Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton 2001. J Rheumatol. 2004; 31::390-392
Thomson W, Barrett JH, Donn R, Pepper L, Kennedy LJ, Ollier WE Juvenile idiopathic arthritis classified by the ILAR criteria: HLA associations in UK patients. Rheumatology (Oxford). 2002; 41:1183-1189
Arvidsson LZ, Fjeld MG, Smith HJ, Flato B, Ogaard B, Larheim TA Craniofacial growth disturbance is related to temporomandibular joint abnormality in patients with juvenile idiopathic arthritis, but normal facial profile was also found at the 27-year follow-up. Scand J Rheumatol. 2010; 39:373-379
Pedersen TK, Jensen JJ, Melsen B, Herlin T Resorption of the temporomandibular condylar bone according to subtypes of juvenile chronic arthritis. J Rheumatol. 2001; 28:2109-2115
Ronning O, Valiaho ML, Laaksonen AL The involvement of the temporomandibular joint in juvenile rheumatoid arthritis. Scand J Rheumatol. 1974; 3:89-96
Hu Y, Billiau AD, Verdonck A, Wouters C, Carels C Variation in dentofacial morphology and occlusion in juvenile idiopathic arthritis subjects: a case-control study. Eur J Orthod. 2009; 31:51-58
Stabrun AE, Larheim TA, Rosler M, Haanaes HR Impaired mandibular function and its possible effect on mandibular growth in juvenile rheumatoid arthritis. Eur J Orthod. 1987; 9:43-50
Walton AG, Welbury RR, Foster HE, Thomason JM Juvenile chronic arthritis: a dental review. Oral Dis. 1999; 5:68-75
Armon K Outcomes for juvenile idiopathic arthritis. Paediatr Child Health. 2014; 24:64-71
Stoll ML Intra-articular corticosteroid injections to the temporomandibular joints are safe and appear to be effective therapy in children with juvenile idiopathic arthritis. J Oral Maxillofacial Surg. 2012; 70:1802-1807
Long AR, Rouster-Stevens KA The role of exercise therapy in the management of juvenile idiopathic arthritis. Curr Opin Rheumatol. 2010; 22:213-217
Minden K, Niewerth M, Listing J, Biedermann T, Schontube M, Zink A Burden and cost of illness in patients with juvenile idiopathic arthritis. Ann Rheum Dis. 2004; 63:836-842
Mercuri LG A rationale for total alloplastic temporomandibular joint reconstruction in the management of idiopathic/progressive condylar resorption. J Oral Maxillofac Surg. 2007; 65:1600-1609
Sidiropoulou-Chatzigianni S, Papadopoulos MA, Kolokithas G Dentoskeletal morphology in children with juvenile idiopathic arthritis compared with healthy children. J Orthod. 2001; 28:53-58
Richmond S, Roberts CT, Andrews M Use of the Index of Orthodontic Treatment Need (IOTN) in assessing the need for orthodontic treatment pre- and post-appliance therapy. Br J Orthod. 1994; 21:175-184
Ringold S, Cron RQ The temporomandibular joint in juvenile idiopathic arthritis: frequently used and frequently arthritic. Pediatr Rheumatol Online J. 2009; 7
Weiss PF, Arabshahi B, Johnson A, Bilaniuk LT, Zarnow D, Cahill AM High prevalence of temporomandibular joint arthritis at disease onset in children with juvenile idiopathic arthritis, as detected by magnetic resonance imaging but not by ultrasound. Arthritis Rheum. 2008; 58:1189-1196
Muller L, Kellenberger CJ, Cannizzaro E, Ettlin D, Schraner T, Bolt IB Early diagnosis of temporomandibular joint involvement in juvenile idiopathic arthritis: a pilot study comparing clinical examination and ultrasound to magnetic resonance imaging. Rheumatology (Oxford). 2009; 48:680-685
Scarfe WC, Farman AG, Sukovic P Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc. 2006; 72:75-80
Scarfe WC, Farman AG What is cone-beam CT and how does it work?. Dent Clin North Am. 2008; 52:707-730
Hatcher DC Operational principles for cone-beam computed tomography. J Am Dent Assoc. 2010; 141
Hilgers ML, Scarfe WC, Scheetz JP, Farman AG Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am J Orthod Dentofacial Orthop. 2005; 128:803-811
Krishnamoorthy B, Mamatha N, Kumar VA TMJ imaging by CBCT: current scenario. Ann Maxillofac Surg. 2013; 3:80-83
Tvrdy P Methods of imaging in the diagnosis of temporomandibular joint disorders. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2007; 151:133-136
