Hansa I, Semaan S, Ferguson D. Remote monitoring and ‘tele-orthodontics’ – concept, scope and applications. Semin Orthod. 2018; 24:470-481 https://doi.org/10.1053/j.sodo.2018.10.011
Cook J, Mullings C, Vowles R Online orthodontic advice: a protocol for a pilot teledentistry system. J Telemed Telecare. 2001; 7:324-333 https://doi.org/10.1258/1357633011936958
Stephens CD, Cook J. Attitudes of UK consultants to teledentistry as a means of providing orthodontic advice to dental practitioners and their patients. J Orthod. 2002; 29:137-142 https://doi.org/10.1093/ortho/29.2.137
Mandall NA, O'Brien KD, Brady J Teledentistry for screening new patient orthodontic referrals. Part 1: A randomised controlled trial. Br Dent J. 2005; 199:659-662 https://doi.org/10.1038/sj.bdj.4812930
Berndt J, Leone P, King G. Using teledentistry to provide interceptive orthodontic services to disadvantaged children. Am J Orthod Dentofacial Orthop. 2008; 134:700-706 https://doi.org/10.1016/j.ajodo.2007.12.023
Crawford E, Taylor N. The effective use of an e-dentistry service during the COVID-19 crisis. J Orthod. 2020; 47:330-337 https://doi.org/10.1177/1465312520949557
Rahman N, Nathwani S, Kandiah T. Teledentistry from a patient perspective during the coronavirus pandemic. Br Dent J. 2020; 1-4 https://doi.org/10.1038/s41415-020-1919-6
Greenhalgh T, Wherton J, Papoutsi C Beyond adoption: a new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. J Med Internet Res. 2017; 19 https://doi.org/10.2196/jmir.8775
Donaghy E, Atherton H, Hammersley V Acceptability, benefits, and challenges of video consulting: a qualitative study in primary care. Br J Gen Pract. 2019; 69:e586-e594 https://doi.org/10.3399/bjgp19X704141
Wherton J, Shaw S, Papputsi C Guidance on the introduction and use of video consultations during Covid-19: important lessons from qualitative research. BMJ Leader. 2020; 4:120-123 https://doi.org/10.1136/leader-2020-000262
Rockwell KL, Gilroy AS. Incorporating telemedicine as part of COVID-19 outbreak response systems. Am J Manag Care. 2020; 26:147-148 https://doi.org/10.37765/ajmc.2020.42784
Iacobucci G. Online consulting enthusiasts must engage with criticism, says GP leader. BMJ. 2018; 362 https://doi.org/10.1136/bmj.k4045
Dunbar AC, Bearn D, McIntyre G. The influence of using digital diagnostic information on orthodontic treatment planning – a pilot study. J Healthc Eng. 2014; 5:411-427 https://doi.org/10.1260/2040-2295.5.4.411
Saccomanno S, Quinzi V, Sarhan S Perspectives of tele-orthodontics in the COVID-19 emergency and as a future tool in daily practice. Eur J Paediatr Dent. 2020; 21:157-162 https://doi.org/10.23804/ejpd.2020.21.02.12
Mandall NA, Qureshi U, Harvey L. Teledentistry for screening new patient orthodontic referrals. Part 2: GDP perception of the referral system. Br Dent J. 2005; 199:727-729 https://doi.org/10.1038/sj.bdj.4812969
The objective of this study was to assess the feasibility and acceptability of conducting remote new patient consultations using teleorthodontics. Part 1 of the study used a five-point Likert-scale patient questionnaire and Part 2 comprised an orthodontist service evaluation assessing: (1) ease of use; (2) effectiveness; (3) reliability; (4) patient satisfaction; and (5) orthodontist satisfaction and outcome. The results for Part 1 showed that overall, 99% of patients reported that the system was easy to use, while 98% felt that it met their needs and 91% would choose to consult with a healthcare professional in a remote consultation in the future. For Part 2, 87% of orthodontists reported the remote consultation system worked well. Orthodontists were unable to identify the IOTN in 11% of cases and 11% required a further face-to-face appointment for imaging or clinical examination. In conclusion, teleorthodontics has the potential to augment traditional clinical services, such as during the COVID-19 pandemic, and beyond. An overwhelmingly positive response towards teleorthodontics was obtained from patient and specialist orthodontist stakeholders.
CPD/Clinical Relevance: The teleorthodontic system demonstrates improved patient and orthodontist acceptance and feasibility and can deliver good outcomes.
Article
Teleorthodontics is a broad term that encompasses remote provision of orthodontic care, advice, or treatment via information technology rather than a conventional face-to-face consultation (FTFC).1 As a concept, it is something that may have been previously considered as a fledgling idea in orthodontics. With the imperative to reduce FTFCs due to the COVID-19 pandemic, the prospect of using information technology and connectivity to replace traditional face-to-face appointments with remote consultations (RCs) was thrust into the limelight.
