Chate RA. Correction of a prominent premaxilla in a juvenile with a bilateral cleft lip and palate using a novel, hybrid function regulator, the FR-BCPPm, followed by preadjusted fixed appliances: a 20-year follow-up. J Orthod. 2022; 49:426-440 https://doi.org/10.1177/14653125221079635
Fränkel R. The theoretical concept underlying the treatment with function correctors. Rep Congr Eur Orthod Soc. 1966; 42:233-254
McNamara JA JCO interviews Dr James A McNamara, Jr on the Frankel appliance. Part 1 – Biological basis and appliance design. J Clin Orthod. 1982; 16:320-337
McNamara JA JCO/interviews Dr James A McNamara, Jr on the Frankel appliance. Part 2 – Clinical management. J Clin Orthod. 1982; 16:390-407
Goshgarian RA. Orthodontic palatal arch wires.: United States Government Patent Office; 1972
Baldini G, Luder HU. Influence of arch shape on the transverse effects of transpalatal arches of the Goshgarian type during application of buccal root torque. Am J Orthod. 1982; 81:202-208 https://doi.org/10.1016/0002-9416(82)90053-7
Kharche A, Durkar S, Kawale P Transpalatal arch: an overview of literature. J Adv Med Dent Scie Res. 2019; 7:26-32
McNamara JA, Bookstein FL, Shaughnessy TG. Skeletal and dental changes following functional regulator therapy on class II patients. Am J Orthod. 1985; 88:91-110 https://doi.org/10.1016/0002-9416(85)90233-7
Kerr WJ, TenHave TR, McNamara JA A comparison of skeletal and dental changes produced by function regulators (FR-2 and FR-3). Eur J Orthod. 1989; 11:235-242 https://doi.org/10.1093/oxfordjournals.ejo.a035991
Björk A, Skieller V. Growth of the maxilla in three dimensions as revealed radiographically by the implant method. Br J Orthod. 1977; 4:53-64 https://doi.org/10.1179/bjo.4.2.53
The design features of a novel, hybrid function regulator, the FR BCPPm, are presented to facilitate the construction of other such appliances that may be used in the treatment of juveniles with a prominent premaxilla associated with a bilateral cleft lip and palate and mandibular retrusion. As an essential prerequisite to facilitate secondary alveolar bone grafting, how it may be used and the results that can be achieved are documented in a single case.
CPD/Clinical Relevance: To illustrate the design features of a novel function regulator in detail, which may be used to correct a prominent premaxilla in a patient with bilateral cleft lip and palate.
Article
The correction of a bilateral cleft's prominent pre-maxilla is a challenging clinical problem, but a recent case report has illustrated a successful outcome after a decade of treatment with a novel, hybrid functional appliance, namely the Function Regulator, for use in juveniles with mandibular retrusion, a bilateral cleft and a prominent premaxilla (the FR BCPPm), together with a nocturnal high-pull headgear, a quad helix (QH) appliance, followed by a stabilizing transpalatal arch (TPA) and a subsequent period of post-functional, pre-adjusted fixed appliances.1
Over half a century ago, Fränkel first described the design, construction and clinical management of his various function regulators for the correction of Class I, Class II division 1 and Class III malocclusions,2,3,45 which others have since either expanded on, or modified.6,7,8,9,10,11,12,13,14