Kopp S, Carlsson GE, Haraldson T, Wenneberg B Long-term effect of intra-articular injections of sodium hyaluronate and corticosteroid on temporomandibular joint arthritis. J Oral Maxillofac Surg. 1987; 45:(11)929-935
Martini G, Bacciliero U, Tregnaghi A, Montesco MC, Zulian F Isolated temporomandibular synovitis as unique presentation of juvenile idiopathic arthritis. J Rheumatol. 2001; 28:1689-1692
Srivastava R, Jyoti B, Devi P Oral splint for temporomandibular joint disorders with revolutionary fluid system. Dent Res J (Isfahan). 2013; 10:307-313
The aim of the present study was to describe a case with juvenile idiopathic arthritis (JIA) with bilateral temporomandibular joint (TMJ) involvement and long-term facial growth implications, requiring complex surgical treatment and multidisciplinary teams.
CPD/Clinical Relevance: Consideration was given to TMJ replacement with alloplastic graft, however, the final management strategy involved bimaxillary surgery.
Article
Juvenile idiopathic arthritis (JIA) is the most common type of arthritis that affects children, with a reported prevalence rate of 0.07–4.01 per 1000 children. The annual incidence is reported as 0.008–0.226 per 1000 children.1 Previous published literature discusses the effects and morbidity of JIA but its effects on facial structures and oral function is poorly understood.
The precise aetiological factors are not known yet, however, many factors can be implicated separately or concurrently, such as auto-immunological factors, viral infections, traumatic episodes, psychological factors and genetic factors.2
There are seven main types of JIA, as specified by Petty et al:3
Oligoarthritis, the most prevalent form of JIA, is defined as arthritis affecting 1–4 joints during the first 6 months of disease. Two subcategories are recognized:
Persistent oligoarthritis, affecting no more than four joints throughout the disease course; and
Extended oligoarthritis, affecting a total of more than four joints after the first 6 months of disease.4
The implications of JIA on extra-oral and intra-oral features are not noticeable if the TMJs are not affected. Arvidsson et al5 showed that 70% of patients with JIA and TMJ involvement had some form of craniofacial growth disturbance. Pedersen et al described facial asymmetries as a common presenting feature in patients diagnosed with this condition, secondary to an unequal rate of condylar destruction or unilateral activity6
Involvement of temporomandibular joints (TMJ) is not uncommon in patients with JIA, usually resulting in long-term implications on facial growth, especially on mandibular growth.
Condylar lesions have been observed in 22–55% of affected children, with the disparity in figures being due to the type of subjects studied or radiographic technique on which it was based.7
Hu et al also showed that effects are not only limited to extra-oral features but can also affect intra-oral features, with certain occlusal features being more prevalent in affected patients.8 The typical extra- and intra-oral features are shown in Table 1 with an anterior open bite being a classical presenting feature.9
Skeletal
Soft Tissues
Intra-oral Features
Class II skeletal base with a retrognathic and micrognathic mandible
Two of the main dentofacial comorbidities are the limited mouth opening and speech difficulties, with the majority of patients resorting to a softer diet, with the former comorbidity leading to an impediment in good oral hygiene maintenance.10
The management of JIA
The management of JIA can be classified into the three main modalities:
Medical;
Rehabilitative; and
Surgical.
Medical management
Drugs used for the treatment of adult arthritis and by extension JIA have undergone a phenomenal revolution in the last 20 years. The advent of biologic therapy has raised the possibility of remission induction and maybe even cure. Only 20 years ago it was uncommon for children with JIA to be treated with methotrexate, and they were frequently only given non-steroidal anti-inflammatories to control pain, with the hope that the disease would settle on its own without progressing to medication with potentially more serious side-effects.
