Article
All Orthodontists aim to provide time efficient treatment for their patients. This clinical tip shortens treatment time as well as providing an anchorage reinforcing solution to a relatively frequent Orthodontic problem.
Orthodontists managing patients with ectopic maxillary canines, using fixed appliances, traditionally wait until they are in rigid stainless steel archwires before applying traction to the canine.1 Some also advocate additional anchorage supplementation with TPAs or TADs, if the patient presents with high anchorage demands.2
It is well known that alignment of palatally impacted maxillary canines dramatically increases treatment times.3 Palatally ectopic canines not only occur in Class I occlusions, but are often seen in Class II division 1 and Class II division 2 malocclusions.4 In these patients, treatment times can be further increased if anterior-posterior (AP) correction is required, with a phase of functional appliance therapy prior to full upper arch fixed appliances, to align the ectopic canine.
Simple modifications can be made to the twin block design to allow for concurrent AP correction and alignment of the ectopic maxillary canine. Sectional fixed appliances can also be used in conjunction with functional appliances to align the upper labial segment and facilitate the AP correction, especially in Class II division 2 cases.
Figures 1 and 2 demonstrate a simple addition to a conventional modified twin block design. A distal facing hook is soldered to the bridge of the Adams crib on the upper first premolar, on the side of the impacted canine. In addition, a hook or cleat is bonded to the buccal surface of the canine, allowing traction to be applied with intra-oral elastics to start aligning the ectopic canine. This technique also allows unimpeded traction of the canine due to the bite opening effect of the twin block appliance (Figure 1).
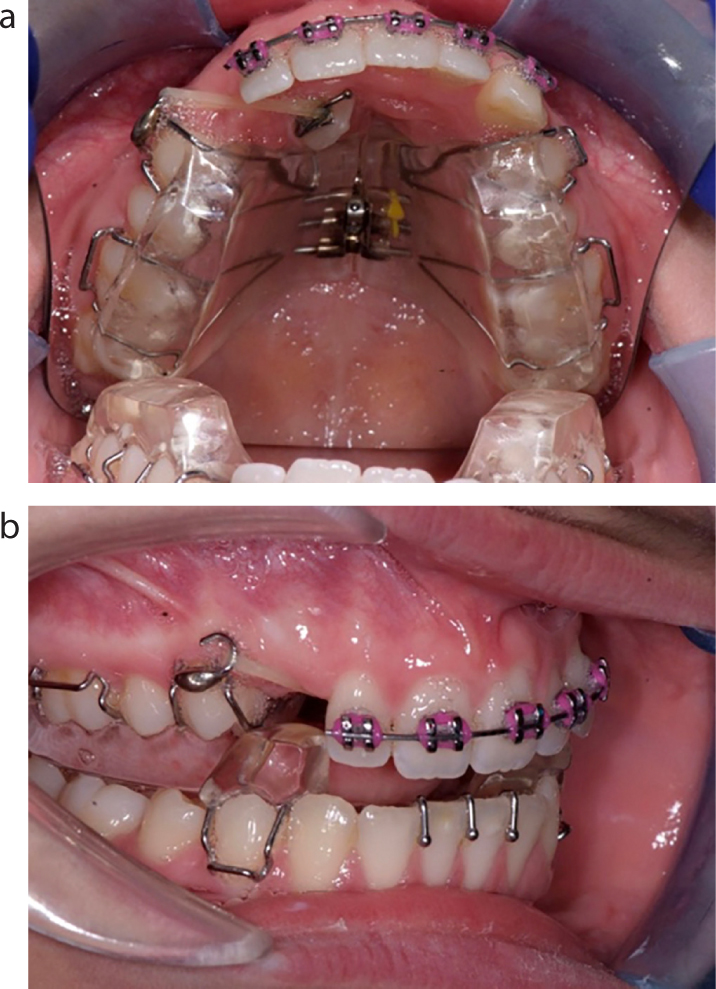

The patient can be instructed to change the elastics every day to ensure a low continuous force is being applied to the canine, thus overcoming the shortfall of other methods requiring the elastomeric chain or thread to be replaced by the Orthodontist, which is prone to rapid force decay.5 Furthermore, transverse and vertical anchorage demands are reduced in aligning the canines, as this is supplemented by the acrylic baseplate of the upper twin block and its adaptation to the palatal vault.
Once the canine approaches the line of the arch, further alignment is achieved with conventional ‘piggy back’ mechanics by simply replacing the hook on the canine with an eyelet, removing the Adams crib to the upper first premolar and bonding an orthodontic bracket to this tooth (Figure 2). Concurrent AP correction and canine alignment is achieved. Once the required AP correction has been achieved and the palatal canine is within the line of the arch, the case is finished using full upper and lower fixed appliances.
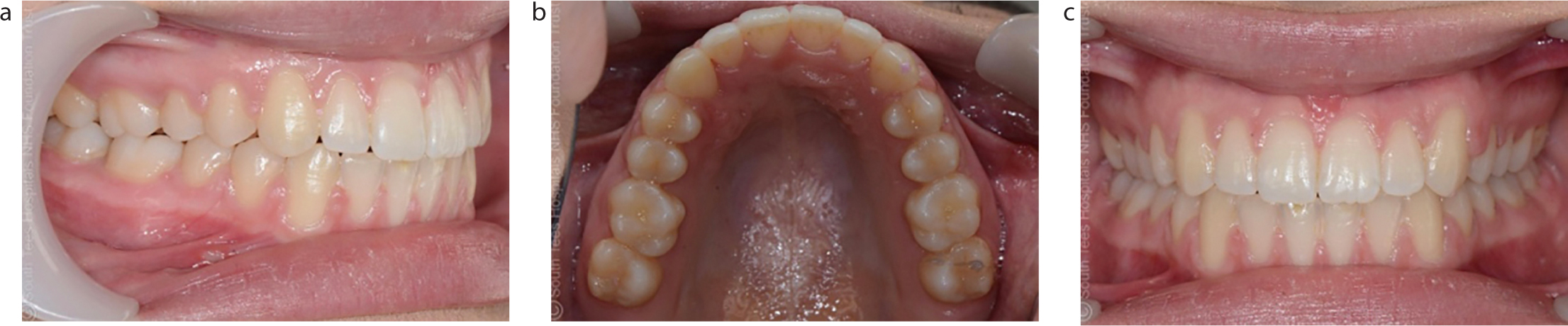
This clinical tip aims to maximize treatment efficiency, reducing the time the patient is wearing full fixed appliances and thus reducing the risks of iatrogenic damage associated with prolonged treatment times (Figure 3).