Until very recently, examples of teleorthodontics in the literature were scarce but included some examples of orthodontic specialists or consultants engaging with general dental practitioners (GDPs) in order to facilitate treatment remotely in order to make specialist advice more accessible.2,3,4,5
More recently with the burgeoning increase of clear aligner therapy, and as the development, ease of use and accessibility of technology has grown exponentially, there has been growing interest in how the remote monitoring of appliances may improve patient convenience, whilst reducing chairside clinical time, such as through the use of applications such as Dental Monitoring (https://dental-monitoring.com).1
With the world now wholeheartedly embracing video-calling applications as a convenient and secure method of communication, it seems likely that, even after the ramifications of the COVID-19 pandemic have dissipated, increased use of RCs will still be seen as desirable.6 There will still be a need to deliver a service that is cost effective, patient-centred and efficient.
It is therefore important that any orthodontic professionals involved in RCs ensure that they are aware of the limitations, as well as the benefits, of teleorthodontics. It remains important that both the quality and the effectiveness of an RC-driven service is evaluated.
This service evaluation appraises the stakeholder experience when using RC for new orthodontic patient consultations.
Objective
The objective was to conduct a clinical service evaluation, with the primary outcome of assessing the feasibility and acceptability of conducting new patient (NP) RCs, and a secondary outcome of identifying the barriers and facilitators to this intervention.
Methods
In response to the COVID-19 lockdown restrictions, Queensway Orthodontic group in north-east England implemented a secure virtual clinical system, Doxy.me (Rochester, NY, USA). Of concern with any online solution in healthcare is confidentiality. Doxy.me is a fully Health Insurance Portability and Accountability Act 1996 (HIPAA) and GDPR compliant solution, with encrypted point-to-point connections and provides a business associate agreement to ensure the security of the protected health information.7 Doxy.me offers a robust browser-based platform that requires no software installation, allows interface customization, an appointment management system, embedded teleconsent forms, live chat functions and video-chat sessions.
Over a 4-week period, consecutive NPs in five orthodontic practices belonging to the Queensway Orthodontic group, were selected for participation in this service evaluation. Historically, these patients would have been offered a FTFC for a NP assessment as a first contact. The protocol developed for managing these clinics remotely is shown in Table 1.
Actions prior to the RC
Patient is offered a virtual new patient consultation with an orthodontist
If the patient agrees, they are given an appointment time and sent guidance and link (with video instructions) to upload photos of their teeth to the patient management system, prior to the consultation. Photographs are assessed against a quality standard sheet prior to being accepted for a consultation
The patients are informed of the service level evaluation study being carried out via an information sheet which is sent via email prior to the appointment
Actions during the RC
Patient logs into the virtual waiting room at the agreed time. If the patient is late, they are contacted via email or telephone by the orthodontist
Orthodontists join the call and complete introductions and ensure patient identity is confirmed and ensure parent/guardian is present
Verbal consent is gained at the beginning of the remote consultation and new patients will be invited to complete an anonymized online satisfaction questionnaire using Wufoo.com sent to their email
Orthodontist to take a history of the problem as per conventional face-to-face appointment
Orthodontist to assess photographs provided by the patient and imaging sent by the GDP in the referral
Orthodontist to report the outcome of appointment and communicate this to the patient/person with parental responsibility
Actions after the RC
Orthodontist to document the consultation
Orthodontist to risk stratify the patient and arrange appropriate outcome, eg NHS waiting list, priority NHS waiting list, face to face appointment, review, rejection of referral
Orthodontist to complete service evaluation data collection form
The teleorthodontic model used was a combination of real-time video consultations with the patient (and person with parental responsibility), alongside radiographs from the GDP from the referral and/or intra-oral photographs provided in advance by the patient, to aid decision-making. If additional diagnostics or a clinical examination were required, an FTFC was arranged. Inappropriate referrals were triaged, and the correspondence to the referrer discussed the reasons for rejection of the referral on each occasion.
The core features of an orthodontic NP consultation were identified (Table 2). The RC process evaluated in this study is compared to this ‘baseline standard’, with the following key features:
Allows for a comprehensive dialogue between the patient (and/or person with parental responsibility) and the orthodontist;
Enables an appropriate NP consultation remotely, that allows sufficient information to be gathered in order to triage patients and assign them to the most appropriate treatment pathway;
Patient intra-oral photographs have been uploaded to the patient management system, prior to the consultation;
Uses a secure and stable IT platform in line with GDPR and data governance standards.
1
Orthodontic referral is made by GDP and triaged by an orthodontist
2
Appointment generated and sent in the post to patient
3
The patient attends the orthodontic practice to see the orthodontic professional
4
The orthodontic professional undertakes a comprehensive history taking including: patient's complaint and motivation; dental history; medical history and social history. Followed by an extra- and intra-oral clinical examination
5
If required, records are taken
6
IOTN diagnosis provided
7
Treatment options are provided and discussed. An opportunity to answer any questions
Inclusion and exclusion criteria
The inclusion criteria were:
NHS NPs referred by their GDPs to Queensway Orthodontics for an orthodontic assessment;
Patients aged under 18 at the time of referral receipt.
The exclusion criteria were:
Patients who declined to participate in an RC;
Private patients and patients attending for reviews and second opinions.