This approach has been shown to be flawed, since it is almost inevitable that poorly controlled disease leads to long-term joint destruction, which cannot be reversed.11 In addition, the affected child's life is blighted with pain, stiffness, lack of mobility, consequent loss of education and social interaction. The condition is nowadays treated more aggressively.
This includes NSAIDs and intra-articular corticosteroid injections to affected joints, or systemic steroids for polyarticular disease. Intra-articular steroid injections to the TMJ were thought to be damaging and therefore not routinely used. This practice has changed more recently.12 Oral methotrexate at a dose of 7.5–15 mg/m2 to a maximum of 20 mg/m2 per week is the norm, usually given by subcutaneous injection as the bioavailability (and therefore effectiveness) is superior to oral administration. If there is failure to control the disease at 3 months on methotrexate, treatment is progressed to biologic therapy early (NICE approval 2015 for Etanercept, Adalimumab, Abatacept and Tocilizumab, dependent on type of JIA and age).
Rehabilitation
Literature substantiates the suboptimal physical activity levels of patients diagnosed with JIA compared to unaffected peers.13 This treatment modality allows assessment of motion and strength of the main muscle groups, posture and range of movement. Interventions would therefore be personalized to the individual. Common interventions include strengthening exercises, posture education, advice on appropriate recreational exercise and referral to other specialties if needed. The cost implications were described by Minden et al,14 and could range from £1299 (1,500 euros) per patient per year diagnosed with active arthritis enthesitis to £1473 (17,000 euros) per patient per year diagnosed with seropositive polyarthritis.
Surgical management
General maxillofacial surgical correction of skeletal abnormalities of mandibular aetiology include:
Sagittal split osteotomy;
Vertical split osteotomy (previously referred to as vertical subsigmoid osteotomy);
Genioplasty;
Distraction osteogenesis; and
Alloplastic TMJ reconstruction.