The aims of this article are therefore to describe in detail the design features of one further, new variant of function regulator, namely the FR BCPPm, so that it may be replicated for use in other patients with bilateral cleft lip and palate and a prominent premaxilla, and through a single case, to document its effects on the growth and development of the teeth, face and the premaxilla.
Case report
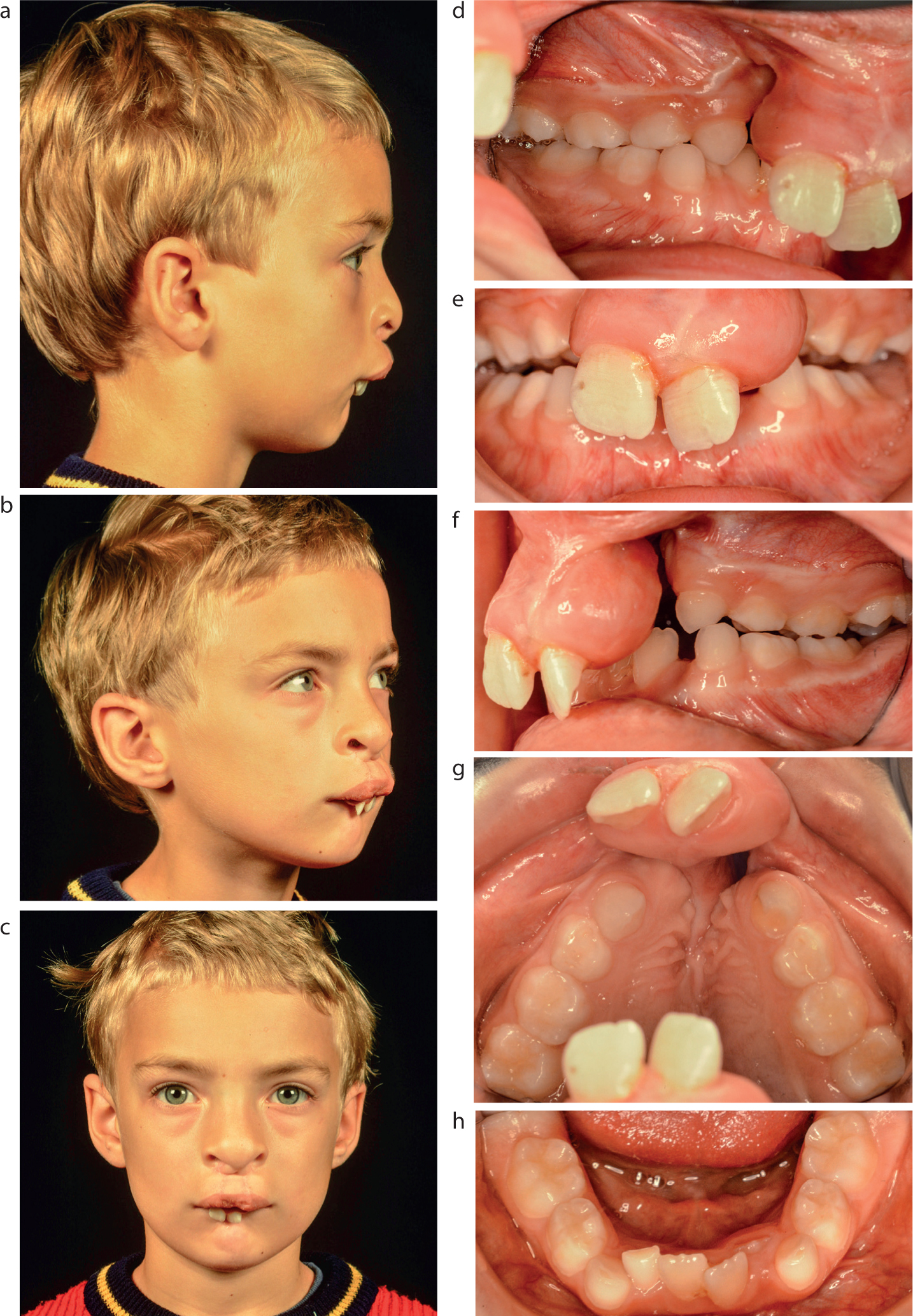
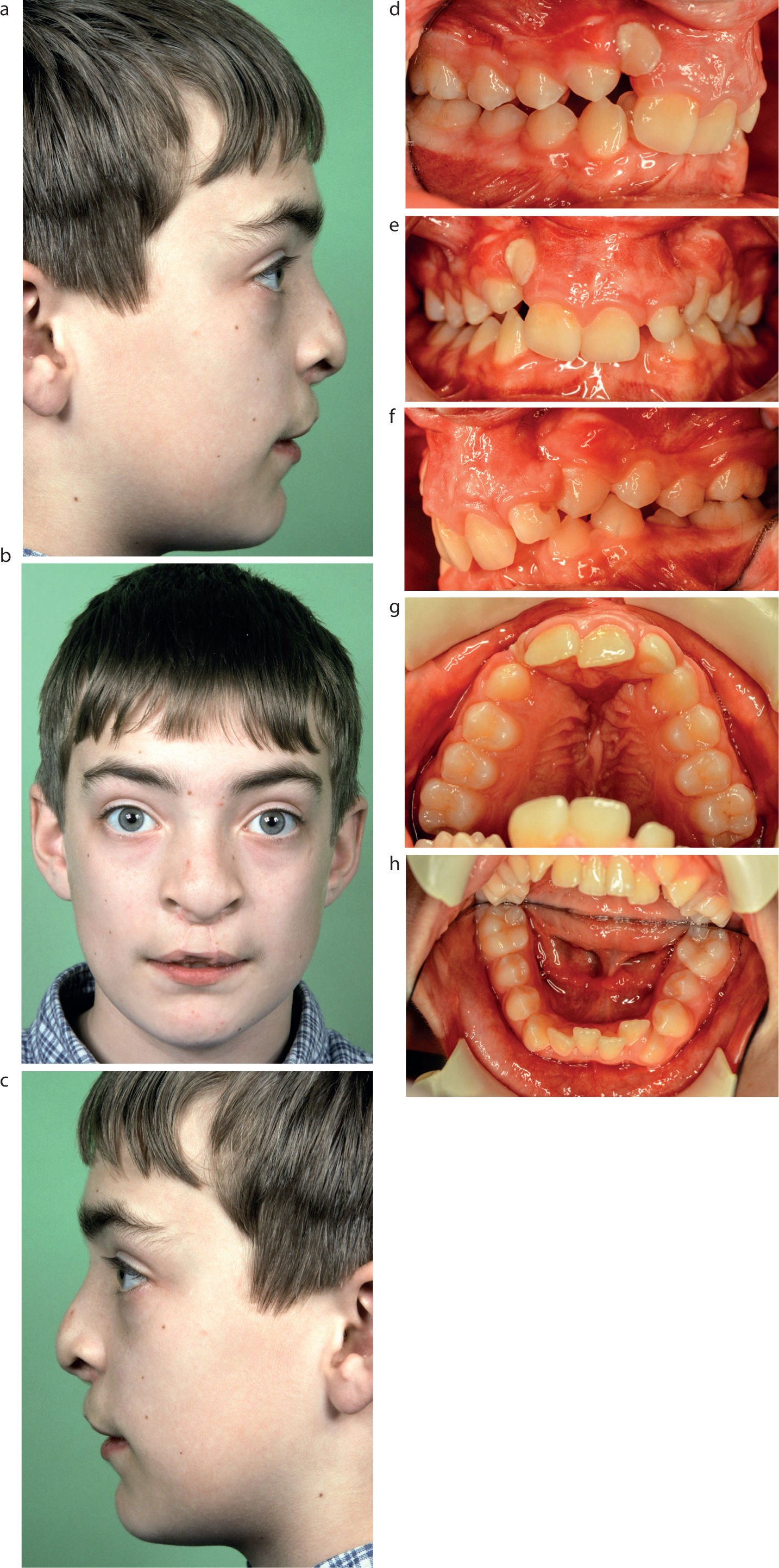
BS was born with a bilateral cleft lip and palate, which was repaired surgically with lip closure at 5 months and hard and soft palate closure at 8 months. By the age of 7 years, the presence of severe mandibular retrognathia, a prominent premaxilla with incompetent lips, palatal lower lip trapping and a pronounced Class II division 1 malocclusion in the early mixed dentition stage was evident (Figure 1).
Figure 1.
(a–h) Extra-oral and intra-oral views the patient at age 7. (Figure 1 d–h reproduced by kind permission of SAGE Publications Inc.)1
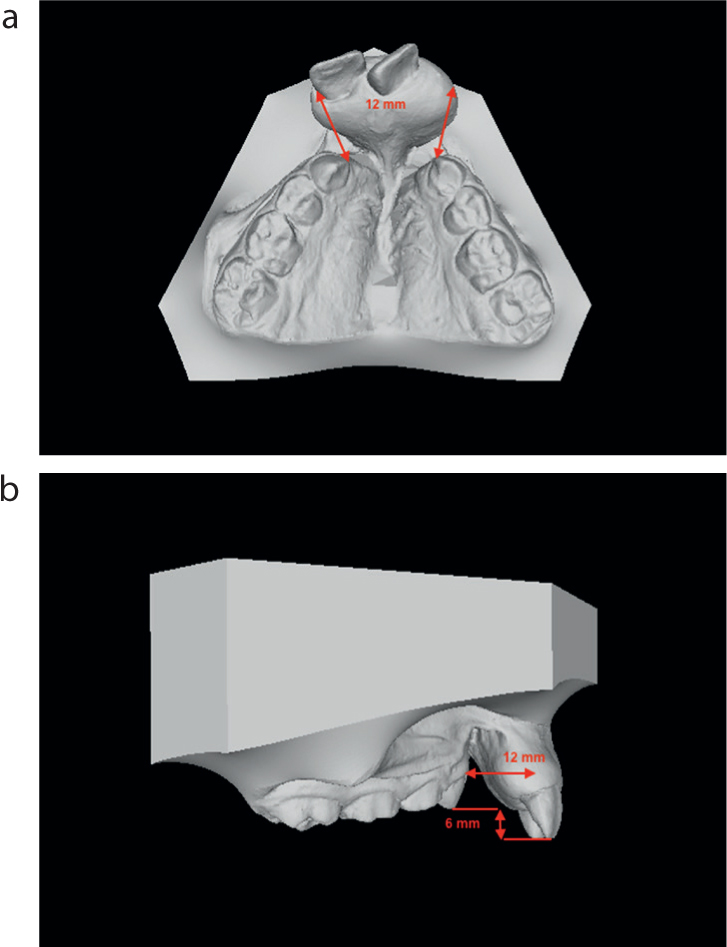
The surgeons on the multidisciplinary cleft team were also concerned about the very large separations and displacements between the gingival and alveolar tissues on either side of both clefts, in relation to how these would prevent achieving full soft-tissue coverage after the insertion of alveolar bone grafts (ABGs), which would otherwise compromise their post-operative integration and consolidation. As such, with only 2 years left before the patient would reach the youngest age at which an ABG could be inserted, there was a sense of urgency to correct the 18.5-mm overjet, the 12-mm increased overbite, the 12-mm wide alveolar gaps, the bilateral crossbites and the 6-mm vertical steps between the posterior and anterior aspects of the maxillary occlusal plane (Figure 2).
Figure 2.
(a) The 12-mm wide alveolar gaps. (b) The maxillary occlusal plane's 6-mm vertical steps.
Consideration was therefore given as to which appliance could be used during the deciduous and early mixed dentition stages and a function regulator of Fränkel was selected. This was because, unlike tooth-borne activators, the acrylic parts of a function regulator remain on the outside of the dental arch, and its component parts become active, not by being in contact with the teeth and alveolar processes, but by standing away from them.4 It is therefore irrelevant if not all of the permanent teeth are present for appliance retention or for tooth movements to be effected, because the modus operandi of a function regulator is to stretch and hold away the soft tissues from the teeth, in order to allow myofunctional forces to exert their effects on them, instead.3,5
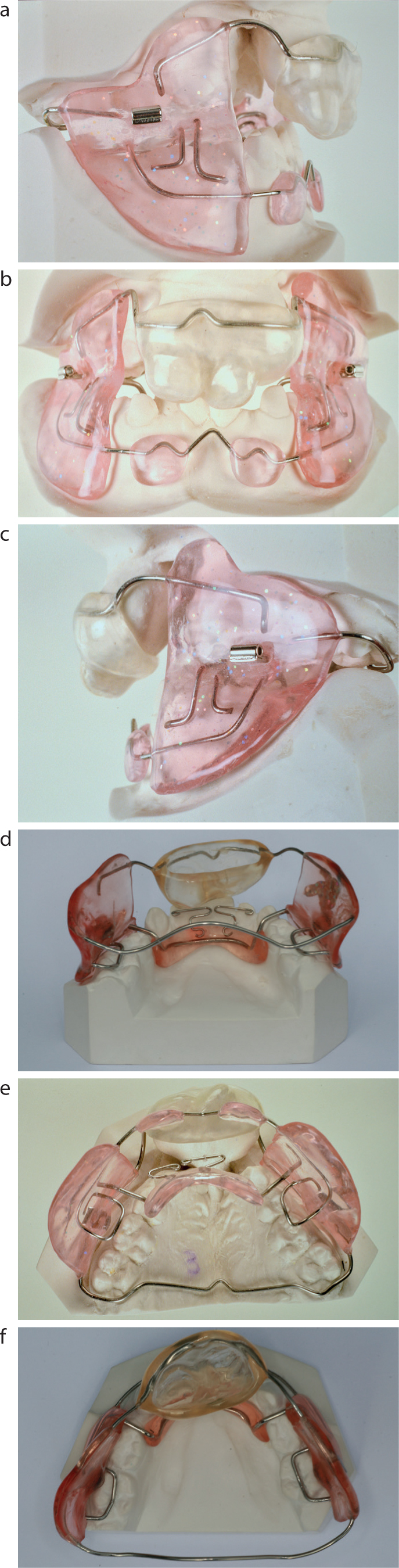
To this end, a new functional appliance was created, the FR BCPPm, which was a hybridized amalgamation of Fränkel's FR I and FR III function regulators, together with two novel additions; namely a clear acrylic bulb embedded in an upper labial bow that encapsulated the premaxillary incisors and extra-oral traction (EOT) tubes that were incorporated in the buccal shields of the appliance (Figure 3).