The evaluations
Patient survey
Part 1 of the anonymized patient survey collected information on patient demographics and familiarity with telehealth. Part 2 comprised four domains using a five-point Likert-scale: (1) ease of use; (2) effectiveness; (3) reliability of the teleorthodontic system; and (4) patient satisfaction. Questions were adapted from a teledentistry service evaluation by Rahman and colleagues.8
Orthodontist service evaluation
Part 1 collected information on patient demographics, attendance behaviour and IOTN diagnosis. Part 2 comprised four domains using a five-point Likert-scale: (1) ease of use; (2) effectiveness; (3) reliability of the teleorthodontic system; and (4) orthodontic professional satisfaction. Part 3 documented the outcome from the RC.
Survey distribution
Using Doxy.me, patients were offered scheduled RCs as a NP appointment. The patients were informed of the service level evaluation study being carried out with an information sheet sent via email, prior to the appointment (Table 1). After the RC, patients were invited to complete an anonymized online satisfaction questionnaire using Wufoo.com, which was sent to the email address the patient had provided (in accordance with GDPR and practice data governance policy).
Four orthodontist specialists completed the service evaluation data collection form following completion of the RC.
Data analysis
Completed responses were entered into an Excel spreadsheet anonymously and analysed (Version 16.43). Cronbach's statistical analysis was completed to determine internal consistency of the patient survey questions. The Fisher's exact test was used to determine any statistical difference in patient responses according to gender.
Results
Demographics and professional characteristics of participants
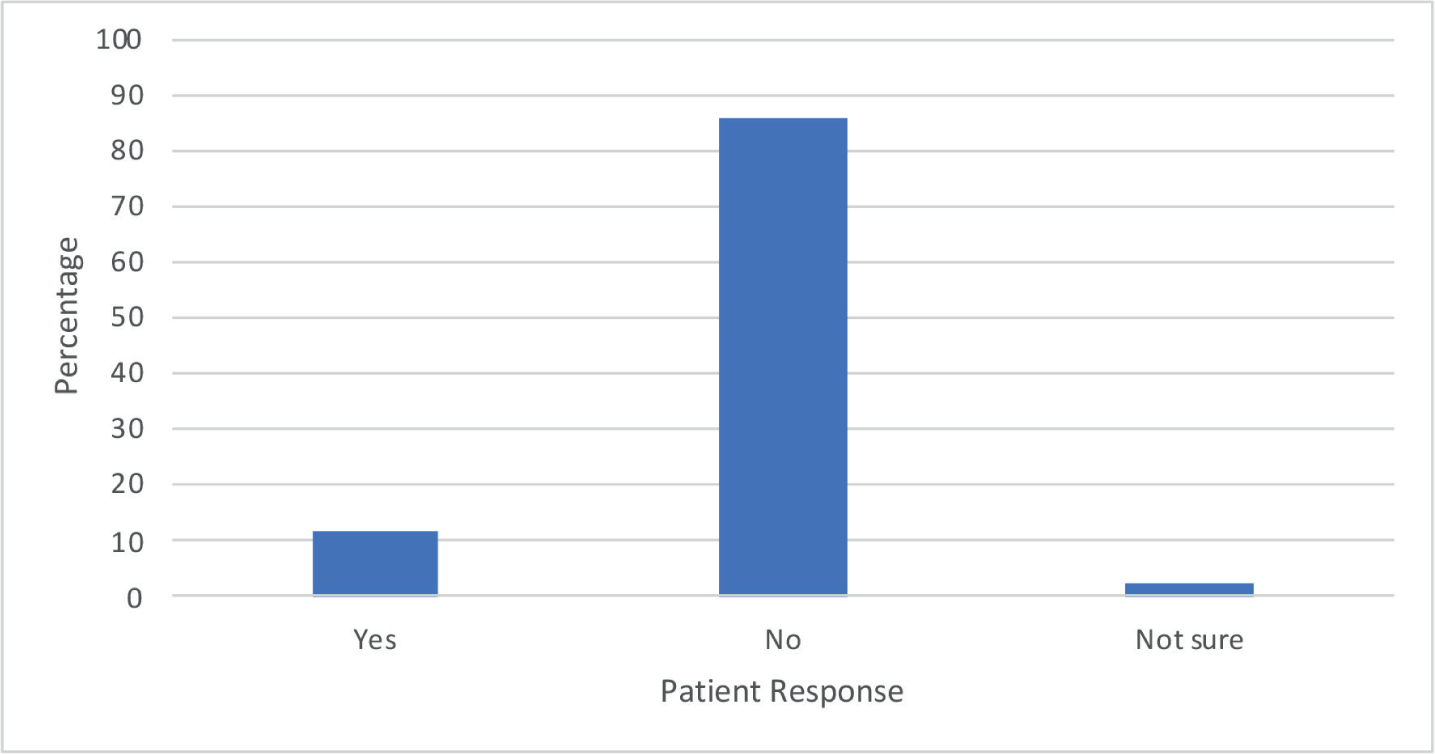
In total, 93 patient survey forms were completed, and 159 service evaluation forms were completed by four orthodontists; 23 of which reported the patient ‘was not brought’ (WNB). The patient age range was 6–18 years of age, with a mean age of 13 years (Table 3). The ratio of female to male patients was 3:2. Of the patient participants, 86% reported no previous experience using telehealth (Figure 1). Over the 4-week period no patients declined the RC and requested an FTFC.