Maxillary correction usually includes, LeFort I osteotomy and surgically-assisted rapid palatal expansion.
In cases of JIA with TMJ involvement, the most contemporaneous methodology involves TMJ reconstruction with alloplastic joints,15 however, all surgical options should be considered and the final clinical decisions should be made on an individual basis.
The aim of this article is to present a case report presenting with more expressive forms of juvenile idiopathic arthritis with long-term facial growth implications, requiring complex surgical treatment involving multidisciplinary teams. This article also reviews the current literature and contemporary management of similar cases.
Case 1
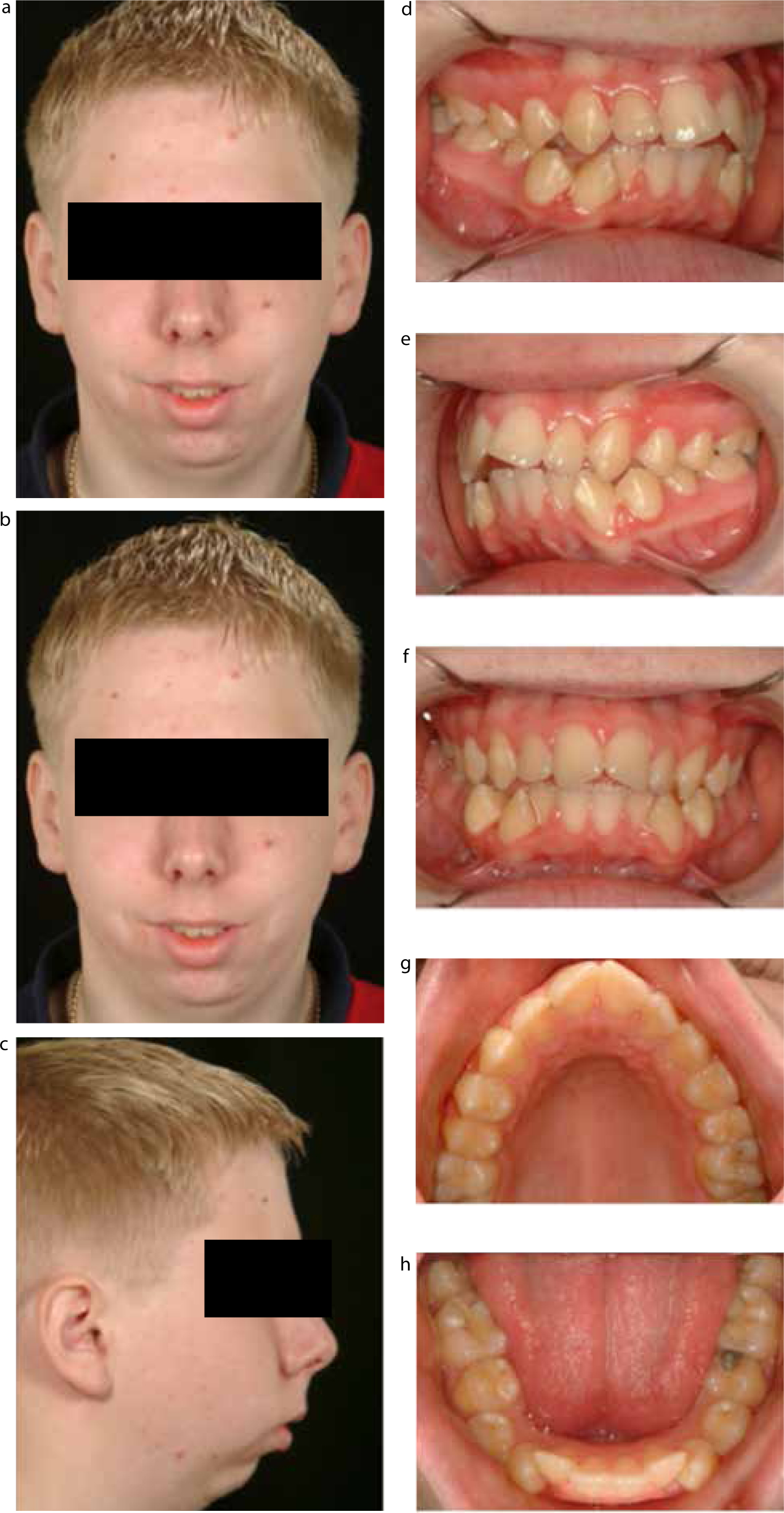
A 13-year-old Caucasian male, LL, was referred by a consultant paediatric rheumatologist with concerns relating principally to his small mandible with no marked functional problems (Figure 1 a–h).
Figure 1.
(a-h) Extra and intra-oral clinical photographs at presentation.
LL had a known medical history of extended oligoarthritis, however, had no known drug allergies. Past drug history included a weekly regimen of 15 mg/m2 methotrexate, which was continued over three years between the ages of 13 and 16. It was tapered gradually with a monthly reduction of 2.5 mg/m2 to monitor any recurring symptoms of arthritis in any of his joints during this reduction phase.
LL was a regular dental attendee to his general dental practitioner and his oral hygiene was fair but needed improving. Extra-oral clinical examination revealed a severe Class II skeletal base with increased vertical proportions, however, with no apparent facial asymmetry.
Upper and lower lips were incompetent. No abnormalities were detected with tongue size and/or morphology and the swallowing pattern was normal. He had no known habits. Intra-oral clinical examination revealed all teeth were present, with the lower and upper labial segment being moderately crowded and proclined. The lower canines were mesio-labially rotated (Figure 1d–h). The buccal segment relationships were Class I bilaterally and the upper centreline was shifted to the left compared to its soft tissue counterparts by approximately 3 mm.