The FR BCPPm was designed to realize the clinical objectives of (i) approximating the opposing cleft alveolar margins towards each other; (ii) levelling up the anterior to the posterior aspects of the maxillary occlusal plane; (iii) correcting the bilateral crossbites through the expansion of the lesser segments of the cleft maxilla; (iv) establishing a normal incisor occlusion; and (v) creating an anterior oral seal.
The first three of these clinical objectives were to facilitate achieving complete, tension-free, mucoperiosteal flap coverage of the future ABGs and so minimize the prospects of either inadequate peri-operative soft-tissue cover and/or post-operative wound breakdowns, either of which could jeopardize the success of the bone grafts.
The design features of the FR BCPPm
The aspects of the FR BCPPm that are drawn from the FR I appliance include the upper labial bow; the lower incisor cingulum wires; the lower labial sulcus acrylic pads and the lower anterior lingual shield of acrylic (both of which are jointly constructed to effect forward mandibular protrusion); the cross-over hanger wires that pass from the lingual shield and connect it to the acrylic vestibular shields; and the vestibular flanges that are extended in order to project into the alveolar sulci with generous lateral relief of the upper buccal segments (Figure 3a–e).
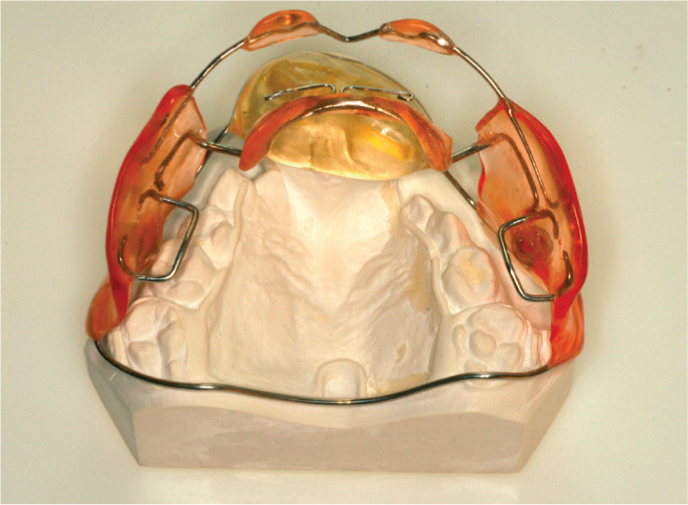
Figure 3. Views of the FR BCPPm: (a) Right lateral; (b) frontal; (c) left lateral; (d) lower antero-lingual; (e) upper occlusal; and (f) lower occlusal.
Those that are derived from the FR III appliance are the transpalatal arch, which passes distal to the upper terminal molars from one vestibular shield into the other on the opposite side, as well as the lower molar occlusal stops (Figure 3e,f).
The two novel components of the clear acrylic cup that encapsulates the premaxilla and its incisor teeth, together with the buccal shields' EOT tubes are illustrated in Figure 3a–c.
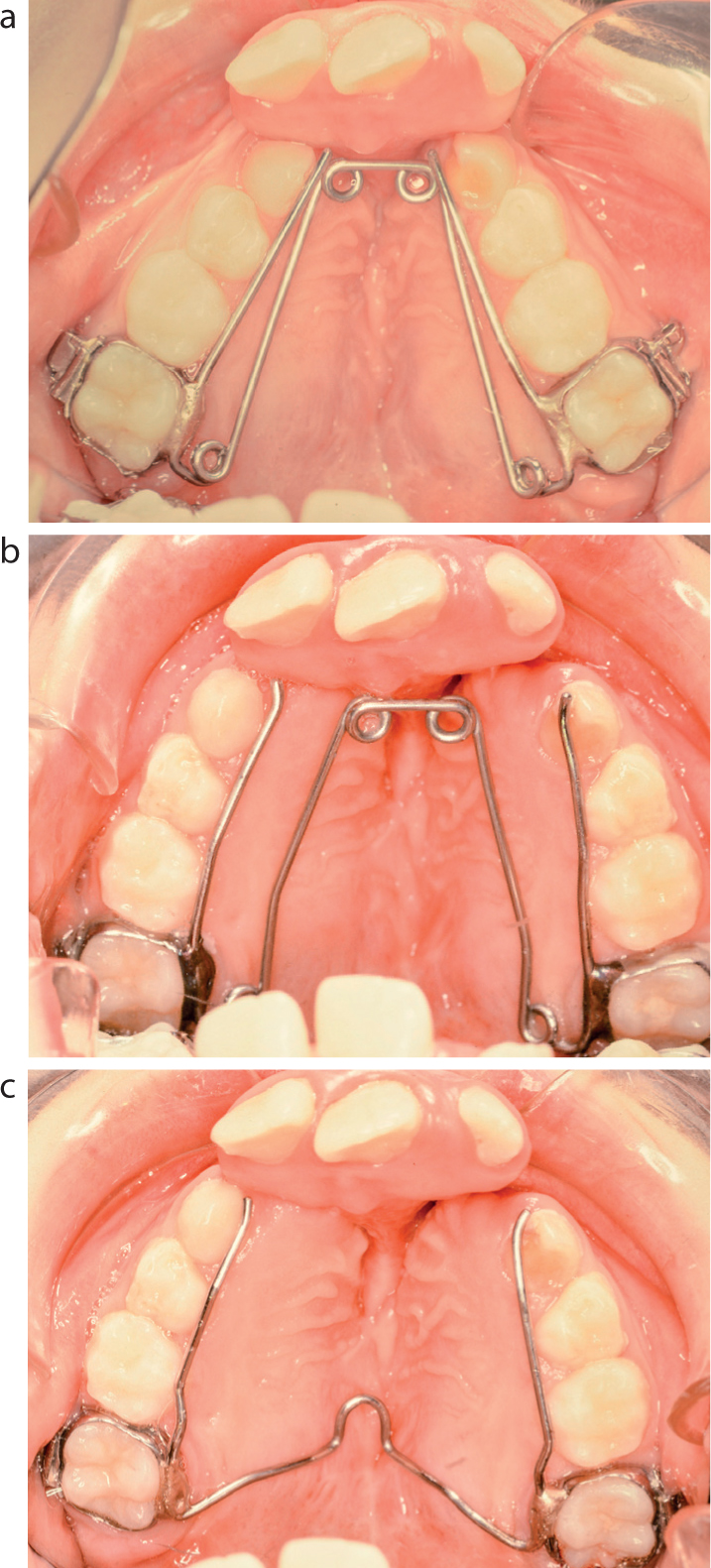
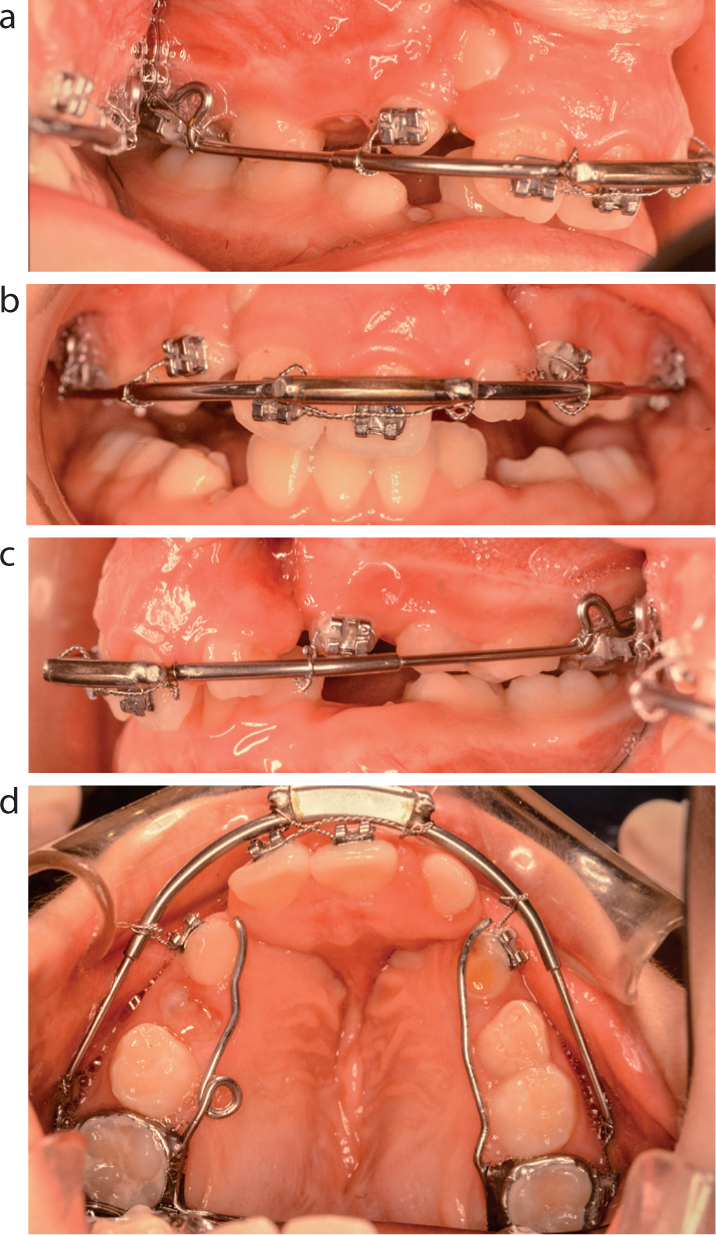
As part of the treatment with the FR BCPPm, a QH appliance is used concomitantly to expand the upper arch,15,16 followed by a stabilizing, soldered Goshgarian-type TPA17,18,19 that remains in situ until the insertion and consolidation of the alveolar bone grafts (Figure 4).
