the brackets and ensure the effectiveness of the customised system is maintained.3, 8, 24 The option of using customised wires is also available to the clinician.
Customised arch wire
In the field of customised orthodontic appliances, much of the development has focused on producing customised brackets. However, the introduction of robotics to the digital process in orthodontics has led to the creation of a number of customised arch wire systems. One such system is OraMetrix's SureSmile. This digital orthodontic system, like many others, allows the user to manipulate a set of digital models to plan the case and assess the likely treatment outcomes. Once this has been done the planned treatment can be simulated, and the plan transferred to a ‘wire-bending robot’ that will fabricate the orthodontic arch wires to the geometry of the virtual treatment plan. The same robotic wire bending technique has also been applied to customised lingual orthodontic systems such as the Incognito system. When compared to conventional methods, this technology has been reported to reduce treatment time and improve treatment outcome, although discrepancies in the predicted tooth movement have also been reported, especially with regard to crown torque and tip/rotation movements.3, 25
Customised teeth
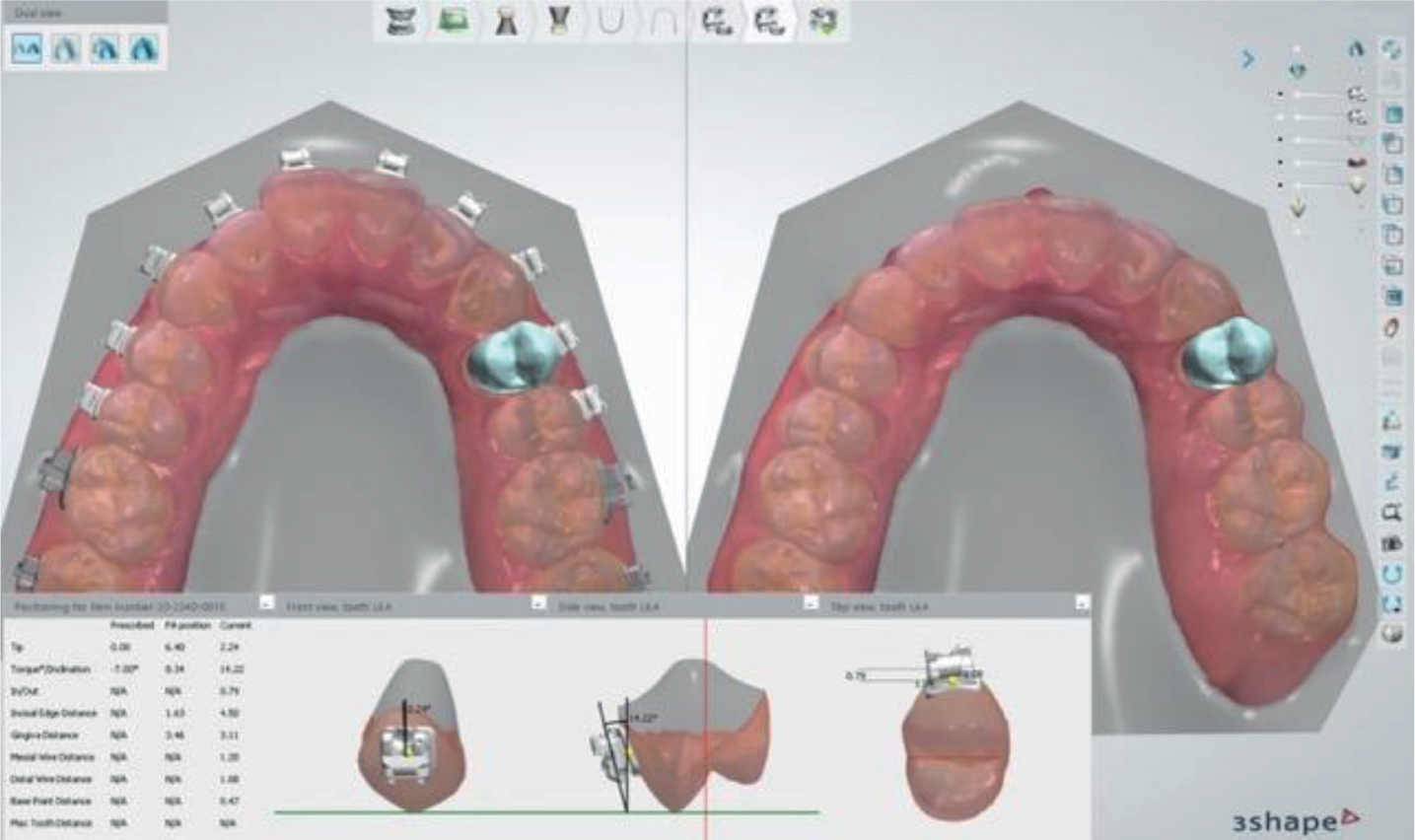
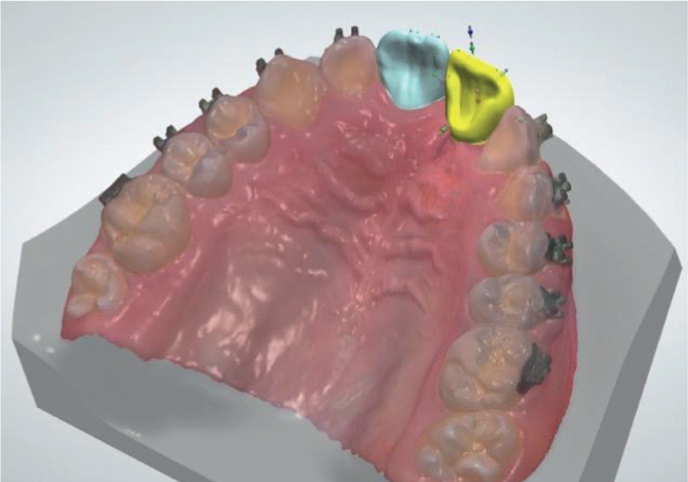
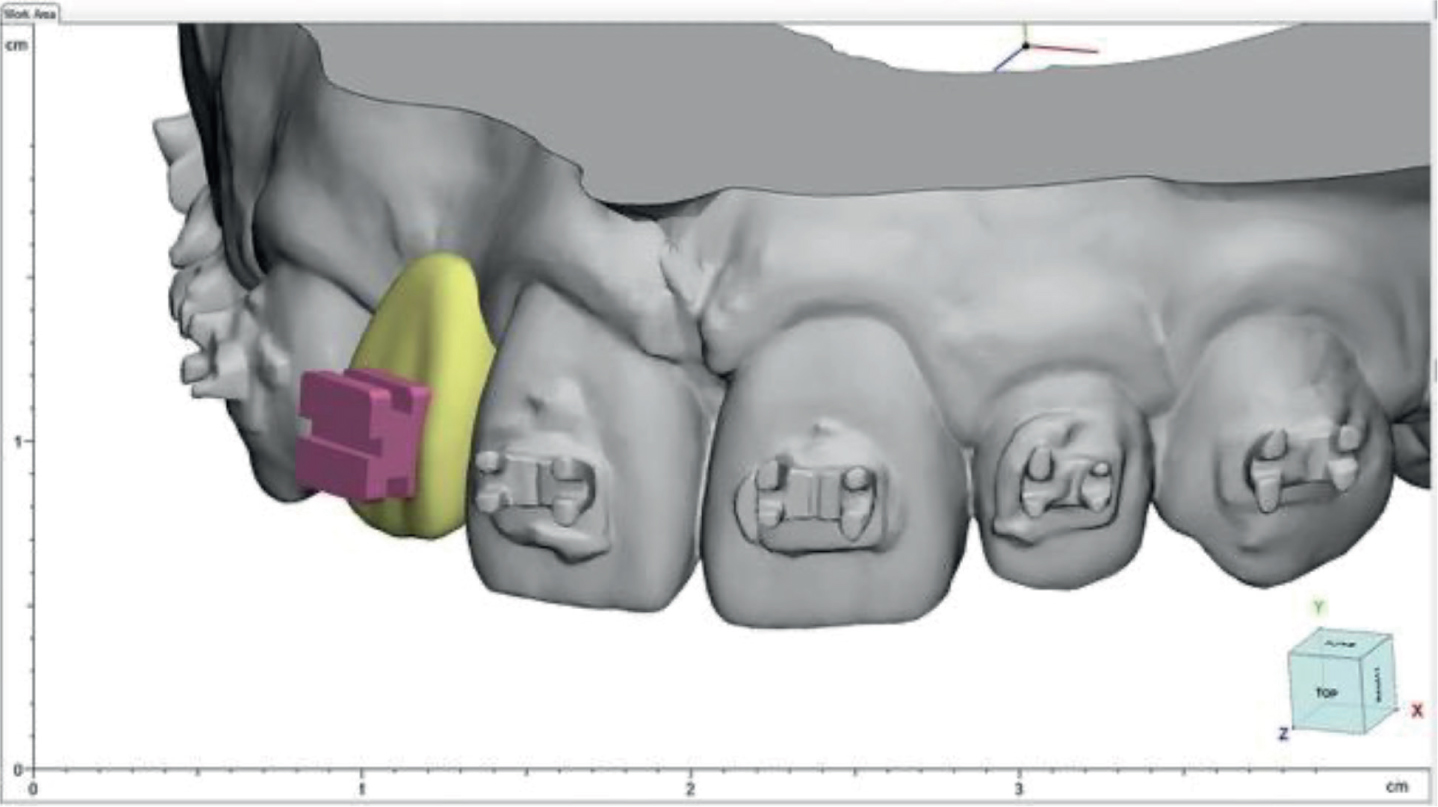
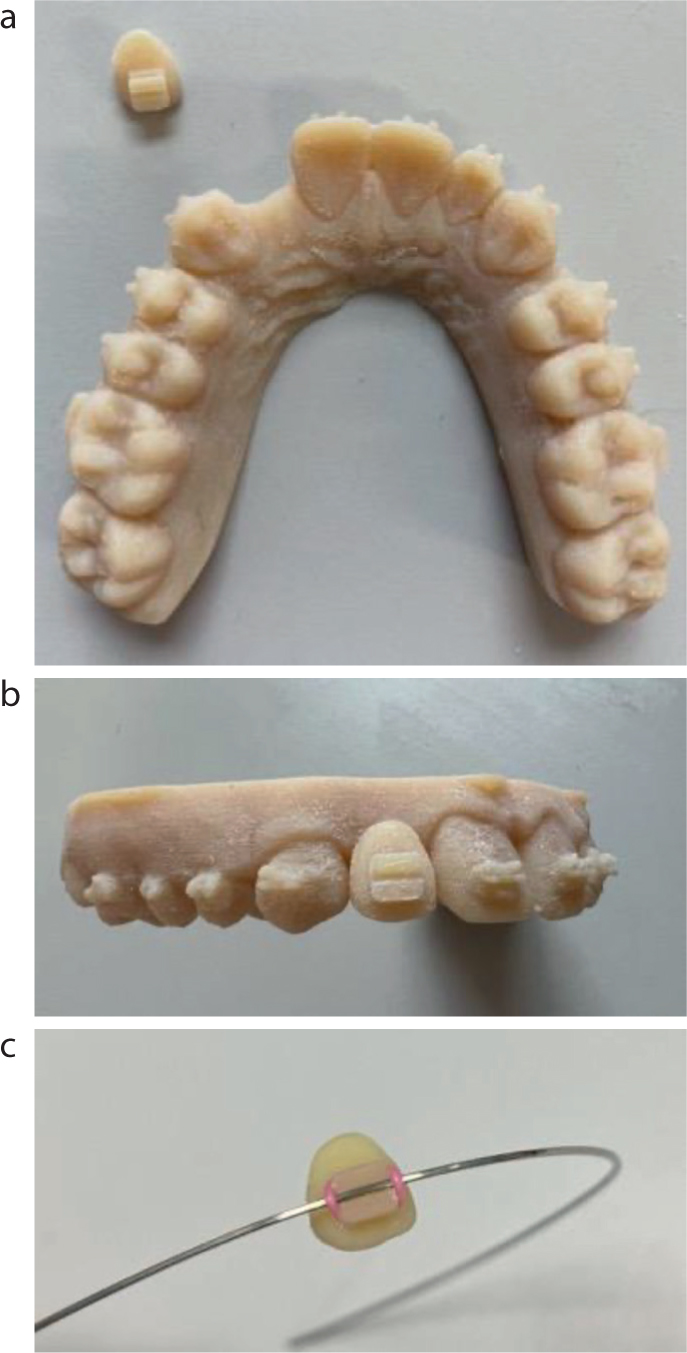
By utilising intra-oral scanning technology, CAD software and 3D printing, it is now possible to digitally design and 3D print customised teeth with an orthodontic bracket in-situ. The current workflow allows the user to load the intra-oral scan and either import a digital stock tooth into the edentulous space (Figure 17) or mirror the desired contralateral tooth into position via the sagittal plane. Once the tooth size has been manipulated and the tooth position approved, an orthodontic bracket that has been specifically designed to be 3D printed in acrylic is then imported. The user is able to place the bracket in the desired position on the tooth (Figure 18) before finally merging the bracket and tooth files and exporting the single digital file to the 3D printer. In this way, a one-piece tooth and bracket can be printed using a coloured (VITA shade A2) biocompatible resin (Figure 19) before being fitted in the mouth.
Figure 17. Importing and manipulating a UL1 digital stock tooth into the edentulous space using the virtual setup module of the 3Shape OrthoAnalyzer software.Figure 18. Positioning the custom orthodontic bracket onto a digital stock tooth.Figure 19. 3D printed ‘tooth and bracket’ in a biocompatible VITA Shade A2 resin and study model.
Conclusions
Digital workflows are increasingly becoming a mainstay of orthodontic practice and have the potential to improve the quality of patient care, reduce treatment times and facilitate more efficient day-to-day working practices. It is important to point out that digital orthodontics requires investment, appropriate training, and evaluation to ensure it achieves its goals. The second article in this two-part series will document the application of digital workflows in joint orthodontic/orthognathic treatment and present clinical cases which have undergone treatment by means of a digital workflow.