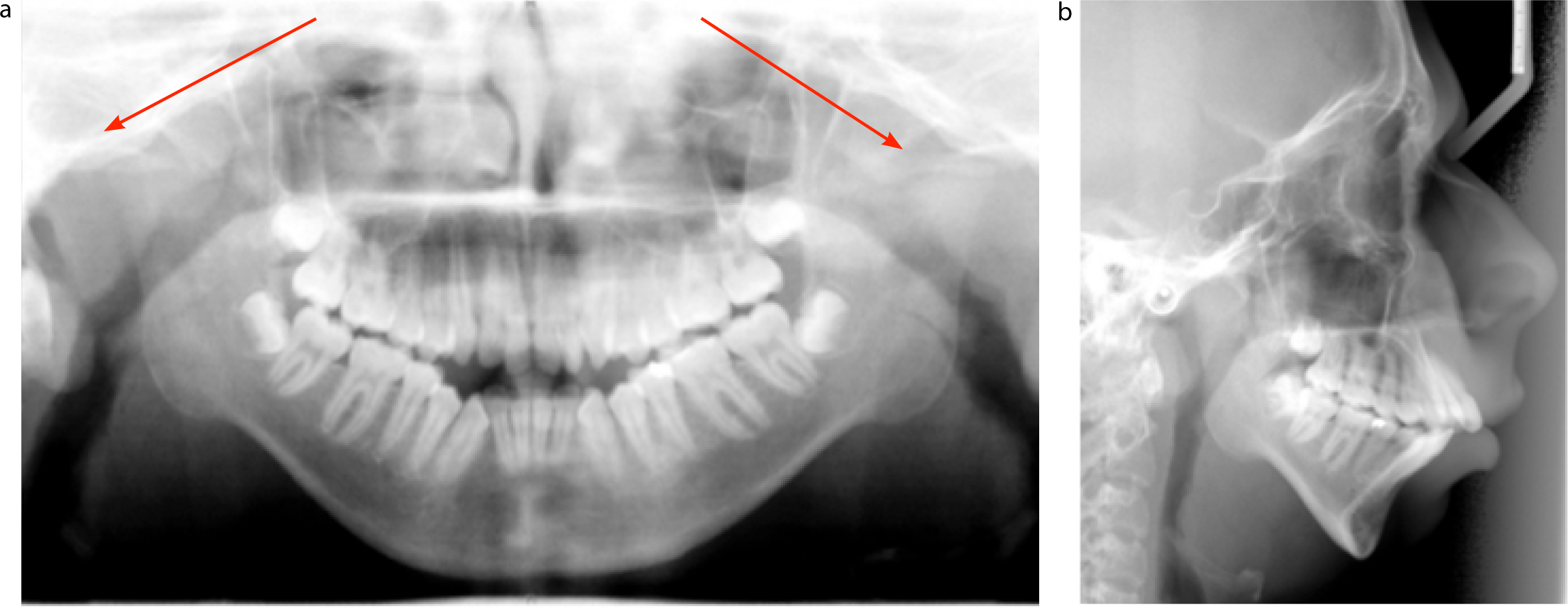
The initial radiological investigation consisted of a dental panoramic tomograph (DPT) and a lateral cephalogram (LC). The DPT confirmed complete resorption of both right and left condyles, whilst the lateral cephalogram confirmed the clinical findings of a skeletal Class II base, increased vertical proportions, with a predominant posterior growth rotation type of facial growth (Figure 2a and b). This is in line with the findings of Sidiropoulou-Chatzigianni et al.16
Skeletal Class II base with mandibular retrognathia;
Increased vertical proportions;
Lip seal was incompetent;
Bimaxillary proclination;
An anterior open bite; and
An increased overjet, which is the horizontal overlap between the top and bottom anterior teeth.
This case was classified as having a dental health component of 5a with an aesthetic component of 9 on the Index of Treatment Need (IOTN).17
Severe skeletal cases are usually managed with one of four treatment modalities: no treatment and regular monitoring; growth modification with removable orthodontic appliances that stimulate mandibular growth through muscle and fascial stretching; orthodontic treatment only with fixed appliances to camouflage the malocclusion; and orthognathic treatment involving both orthodontic and surgical treatment.
In this case, LL was referred to a Multidisciplinary Clinic and the following were specified as part of the overall plan:
Improvement of oral hygiene;
Monitoring of growth with yearly review appointments;
Regular review by the rheumatology team to monitor efficacy of treatment;
Forward sliding genioplasty for immediate improvement of overall aesthetics; and
Referral to a craniofacial centre for innovative and expert advice by a craniofacial team.