Figure 4. Maxillary occlusal views of the quad helix (a) pre-expansion and (b) post-expansion. (c) Stabilizing Goshgarian TPA.
Table I lists both the wire dimensions, and the origins of the appliances' various wire components that are used, although these can be seen to vary slightly, depending on which source is referenced.7,9,10,12,14,16,17,18,19
Wire components
Dimensions (mm)
Origins
Upper labial bow
0.9
FR I
Lower labial pad wires
0.9
FR I
Lower incisor cingulum wires
0.7
FR I
Lower lingual hangar wires
1.25
FR I
Vestibular shields' transpalatal wire
1.0
FR III
Lower molar occlusal stops
1.0
FR III
Quad helix
0.9
Bio-progressive therapy
Transpalatal arch
0.9
Goshgarian TPA
FR: function regulator of Fränkel; QH: quad helix; TPA: transpalatal arch.
Modus operandi of the FR BCPPm in realizing the clinical objectives
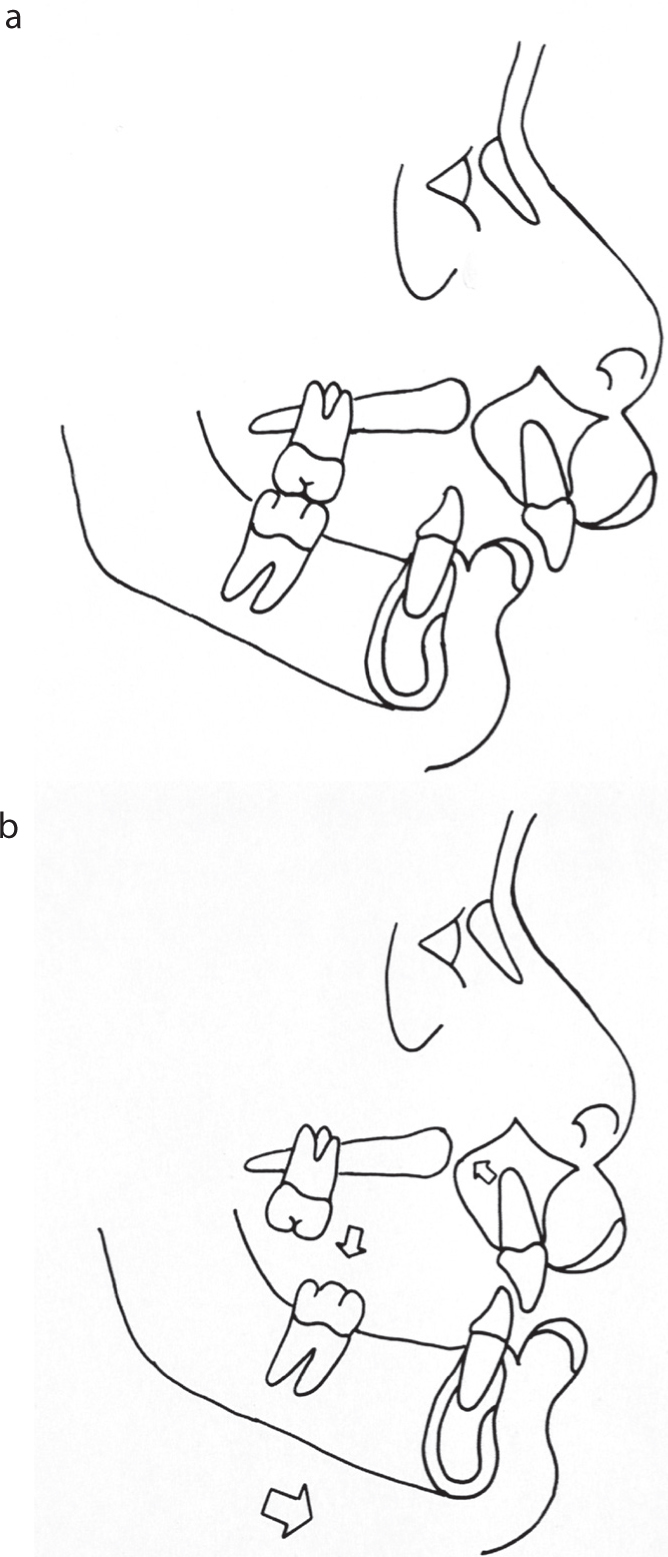
The approximation of the opposing cleft alveolar margins and the levelling of the maxillary occlusal plane are achieved through both the vertical intrusion and horizontal restraint of the premaxillary incisors, together with the unopposed eruption of the maxillary posterior teeth (Figure 5).
Figure 5. Schematic profile line diagrams of (a) the prominent premaxilla and (b) the required mandibular protrusion, premaxillary vertical intrusion + horizontal restraint and the preferential eruption of the upper posterior teeth.
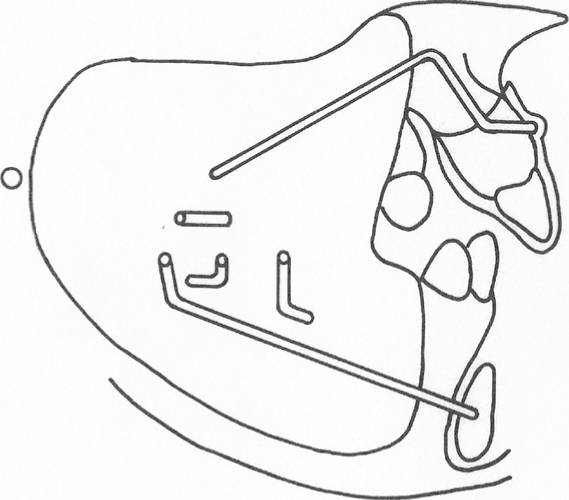
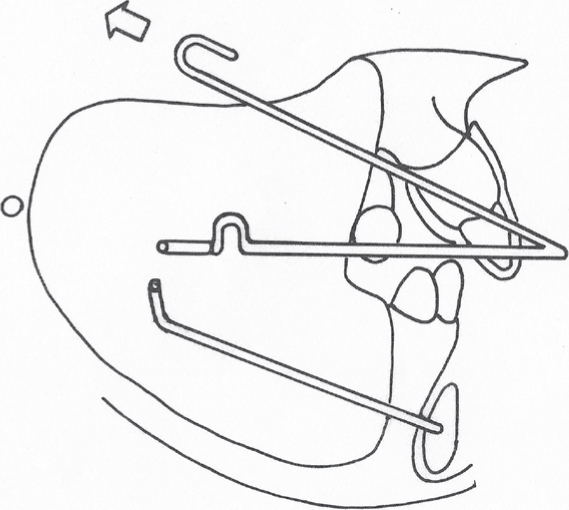
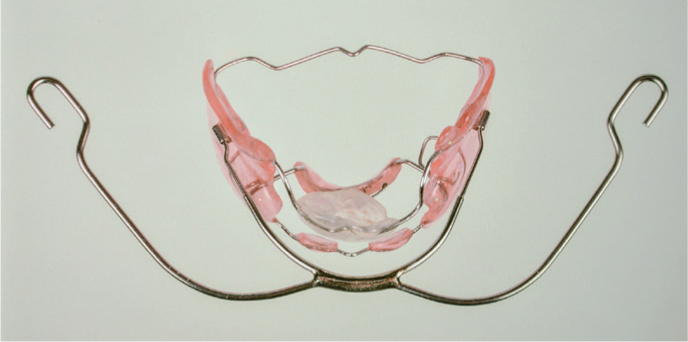
The premaxilla acrylic cup is designed to restrain the downward and forward development of the premaxillary incisors (Figure 6), while the buccal shield EOT tubes facilitate the insertion of a Kloehn facebow and the use of an occipital, high-pull headgear at night that supplements the acrylic cup's intrusive action (Figures 7 and 8).
Figure 6. Schematic profile line diagram of the FR BCPPm.Figure 7. Schematic profile line diagram of the FR BCPPm with a facebow attached.Figure 8. An FR BCPPm with a Kloehn facebow attached to the vestibular shields' EOT tubes.