Patient survey response
Orthodontist survey response
Characteristics
Age range (years)
6–18
6–18
Mean age (SD)
13 (2.1)
13 (2.3)
Gender
Female
56 (60%)
92 (58%)
Male
37 (40%)
67 (42%)
Figure 1. A bar chart to show previous experience with telehealth.
Ease of use of the teleorthodontic system
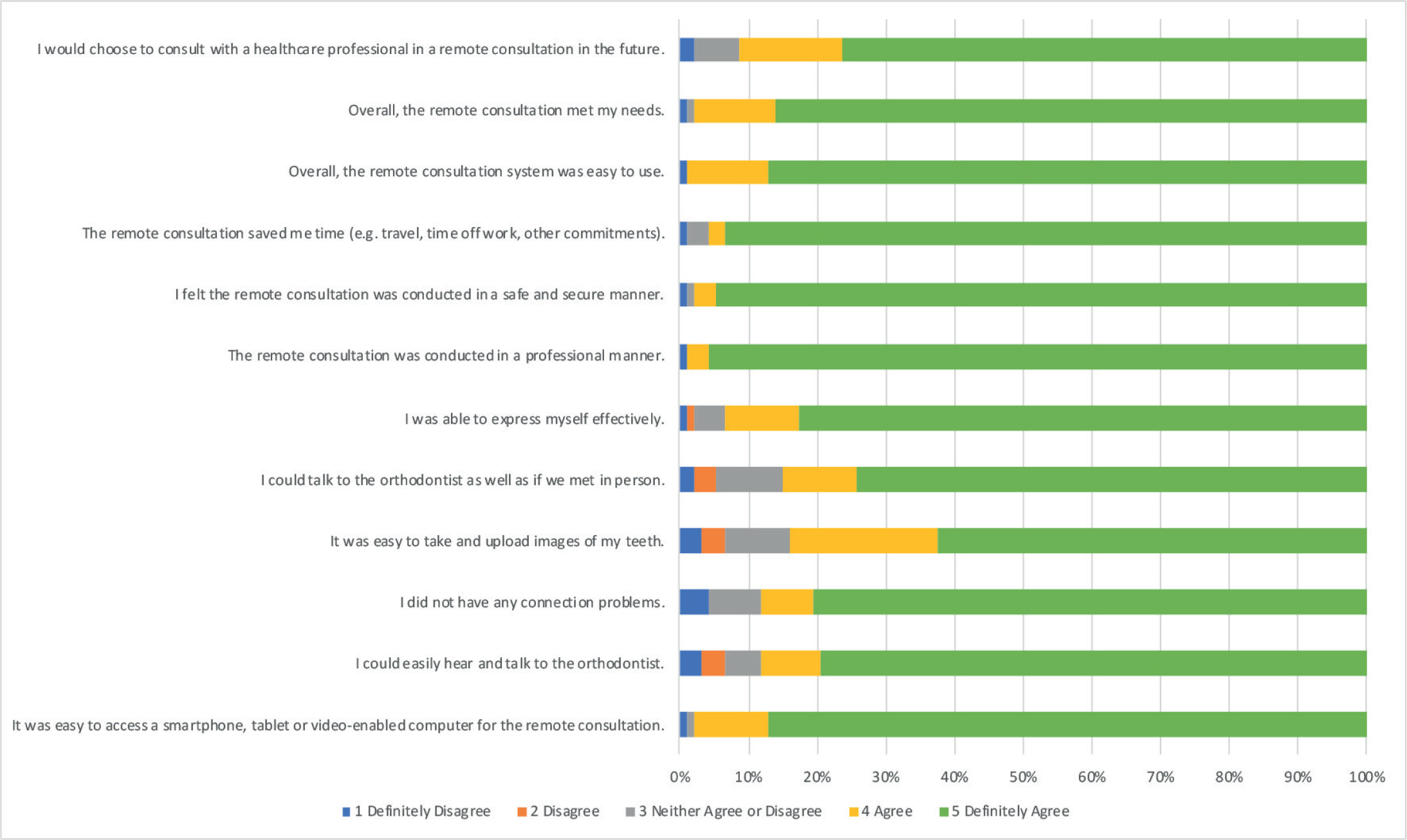
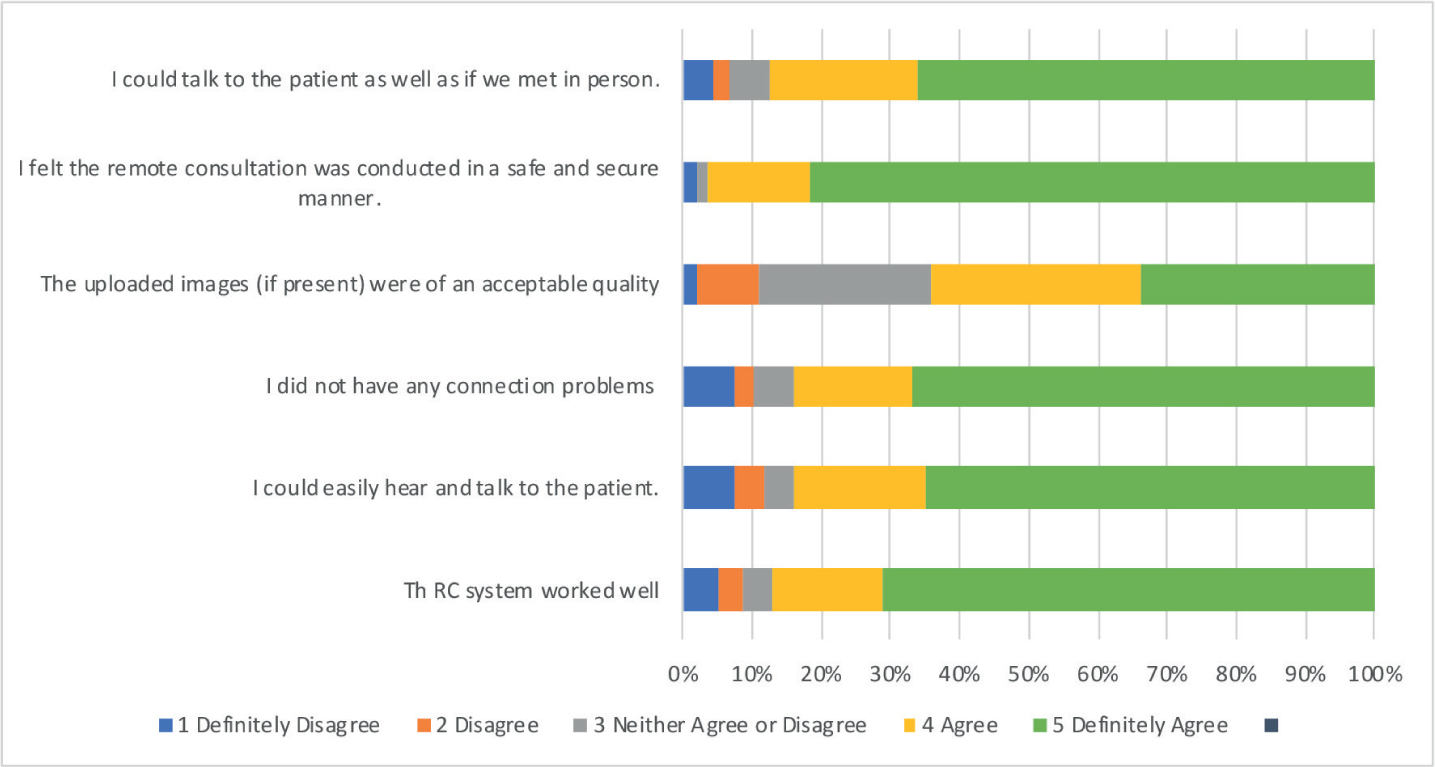
The majority of patients reported that the system was easy to use (99%) and felt it was easy to access a smartphone, tablet or video-enabled computer for the RC (98%) (Figure 2). In total, 84% of patients reported that it was easy to upload the images of their teeth prior to the appointment; however, only two-thirds of the photographs were reported to be of acceptable quality by the orthodontist (Figure 3). The most frequent criticism was that unacceptable images were ‘too dark to make an orthodontic assessment’. In one-third of cases, orthodontists neither agreed nor disagreed that the quality of the photographs provided were of acceptable quality and reported that, although ‘the photographs [were] not good enough to complete the whole orthodontic assessment, they could identify…the need for orthodontic treatment’ and patients were placed onto appropriate waiting lists.
Patient respondents (89%) and orthodontist specialists (84%) agreed or definitely agreed that they could easily hear and speak, while 6% of patients stated that they could not hear the orthodontist and so a subsequent telephone call was carried out. The remaining patients (5%), who neither agreed or disagreed, reported that, ‘the sound quality was poor, but the orthodontist resolved the issues promptly using a combination of phone call for sound and online for video.’
Effectiveness including increasing access
In total, 94% of patient respondents reported that they were able to express themselves clearly (Figure 2). Many commented that the RC was an effective form of communication, and that being at home made them feel at ease, particularly during ‘these troubled times’ and therefore better able to absorb information. One parent commented that it is a great way for her son, diagnosed with autistic spectrum disorder (ASD), to first meet the orthodontist online; the RC acting as a proxy visual aid.
Similarly, 85% of patients and 87% of orthodontists reported that they could talk to the other as if they met in person (Figures 2 and 3). Explanations made by the orthodontist for compromised communication included, connection problems (5/21), non-English speaking patient (1/21), technology/hardware problem (7/21), patient co-operation (3/21) and patient sensory impairment (2/21). One orthodontist reported that they felt that the mother was ‘taking over’ the remote consultation and that during chairside consultations, it can be easier to talk to the patient directly owing to non-verbal cues, such as body positioning and eye contact. Compromised communication was never used for the justification of the outcome of the RC.