The active phase of treatment consisted of extractions of lower first premolars to relieve crowding and allow pre-surgical decompensation utilizing pre-adjusted edgewise appliances with an MBT prescription in a 0.022” x 0.028” bracket slot, Victory series® (3M Unitek, UK). Computerized tomography (CT) of the head allowed precise localization of the lingula and assisted in planning the access for bimaxillary surgery. The main aim of treatment was to correct the retrognathic profile due to a Class II skeletal pattern and closure of anterior open bite, post-surgical orthodontic treatment and retention with removable appliances worn at night-time long term.
Discussion
LL's case of JIA with severe TMJ involvement has been described resulting in significant oral function consequences, requiring a multidisciplinary approach. The patient was classically under the care of a paediatric rheumatology team from the start, receiving continuous active management to control the disease and attempt to induce arthritis remission.
Ringold and Cron outline the reasons for the extensive damage usually seen on TMJs of affected patients, with the main reasons being the anatomical position of the growth centre in the condyle, which is susceptible to damage during inflammation or trauma and the frequent use of this joint, which can amount to 2,000
History-taking and clinical examination are unreliable methods in detecting TMJ involvement in patients with JIA, making radiographic imaging the sole method of investigation available for these patients. Clinical findings could include a history of pain, limited mouth opening and asymmetrical mouth opening.
Dental panoramic tomogram (DPT) (also referred to as orthopantomogram, OPG), ultrasound (US), computed tomography (CT) and magnetic resonance imaging (MRI) have all been described in the literature as reliable investigations to detect the extent of condylar damage and for treatment planning. In a recent study by Weiss et al, MRI and US were compared for sensitivity and specificity and MRI was shown to be a superior investigation to US as the latter can only reliably examine the lateral aspect of the joint.19 In addition, US investigations are not appropriate if there are two dense cortical surfaces in close proximity, and Müller et al proved this in a pilot study showing US as the least reliable investigatory technique.20
Computerized tomography remains the gold standard technique and its applications in the dental setting are well documented.21 Scarfe and Hatcher accurately described the clinical applications and operational procedures in the literature, respectively,22,23 whilst Hilgers et al reported the precision of this technique in measuring linear parameters in temporomandibular joints.24 Krishnamoorthy et al describe computed beam CT (CBCT) as a diagnostic tool with relatively low-dose high-spatial-resolution characteristics.25
Radionuclide imaging has advanced significantly since first introduced in the 1950s and has been used ever since for diagnostic purposes.26 The best category of nuclide imaging devices for TMJ is Single Photon Emission Computed Tomography (SPECT) due to the joint anatomy. This nuclear imaging technique has a high sensitivity, however, specificity is very low, resulting in numerous false positive results, rendering it useful as a screening method only.27
LL was initially managed with a medical approach, but the control of his condition was suboptimal. In general, local intra-articular steroid injections have been shown to be effective, with a minor risk of adverse effects,28 even when accompanied by a synovectomy as reported by Martini et al.29
Medical and/or rehabilitative approaches fail to address the extra- and intra-oral features that most cases of JIA present with, including the case presented in this article.
In LL's case, the options of treatment included: ‘TMJ unloading’ with splint therapy, orthodontics only, orthodontics and orthoganthic surgery or orthoganthic surgery only.
Splint therapy for ‘unloading’ or ‘calibration’ of the occlusion would be one of the initial considerations to alleviate TMJ discomfort. Srivastava et al and Gnanashanmugham et al describe this type of intervention and report on a successfully treated case, respectively.30,31 This intervention was not considered in LL's case as his main complaint was not a functional one and presented with no TMJ dysfunction.
Orthodontic camouflage with extractions of upper and lower first premolars, followed by upper and lower fixed appliances to improve the presenting anterior open bite, could have been considered as a treatment modality but this approach would not have addressed the condylar resorption and the resulting Class II skeletal base. The advantages of such an approach on the other hand would have been a less invasive treatment. However, LL was mostly concerned with his extra-oral appearance.
There were three main surgical options available to our patient:
Fixed appliance therapy in combination with bimaxillary surgery;
Distraction osteogenesis followed by orthognathic surgery;
Alloplastic TMJ replacement.