Posteriorly, the unopposed eruption of the maxillary molars is promoted by the positioning of the interconnecting vestibular shields' transpalatal arch, which, rather than passing over the mesial marginal ridges of the upper terminal molars, instead passes distal to them (Figure 3e). In conjunction, the lower molar stops facilitate the unopposed eruption of the upper posterior teeth by obstructing the vertical eruption of the mandibular terminal molars (Figure 3d,f).
In the correction of Class II division 1 malocclusions with a function regulator, in order to avoid creating bilateral crossbites as the mandibular dentition develops forwards, generous lateral relief of the maxillary buccal dentition is incorporated in the design of an FR I, usually around 3 mm on each side,9 with the upper peripheries of the acrylic vestibular shields also extended to purportedly stretch and thereby stimulate the adjacent peri-oral musculature. In this way, unopposed tongue pressure expands the maxillary dental arch,2,3,4,5 and, as a consequence of the peri-oral musculature tension, it is claimed that osteogenic activity in the area of muscle insertion is elicited,3,4,6 which purportedly facilitates the expansion that is required to avoid the development of a buccal crossbite, and to relieve any crowding as treatment to advance the mandibular dentition progresses.2,3,4,5
However, in situations with a surgically repaired cleft palate, this feature of the function regulator that would normally produce upper arch expansion is ineffective. This is because of the inelastic mid-palatal scar tissue and, as a consequence, concomitant active dental expansion must be undertaken using a QH appliance while the FR BCPPm is being worn instead, which is then subsequently stabilized by a Goshgarian TPA (Figure 4). With the design of the FR BCPPm, the traditional FR I function regulator vestibular shields' lateral relief for the upper buccal segments provides clearance into which the upper canines and posterior teeth can be expanded (Figure 3e), while the FR III's transpalatal arch, which passes distal to the upper terminal molars, also avoids physical contact and/or interference with either the QH or the TPA, which are cemented by bands onto the maxillary first permanent molars (Figure 9).
Figure 9. Occlusal view of the FR BCPPm on the work model, showing the lateral relief for the upper buccal segments and the transpalatal arch that passes distal to the terminal molars, on which is cemented a TPA.
In order to establish a normal incisor occlusion, a clinical construction bite must be taken with approximately 4.0–6.0 mm of mandibular advancement, which will usually result in an incisor edge-to-edge occlusion.9 For more severe Class II cases, the mandible needs to be re-advanced approximately 6 months later, either by constructing a new function regulator,9 or by advancing the lower labial and lingual acrylic pads downwards and forwards as a unit,13 across the split vestibular shields that may be pre-emptively incorporated in the appliance's initial design and construction.4,5
It is the co-related anterior positioning of the lower labial lip pads and the lingual shield in a function regulator that encourages the adoption of a protruded mandibular position, and it is this that effects the Class II incisor correction. Fränkel emphasized that the difference between his function regulator and tooth-borne activator functional appliances was that rather than producing a Class II traction effect on the upper and lower dentitions,4 whenever the mandible tries to fall back into its habitual distal position, the lingual acrylic shield produces a reaction by making contact with the mucosa at the lingual surfaces of the alveolar process,3 and thereby through feed-back, the lateral pterygoid muscles are activated to protract the mandible and so purportedly stimulate compensatory growth of the condylar cartilage, instead.4,5
In reality though, while the lower incisor cingulum wires are designed to prevent only lower incisor extrusion during treatment as a means of reducing a deep overbite,9 they do result in lower incisor proclination,20,21 which is why an appliance modification has been previously described to try to limit this.8
For similar reasons, the FR II was created with an additional wire palatal to the upper incisors,9 in order to counter the FR 1 upper labial bow's tendency to retrocline the upper incisors during treatment.20,21
However, in those Class II cases with proclined maxillary incisors, retroclination by the upper labial bow is desirable, but in the case of the FR BCPPm, its primary role is to provide a means of connecting the premaxillary acrylic cup to the body of the appliance.
In order to establish an anterior oral seal, the lower labial sulcus acrylic pads act to: (i) inhibit the aberrant vertical contraction of the mentalis muscles;9 (ii) prevent the lower lip from curling outwards, erecting it to contact the upper lip, instead;5 and (iii) flatten the pronounced labio-mental sulcus.9
However, it is suggested that to effectively establish an anterior oral seal, the use of lip-seal training exercises in conjunction with the lower labial pads is also essential.4,5,9
However, if these acrylic pads are not constructed to fit into the depth of the lower labial sulcus,9,20 or if they are subsequently advanced just horizontally forwards from the depth of the lower labial sulcus, rather than being advanced both downwards and forwards when further protrusive activation is required,13 this can result in lower incisor proclination. This is because the pads then push against orbicularis oris, which creates a lower lip bumper effect that leaves the tongue pressure against the lower incisors unopposed, thereby resulting in their unwanted proclination. In addition, the desired restrictive effect of the lower labial acrylic pads on the aberrant mentalis muscle activity is also lost,20 which consequently compromises the ultimate establishment of competent lips.9
Clinical deployment and standard regimen of wear of the FR BCPPm
At the age of 7 years, BS was supplied with, and instructed to wear, his FR BCPPm for only 2 hours per day for the first fortnight, thereafter progressing to additional night-time wear for a month, followed by a gradual advance to full-time wear at his own pace (excluding sports and eating), as previously recommended (Figure 10).3,6
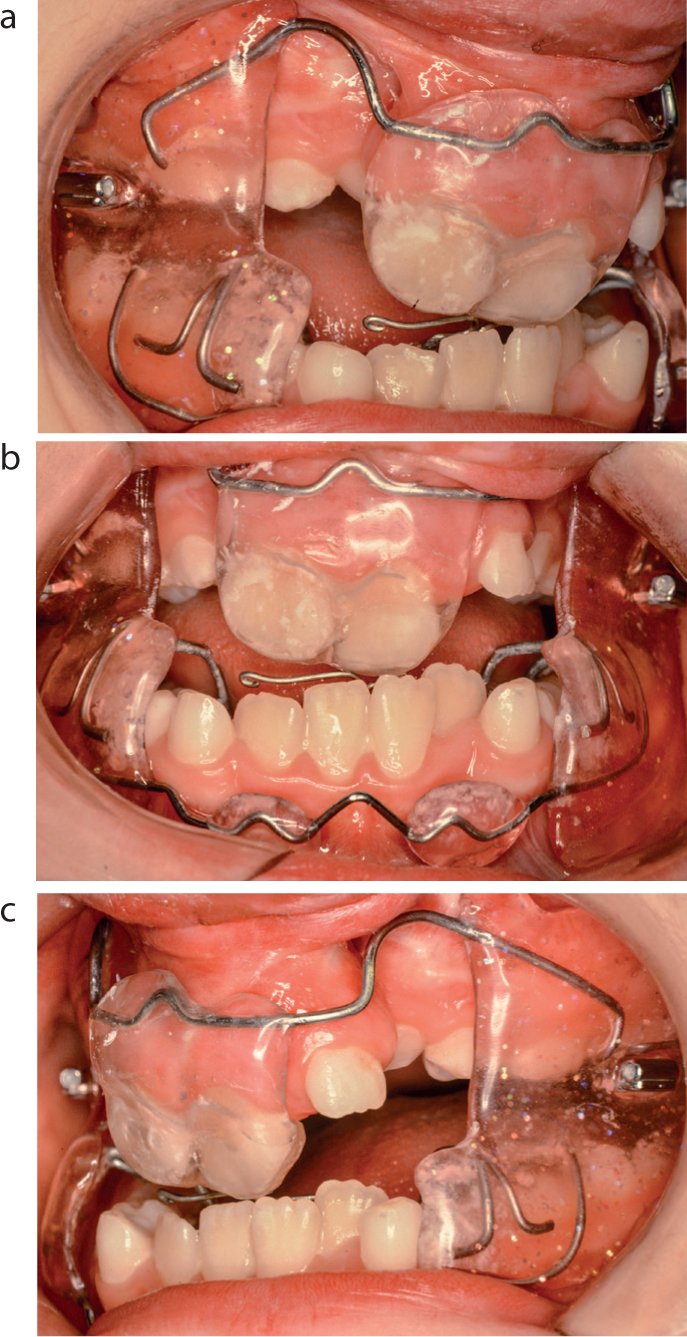
Figure 10.
