
Article
The difficulty, particularly with rotated lower incisors, is that there is very little span between the brackets to allow full engagement of the wire into the slot (Figure 1). Partial ligation means that the clinician has to tediously and continuously retie until the tooth derotates sufficiently to allow full ligation. Severely rotated lower incisors, especially when the patient is being treated on a non-extraction basis, can delay the progression from the initial aligning archwire. There are several techniques that have been employed including:


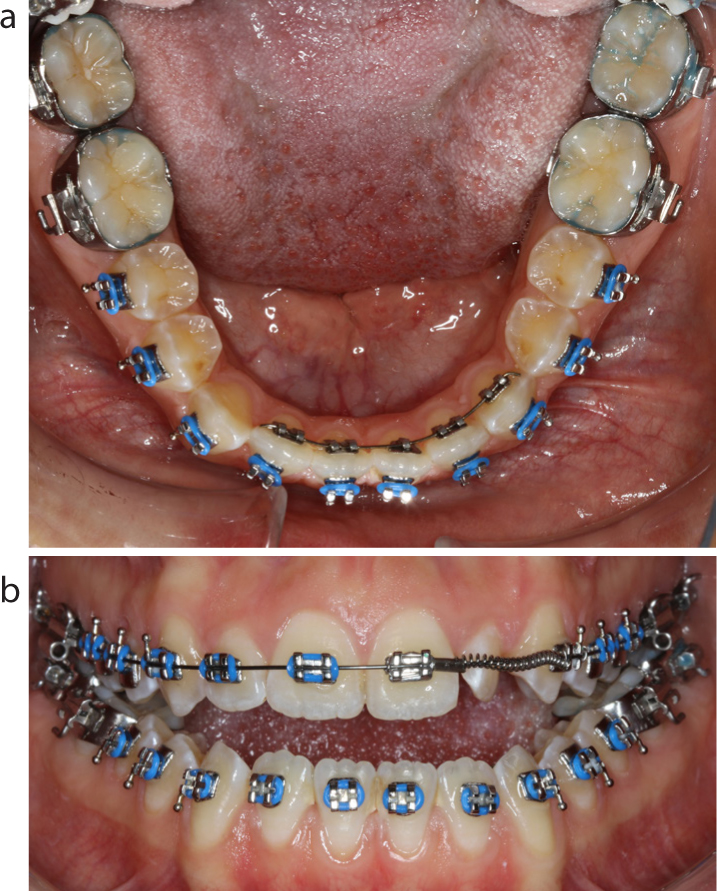
A useful technique to derotate lower incisors, where the mesial tie wings are too closely approximated to allow full archwire engagement, involves use of a 2D lingual appliance. These appliances are low profile. There is a simple gate that can be opened with a flat plastic to create the slot into which the archwire can be placed. There is no specific armamentarium required, apart from the brackets themselves. Molar tube holders can be used to place the brackets, and Weingart pliers to close the gates. A sectional archwire is placed (usually an 0.014” NiTi), which allows for sufficient derotation, to then place the labial archwire fully engaged in 6–8 weeks' time. The patients do not usually mind having a very short course of lingual appliance treatment, and the costs of the appliance are offset by the reduction in chairside time and time in the aligning archwire sequence.