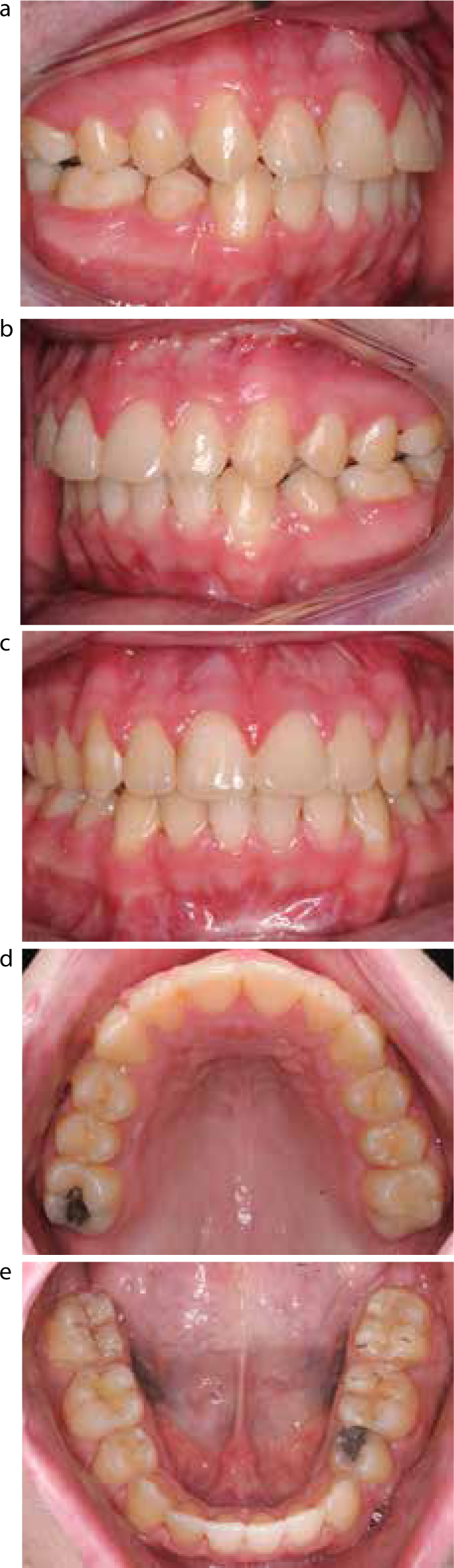
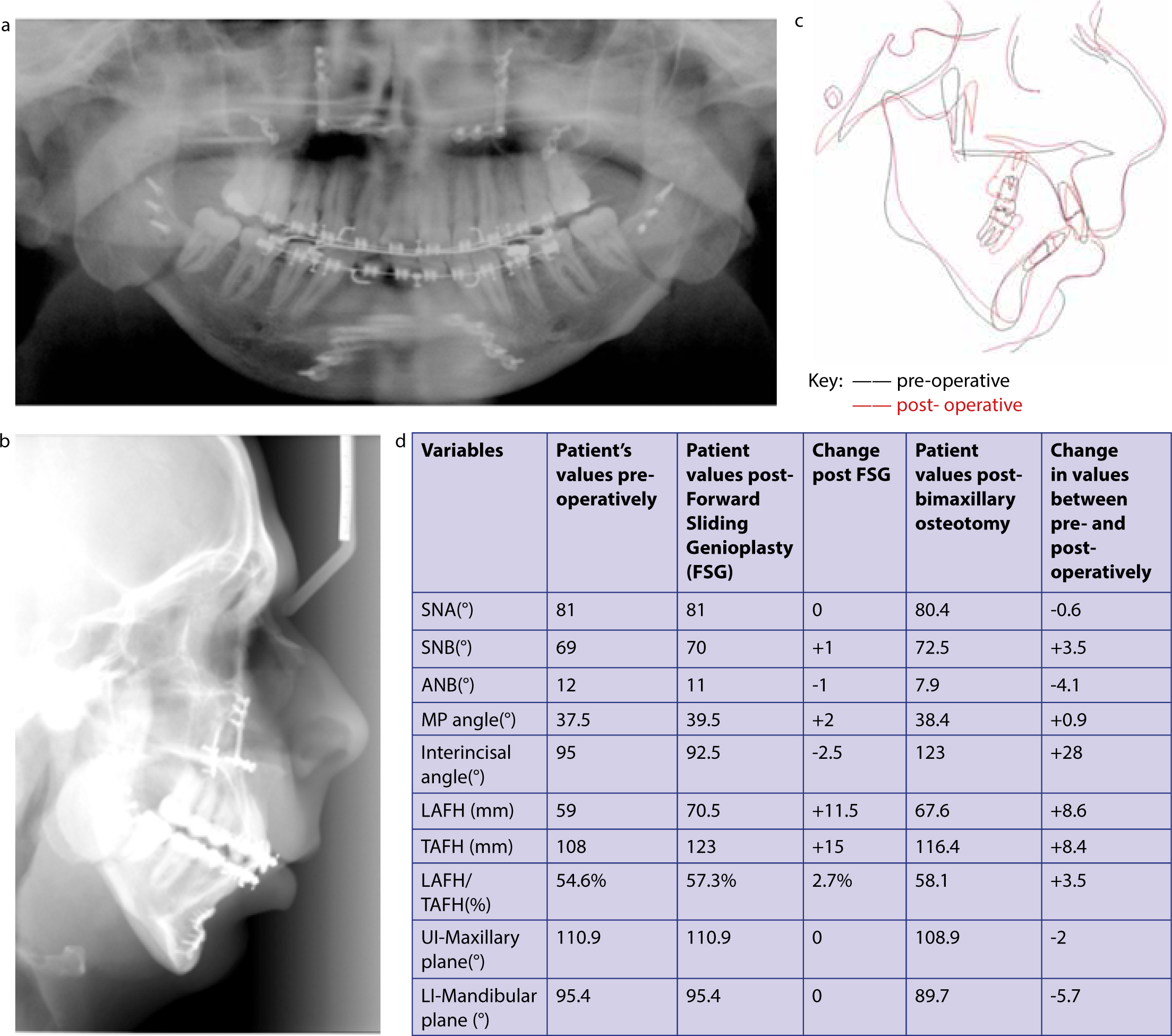
The more conventional approach of forward sliding genioplasty (Figure 3) followed by a thorough analysis of the CT scan (Figure 4) and bilateral sagittal split osteotomy and a posterior maxillary differential impaction, took precedence. The post-operative improvement is reflected intra-orally (Figure 5 a–e), whilst Figure 6 (a–d) represents the post-operative radiological investigations and illustrates the cephalometric superimposition and change in values. The justification for this approach was obtained from the computed tomography which showed enough ramal height above the lingula to perform this procedure and stability of resorptive effects of JIA. The post-operative radiographs (Figure 6a and b) show a significant improvement in the facial profile.
Figure 3.
(a–c) Post-operative clinical photographs following a forward sliding genioplasty (FSG) procedure. (d) Lateral cephalogram post – forward sliding genioplasty.Figure 4.
(a, b) Computerized tomography scan and three dimensional reconstruction to localize the lingula and plan a bimaxillary osteotomy procedure.Figure 5.
(a–e) Final post-operative intra-oral clinical photographs.Figure 6.
(a) Post-operative dental panoramic tomograph; (b) lateral cephalogram; (c) cephalometric superimposition and (d) changes in cephalometric values.
Although options (2) and (3) would have produced an instantaneous improvement in both function and aesthetics, treatment duration would have been longer and there are no long-term studies on TMJ arthroplasties and reconstructions.32
Conclusion
This case report highlights the characteristic features of a patient presenting with JIA associated with severely resorbed mandibular condyles. These patients form part of a very specific group and it is vital for medical practitioners and rheumatologists to identify the potential complications of this condition on the TMJ and oral function. Management is classically complex and requires highly specialized surgical skills in a multidisciplinary setting.
We describe the contemporary surgical management and tailored treatment which is totally dependent on discussions with patients, setting out the options, potential benefits and possible risks. Newer procedures, such as TMJ reconstruction, distraction osteogenesis and implants for orthodontic anchorage, should not be excluded, although further studies utilizing these techniques are needed to establish evidence-based practice.