(a–c) Intra-oral views of the FR BCPPm being worn. (Reproduced by kind permission of SAGE Publications Inc.)1
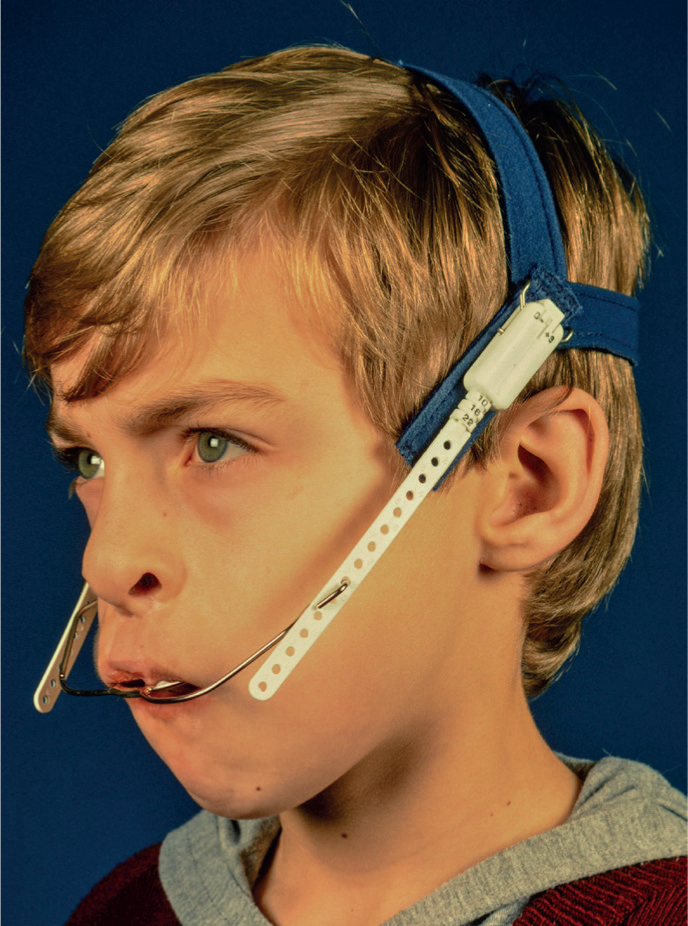
After 7 months, he reached full-time wear of the FR BCPPm and 6 months later, at the age of 8.5 years, the nocturnal wear of an occipital-pull headgear was initiated (Figure 11).
Figure 11. An occipital, high-pull headgear worn with the FR BCPPm.
Note should be made in the illustration that only a single headgear safety product was used, namely a snap-away safety clip, because at the time of its application in the early 1990s, the selection of just one of any such safety products per headgear prescription was standard practice.22 It was not until well after the cessation of this patient's treatment that the use of two separate, independent headgear safety products became the established norm.23
In relation to the number of scheduled appointments that are required to monitor progress with the FR BCPPm, although function regulators have no wire components that need to be reactivated, the lower lingual acrylic shields and the vestibular-extended buccal shields require frequent and regular reviews. This is because as the mandible tries to fall back into its habitual distal position, the lower lingual shield stimulates a protrusive reaction by making contact with the mucosa at the lingual surfaces of the alveolar process.3 If the shield's acrylic does not remain well below the gingival margins of the lower anterior teeth throughout, there is a risk of irritation and stripping of the lingual gingiva.9
For the same reasons, the differentiation between areas of mucosal erythema associated with the pressure exerted by the vertically extended vestibular shields and overt traumatic ulcerations also requires close attention.6
The patient wore his FR BCPPm full time, and after 2 years, he was supplied with a QH to correct his crossbites. Figure 12 shows the over-expansion that was achieved 6 months later. Unfortunately, 7 months after his first TPA was inserted, one of the soldered joints failed and the crossbites relapsed. It took a further 8 months for another QH to recover the situation, after which a new TPA was fitted and wear of the FR BCPPm was temporarily suspended while a stabilizing maxillary arch bar to immobilize the maxillary cleft segments was applied,24 just prior to his admission for the insertion of the ABGs (Figure 13).
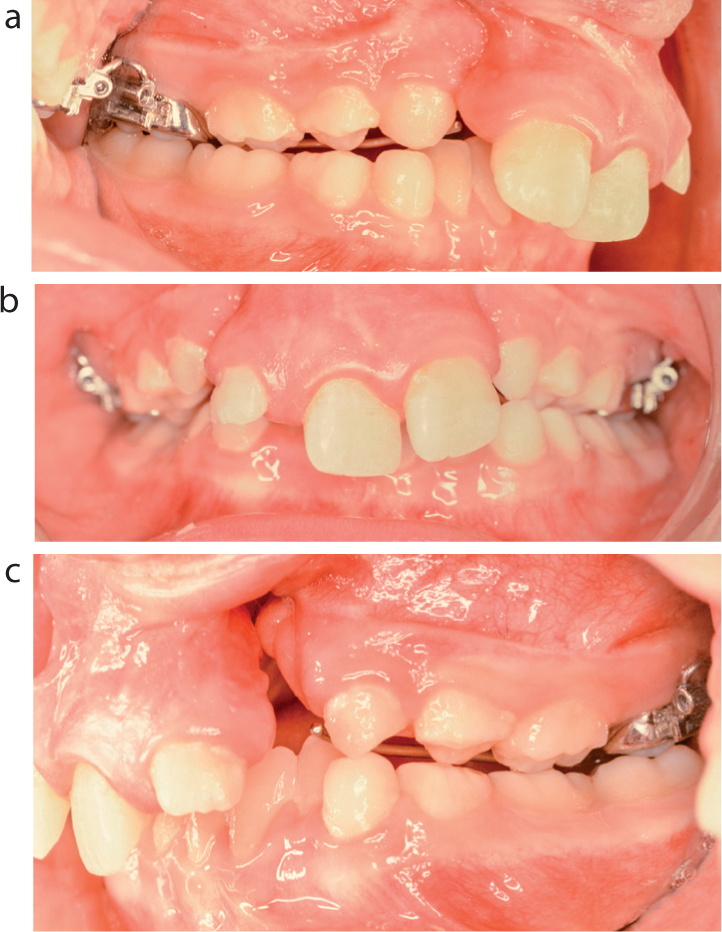
Figure 12.
(a–c) Intra-oral views of the over-expanded upper buccal segments.Figure 13.
(a–d) Intra-oral views of the stabilizing maxillary arch bar that was modified from a Kloehn facebow.
