References
Viganó CO, da Rocha VE, Junior LRM Rotation of the upper first molar in Class I, II, and III patients. Eur J Dent. 2016; 10:59-63 https://doi.org/10.4103/1305-7456.175696
Braun S, Kusnoto B, Evans CA The effect of maxillary first molar derotation on arch length. Am J Orthod Dentofacial Orthop. 1997; 112:538-544 https://doi.org/10.1016/s0889-5406(97)70081-7
Jung JM, Wi YJ, Koo HM Maxillary molar derotation and distalization by using a nickel-titanium wire fabricated on a setup model. Korean J Orthod. 2017; 47:268-274 https://doi.org/10.4041/kjod.2017.47.4.268
Wichelhaus A, Sander C, Sander FG Development and biomechanical investigation of a new compound palatal arch. J Orofac Orthop. 2004; 65:104-122 https://doi.org/10.1007/s00056-004-0214-5
Keles A, Impram S An effective and precise method for rapid molar derotation. World J Orthod. 2003; 4:229-236
Mheissen S, Khan H Derotation of an upper molar using cantilever mechanics. J Clin Orthod. 2022; 56:483-484
Gautam P, Valiathan A, Kumar S, Jain S The horseshoe molar derotator. J Clin Orthod. 2006; 40:538-541
Quadhelix for easy derotation of molars
From Volume 17, Issue 3, July 2024 | Pages 123-124
Article

Rotated first molars are a common problem, affecting upper molars in half of Class II and III orthodontic patients.1 Effective correction of molar rotations can lead to gain of arch space, which is important both in non-extraction cases,2, 3 and in extraction cases where anchorage is at a premium. Derotating molars provides a clinical conundrum, and there are many options available to clinicians to achieve this movement.
Previously described techniques to overcome this problem include compound palatal arches4 and transpalatal arches,5 which are reputedly for bilateral molar derotation. Other suggestions