Reliability of the teleorthodontic system
The majority of patient respondents and orthodontist specialists felt that the RC was conducted in a safe and secure manner (98% and 99%, respectively). Connection problems were reported by 10% of orthodontists who stated that they had ‘difficulty connecting due to server.’ This seemed to be particularly when using the Safari internet browser and orthodontists needed ‘to restart the system multiple times’ (Figure 3).
Almost all patients (99%) felt that the RC was conducted in a professional manner.
Patient satisfaction
The feedback on the potential merits of teleorthodontics to patients was extremely positive and highlighted that it would save time on travel, car parking and in the waiting room. The vast majority of participants (99%) reported that the RC met their needs, and that they would use the virtual clinic again if given the option (Figure 3). Patient comments were extremely positive stating that, ‘[it is] so much easier having the meeting like this, much preferred’, ‘very easy to use!’ and ‘it was great to save time at this stage of the process.’
Orthodontist satisfaction and outcome
Most orthodontists (87%) reported that the RC system worked well: 84% of all patients attended the consultation on time, and did not require contacting prior to the appointment (Figure 4). However, 14% of patients were not contactable, and the outcome of the RC was that the patient WNB.
Figure 4.
(a) Bar chart to show whether patient required contacting by orthodontist. (b) Pie chart to represent the percentage of patients attending the remote consultation on time. Data obtained from the orthodontic service evaluation.
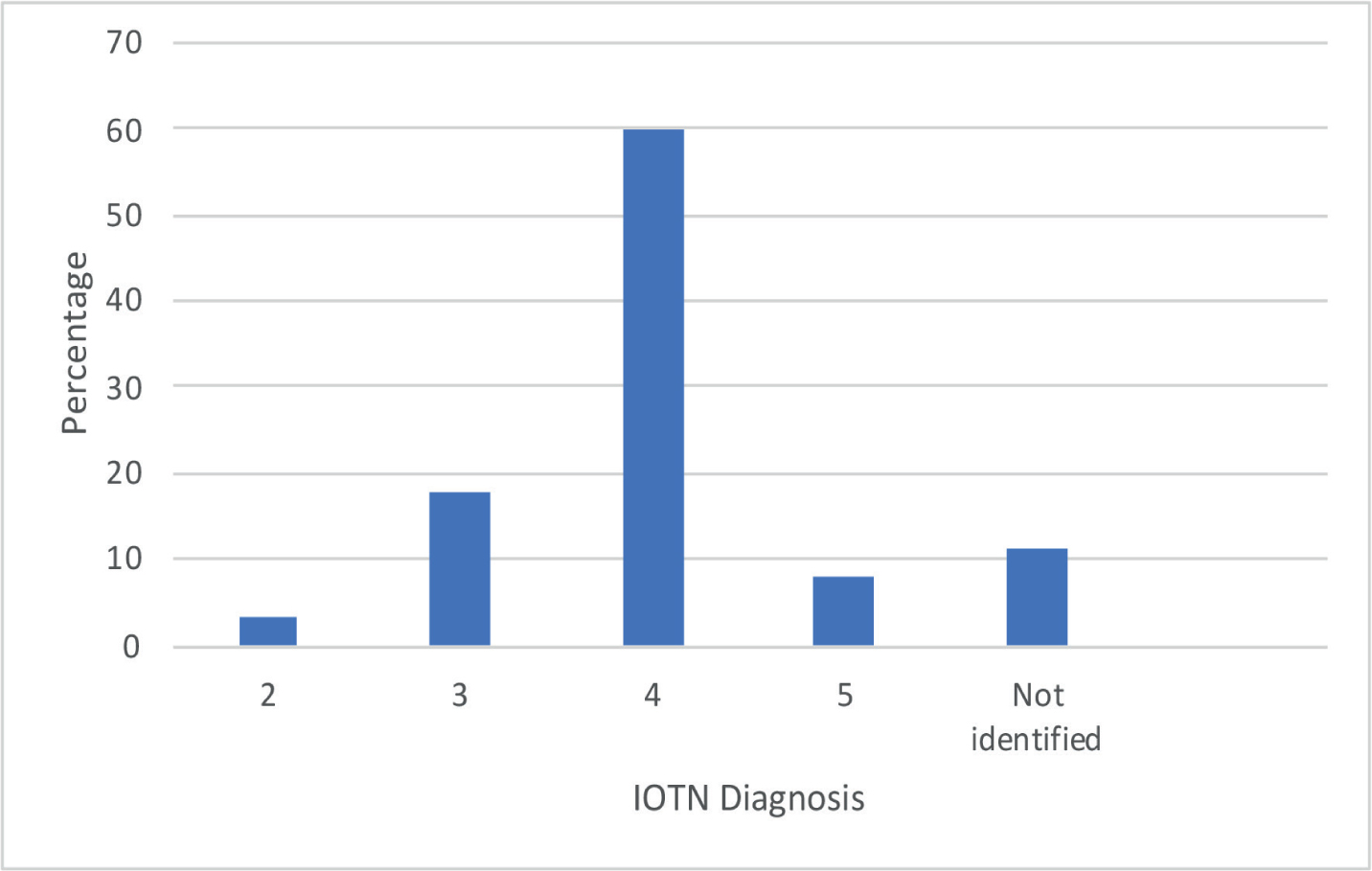
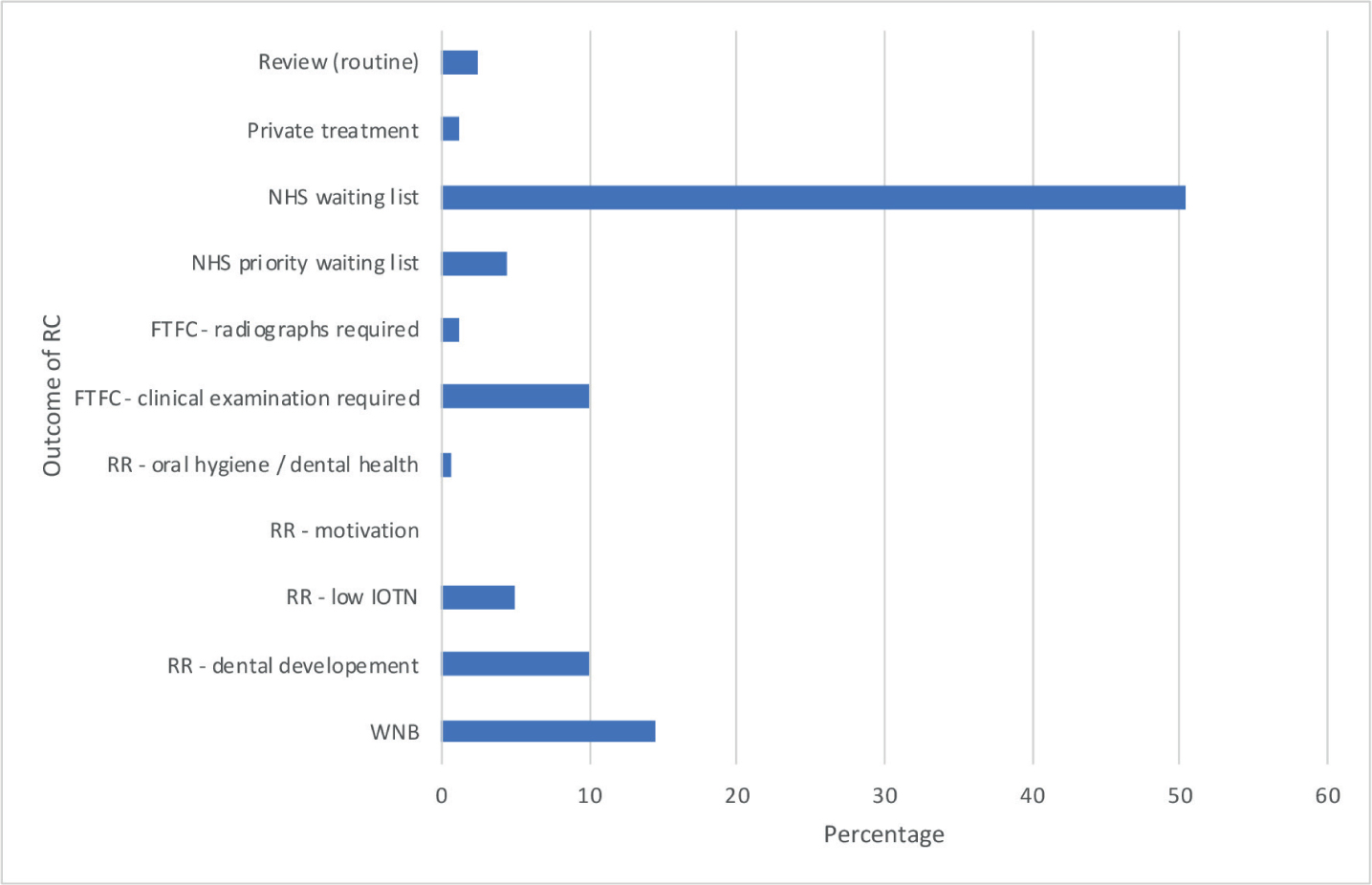
Orthodontists were unable to identify the IOTN in only 11% of cases (Figure 5). Half of all consultations resulted in the patient being placed on the NHS waiting list, a further 4% on the priority NHS waiting list and 16% of patient referrals were rejected due to inadequate dental development, suboptimal oral hygiene and not meeting the IOTN threshold for treatment. A subsequent FTFC was required for 11% because radiographs were required (1%) or a clinical examination to allow a full assessment of the problems (10%) was needed (Figure 6).
Figure 5. IOTN diagnosis following the remote consultation.Figure 6. Outcomes from the remote consultation. WNB: was not brought; FTFC: face-to-face consultation; RR: referral rejection.
Simple statistics
Good internal consistency of the patient survey questions was revealed by Cronbach's alpha analysis at 0.88. A significantly higher Cronbach score would otherwise suggest that some questions were redundant. The Fisher's exact test showed no statistically significant difference between male and female patients (P>0.5) across all questions.