After the consolidation of his grafts and the removal of his arch bar and TPA, a new FR BCPPm was supplied. It was worn only at night from the age of 11 until all of his permanent teeth had erupted at age 13, after which he commenced a second stage of treatment with non-extraction fixed appliances.1
The effect of the FR BCPPm on the growth of the dentition and jaws
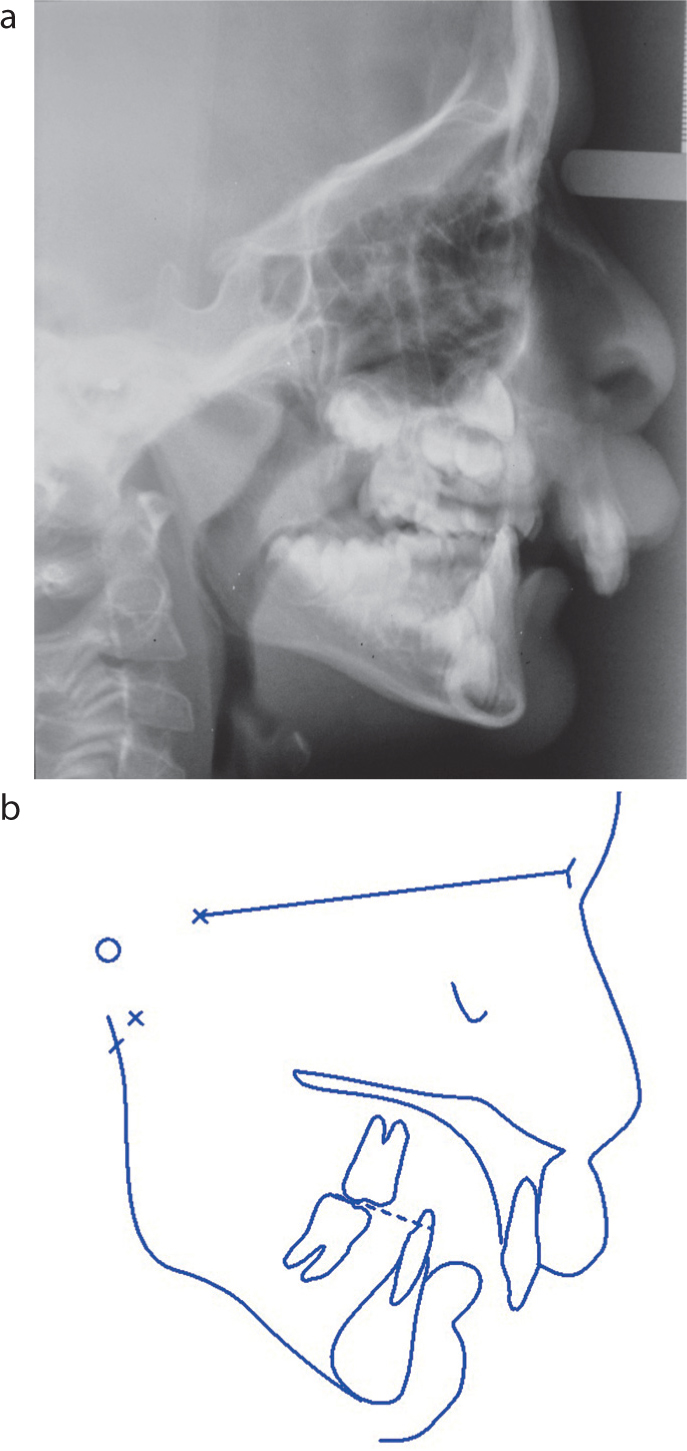
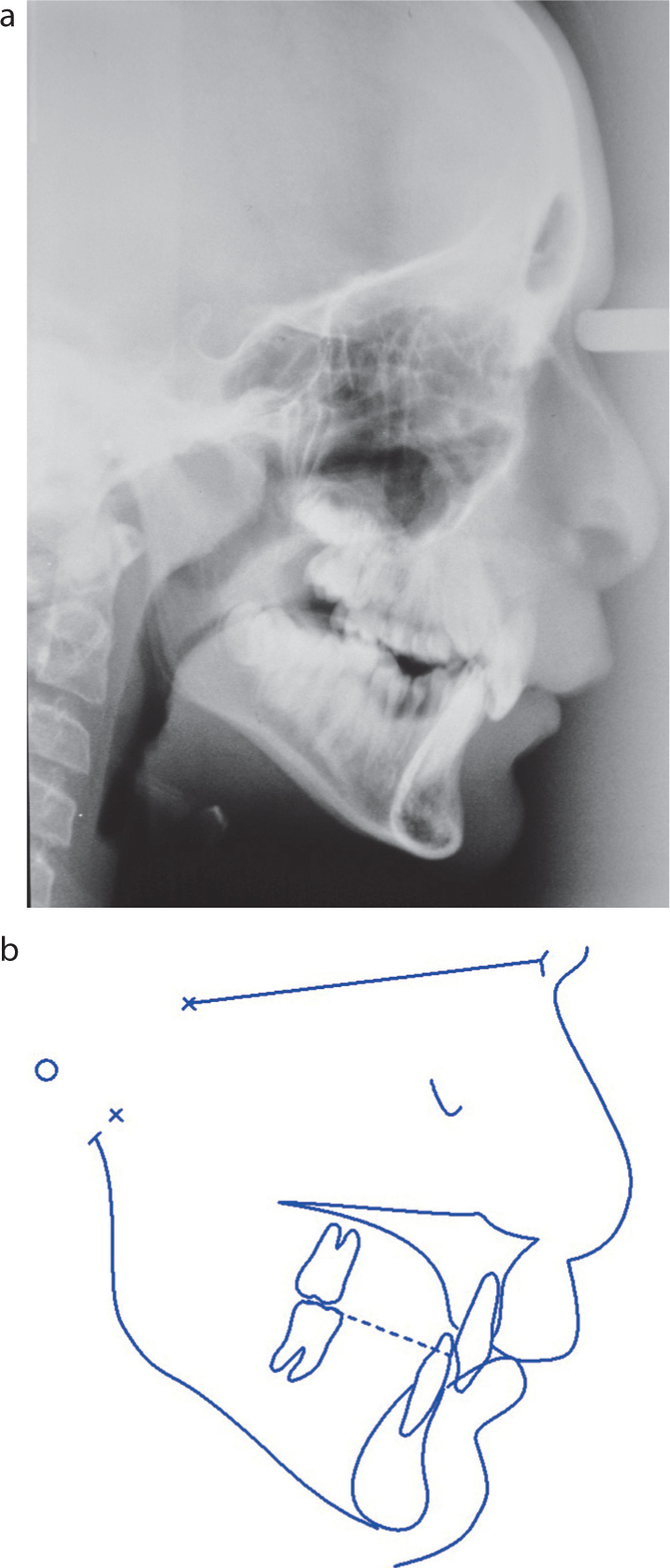
Plain film lateral cephalograms were taken at the start of his treatment (Figure 14), at the end of his functional appliance phase (Figure 15) and biennially in between. These radiographs were then electronically digitized in order to generate computerized lateral cephalometric evaluations and tracings. For the regional maxillary and mandibular outlines, the radiographs were hand-traced, instead. For all of the craniofacial cephalometric superimpositions, registrations were made on the sella-nasion line at sella, while the regional superimpositions were made using Björk's mandibular and maxillary stable structures.25,26
Figure 14. The pre-functional appliance: (a) lateral cephalogram and (b) tracing.Figure 15. The post-functional appliance: (a) lateral cephalogram and (b) tracing.
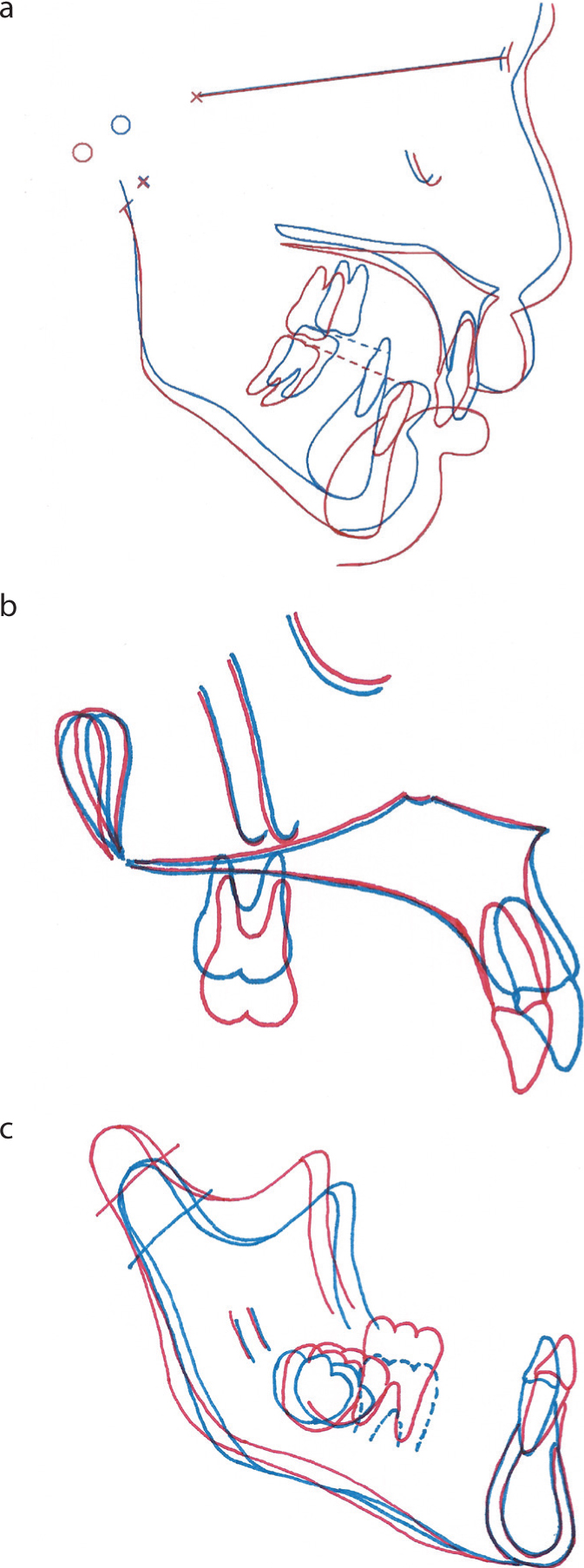
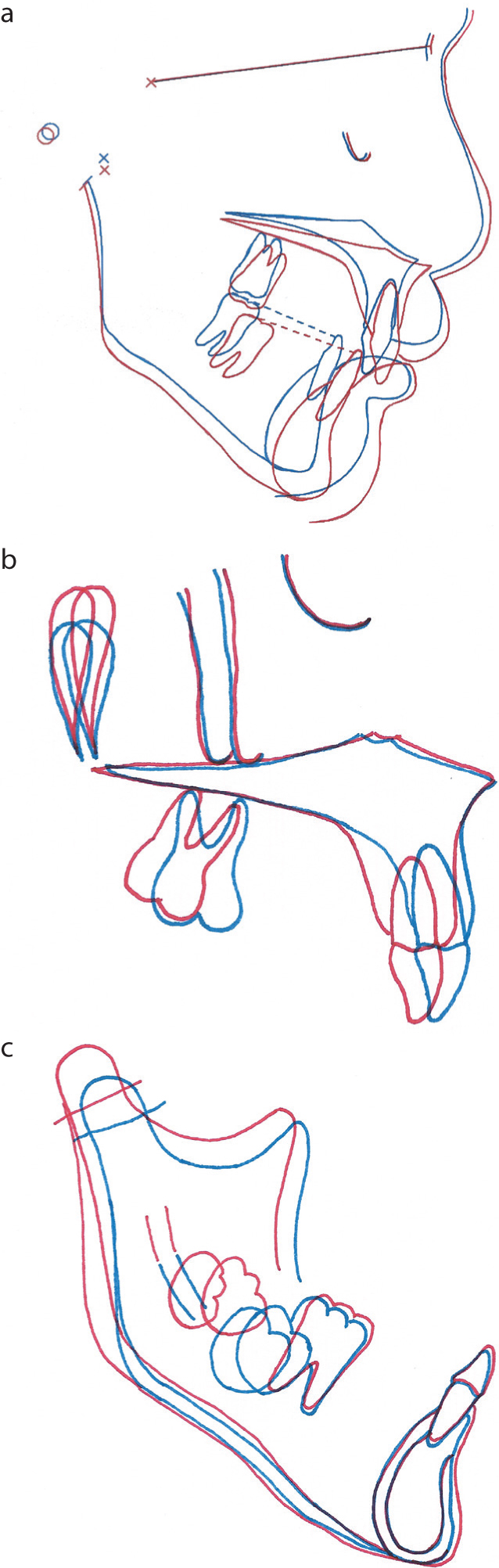
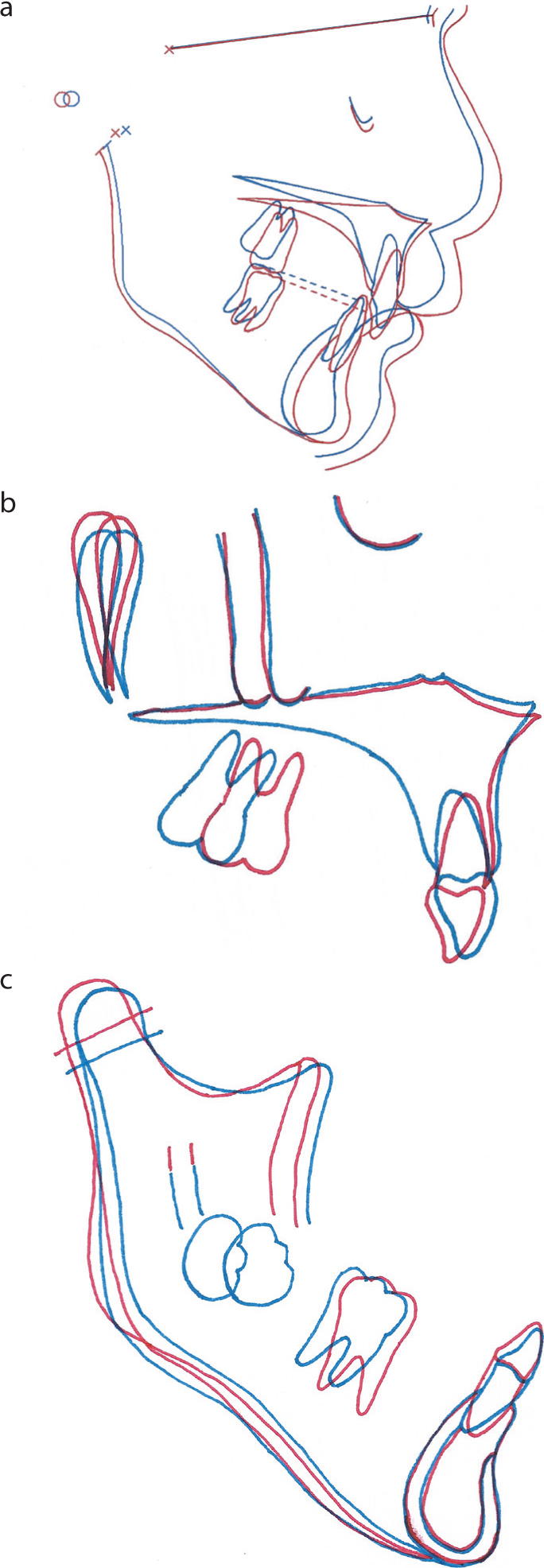
Figure 16 shows how in the first 2 years of full-time wear of the FR BCPPm and its nocturnal headgear, the downward and forward growth of the premaxilla was restrained and a forward and rather more downward development of the mandible was realized. In the maxilla, the upper molars erupted more than the incisors and these latter teeth retroclined noticeably. In the mandible, the lower first permanent molars erupted into the mouth and the lower incisors uprighted labially.
Figure 16. The (a) craniofacial, (b) maxillary and (c) mandibular regional cephalometric superimposition tracings after the first 2 years of treatment.
After the second 2 years of full-time wear, the growth of the premaxilla continued to be restrained and the mandibular pattern of growth became equally downward and forward (Figure 17). In the maxilla, the upper molars were tipped distally (perhaps as a consequence of the QH and the TPA that were used during this stage of the treatment) and the upper incisors appeared to be bodily retracted. In the mandible, there was minimal change in the position of either the molars or the incisors.
Figure 17. The (a) craniofacial, (b) maxillary and (c) mandibular regional cephalometric superimposition tracings after the second 2 years of treatment.