have included constructing complex archwires using cantilever mechanics6 or building a horseshoe molar derotator.7 Both of these techniques have proved to work; however, they may add to treatment times and cause unnecessary stress to the operator, as they require somewhat complicated wirebending techniques that may be unfamiliar to the treating clinicians.
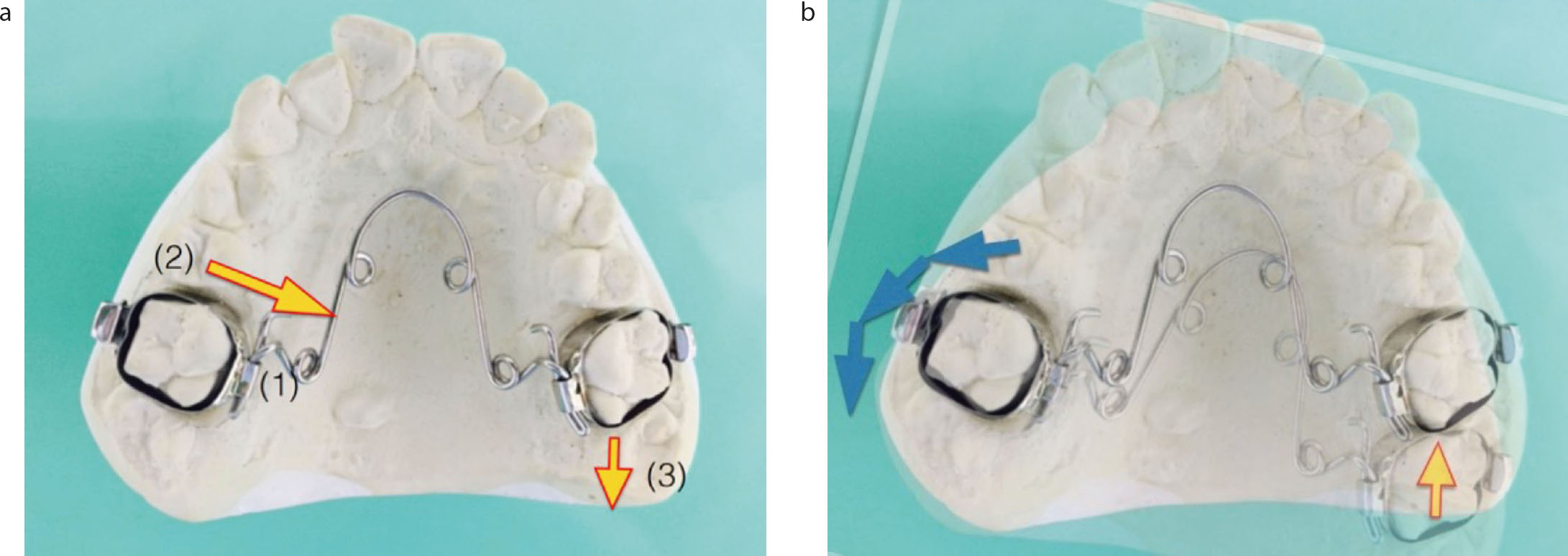
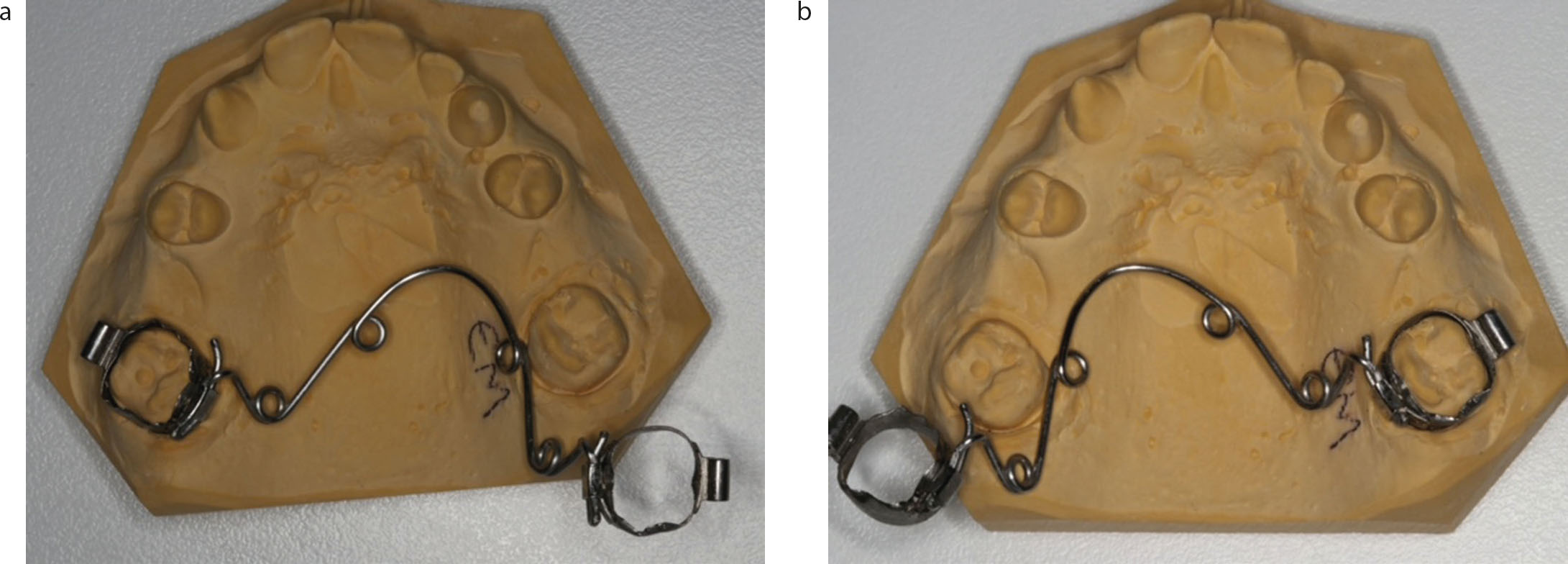
Derotation technique
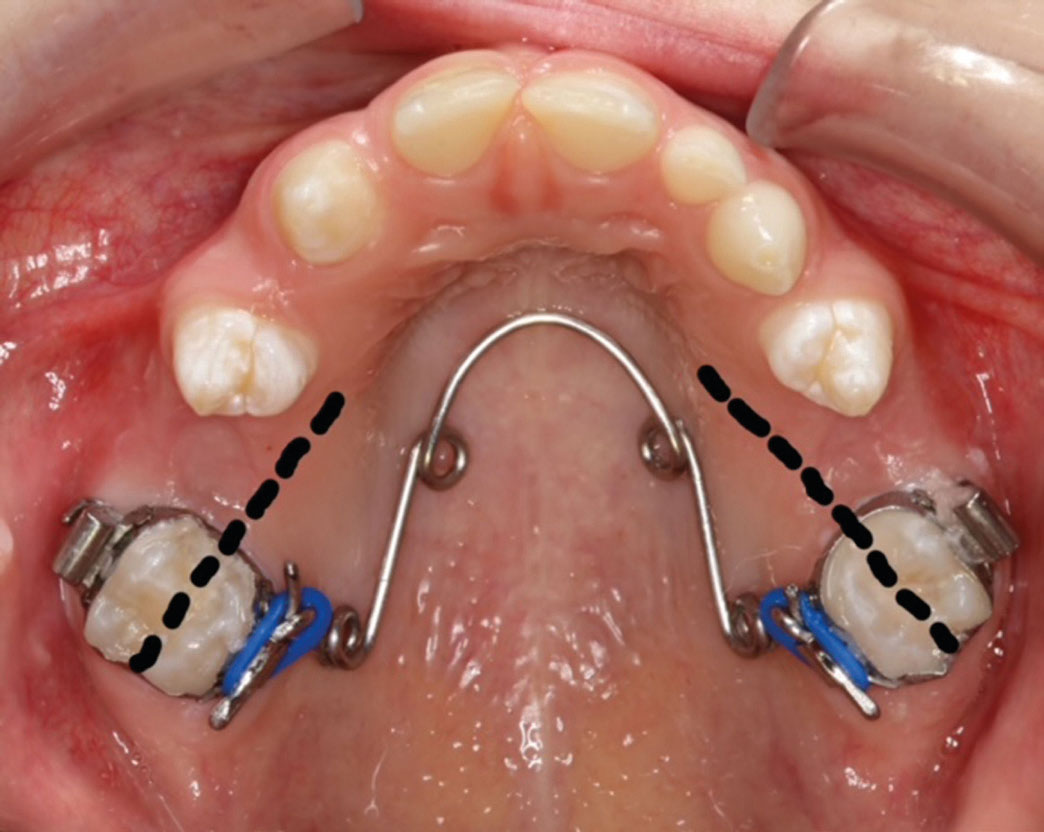
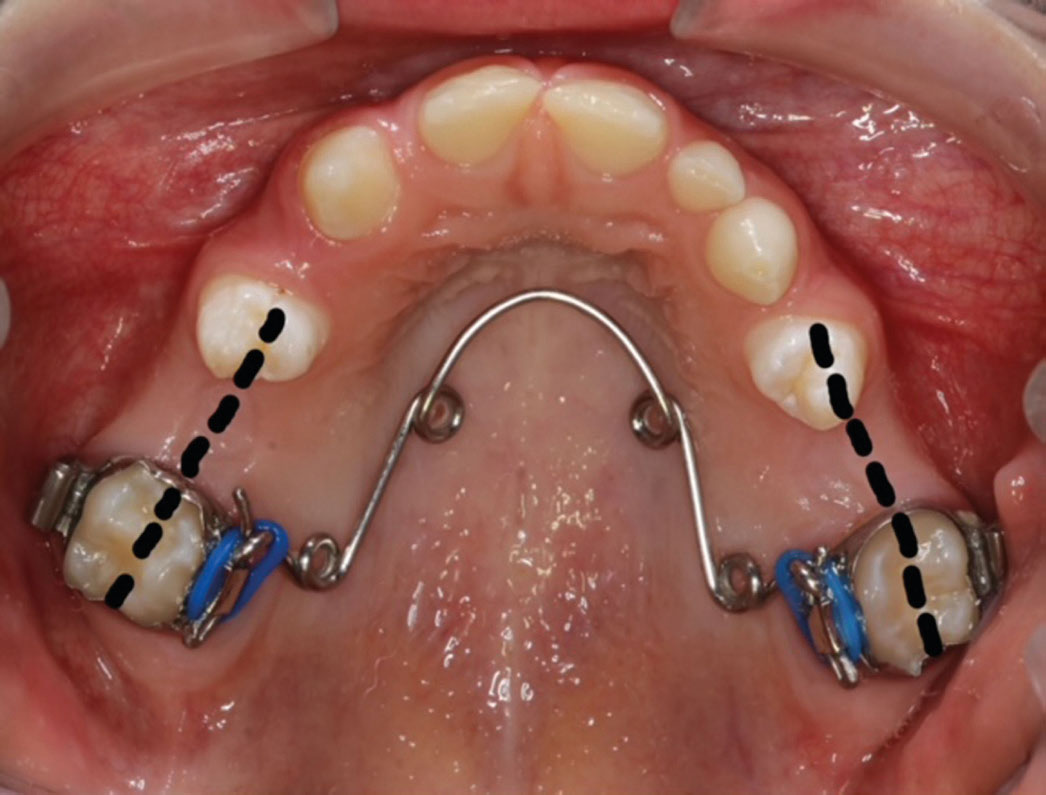
Adjustments to the mobile intra-oral arch removable quadhelix (Figure 1) demonstrate how to derotate an upper right first molar. A clinical case illustrates how these adjustments can be used to derotate both molars simultaneously (Figure 2). Figures 3 and 4 demonstrate what can be achieved with a correctly adjusted quadhelix, in just a few short months.