In the 2-year period when the FR BCPPm was then only worn at night while awaiting eruption of the permanent dentition, Figure 18 shows that the downward and forward restraint on the premaxilla continued, the palatal plane rotated slightly downwards at the back and the growth of the mandible was predominantly horizontal. In the maxilla, the upper molars moved forwards, back to their initial, pre-QH expansion and the TPA retained anteroposterior positions, and the upper incisors retroclined a little further. In the mandible, the lower molar crowns moved slightly forwards, with greater forward translation and anticlockwise rotation of their roots, while the lower incisors moved slightly lingually.
Figure 18. The (a) craniofacial, (b) maxillary and (c) mandibular regional cephalometric superimposition tracings after 2 years of nocturnal retention.
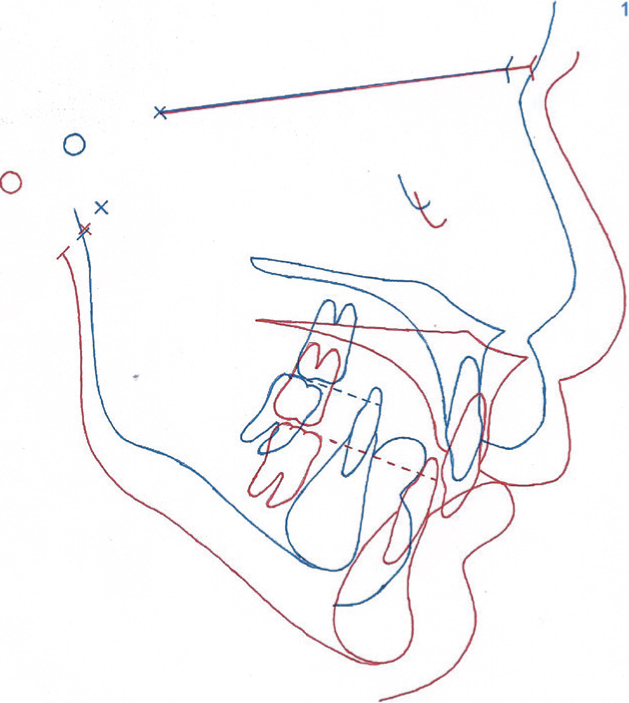
The total effect that the FR BCPPm had on the teeth and facial skeleton during the entire 6-year period of its use may be seen in the cephalometric superimposition of Figure 19, while Figure 20 illustrates the clinical outcome at the end of the functional appliance treatment, namely a Class II division 2 malocclusion with retroclined upper incisors, a 13.5-mm reduction in the original overjet, a 2-mm reduction in the increased, complete overbite, a bilateral Angle's Class I molar relationship, consolidated alveolar bone grafts and the development of lower-arch crowding.
Figure 19. The craniofacial cephalometric superimposition tracing at the end of 6 years of functional appliance treatment.Figure 20. The (a–c) extra- and (d–h) intra-oral views at the end of the functional appliance treatment. (Figure 20 d–h reproduced by kind permission of SAGE Publications Inc.)1
From this point, the patient progressed to a second stage of non-extraction fixed-appliance treatment, in order to complete the correction of his residual malocclusion.1
Summary
The design features of the FR BCPPm are presented which, in conjunction with other detailed publications on the laboratory construction of function regulators,7,9,12,14 may be used to replicate this novel, hybrid Fränkel functional appliance for use in other patients with bilateral cleft-related prominent premaxillae.
From this single case, for an FR BCPPm and its corollary QH to be able to restrain the premaxilla, reduce the alveolar gaps, correct the crossbites and level the maxillary occlusal plane prior to the insertion of ABGs, clinicians treating other bilateral cleft patients with a similar degree of premaxillary protrusion should allow a lead-in time of 2–3 years ahead of the age when it is estimated the patient will be developmentally ready for their bone grafts.