Discussion
Implementation theory9 suggests that, to be successful, any telehealth system must be simple to use, must also be seen to be an advance over existing technology, and ideally integrate with existing work patterns and surgery computer systems. Although, Doxy.me was implemented and evaluated in this study, the authors recognize that other HIPAA-compliant video consultations are available, for instance, Attend Anywhere (AA), Zoom for Healthcare and VSee. AA is already used nationally by NHS Scotland and extensively across England and Wales. To use AA, participants are required to have the Google Chrome web browser or can download an app for Apple devices.10 Zoom for Healthcare includes tools designed for the telemedicine industry, including integrations with medical devices and electronic health records, but does not offer services such as billing features or appointment scheduling. VSee enables a pan–tilt–zoom camera control that is helpful for remote examinations.
Several challenges with video consultations have been reported (Table 4),10 and selecting the most appropriate video platform as one way of reducing these challenges is important. Learning from the experiences of our medical colleagues who have used video applications is particularly beneficial.10,11 Local policies and procedures should be formulated and agreed upon by the practice, including a working-from-home policy if RCs are going to be undertaken from home, and an appropriate risk assessment must also be carried out. The orthodontist should also be familiar with their indemnity provider's guidance regarding the use of RCs to ensure that they comply, as well as regularly checking for any updates in guidance from the General Dental Council as this technology develops.12
Internet connection interruptions
Software malfunction
Accessibility
Resistance to change
Potential for increased administration burden
Missed non-verbal cues and implications for child protection
Medico-legal concerns
Costs for implementation
Data protection concerns
Quality of photographs provided by patients
Connecting remotely provides the ability to assess patients in their own homes, in a known and safe non-clinical environment. A reduction in footfall and clinical contacts, prevents unnecessary exposure of patients to COVID-19 or asymptomatic carriers, including healthcare workers13 and improves safety of medically compromised groups.
When active orthodontic interventions are not required, RCs offer convenience, avoid the need for travel, reduce pressures on car parking and associated costs. Staff are able to provide an outpatient service for those patients in self-isolation or those with childcare responsibilities.
Teleorthodontics is an innovative method of health service delivery that can aid triaging of orthodontic patients and stratifying the outcome of the consultation. To our knowledge, this is the first study that evaluated the use of teleorthodontics from a patient and orthodontist perspective during the COVID-19 pandemic, in primary care. Our results show that the overwhelming majority of patients and orthodontists were extremely satisfied with using teleorthodontics in all five domains: ease of use; the effectiveness (including increasing access to clinica services); reliability of the teleorthodontic system; patient and orthodontist satisfaction. Patients reported that they would be happy to consult with a healthcare professional using RC in the future.
Stakeholder feedback and engagement is very encouraging. Similarly, RCs can be implemented in other areas of orthodontic care, where active treatment or adjustments are not required. Emergency appointments, retainer reviews, treatment reviews, growth and development reviews and MDT consultations have been evaluated using e-dentistry.6 Owing to the practical nature of orthodontic treatment, teleorthodontics can only ever augment traditional clinical appointments.
The benefits of RCs need to be considered against potential risks that include missed diagnoses and health inequalities due to a digital divide,14 legal issues due to patient confidentiality,15 diminished patient–orthodontist rapport16 and missed safeguarding needs.17
Clinicians must be vigilant since there is a risk that referrals may be rejected inappropriately and had the patient been seen for a FTFC, their orthodontic need may have been identified. For four patients in the study, an IOTN diagnosis could not be made from the information gathered during the RC and the referral was rejected without offering a FTFC. The reasons for rejection of these referrals despite a lack of IOTN diagnosis included poor oral-hygiene and insufficient dental development. A way to safeguard against potential misdiagnosis could be to arrange FTFC in cases where there is uncertainty based on the information gathered from the RC, and to always provide correspondence to the GDP advising them of why the referral was rejected.
The 2020 consumer digital index revealed that approximately 16% of people in the UK cannot undertake basic digital activities, such as turning on a device, connecting to wi-fi or opening an app.18 It is recognized that the most vulnerable, disadvantaged, elderly and persons with a physical or learning disability are most likely to be digitally excluded and this can contribute to worsening healthcare inequalities. Feedback from one parent of a patient diagnosed with ASD, however, reported to the contrary; the RC acted as a proxy visual aid and assisted in acclimatizing her son to the orthodontist responsible for his ongoing treatment.
The Royal College of Paediatric and Child Health recommend the approach for RCs should be the same as that adopted for FTFC when assessing a child's safety, presence of a chaperone and a child's ability to make decisions.17,19 While potentially offering an insight into a young person's home environment, safeguarding needs can be missed, such as subtle non-verbal cues. Use of digital consultations should be combined with a consistently low threshold for FTFC should there be any suggestion of safeguarding concerns.
Similarly, WNB pathways should also be followed in respect to virtual appointments. NHS Improvement20 highlighted factors that affect the missed appointment rate and include the distance that patients need to travel, plus the requirement for patients (or parents) to get time off work (or school). NHS Improvement anticipated that both of these factors would be either removed or alleviated by the introduction of virtual consultations. Interestingly, the WNB rate (14%) was doubled following the implementation of the RC system, when compared to the FTFC pre-COVID WNB data. The sample size of this study is, however, small and may not be strictly comparable to pre-COVID rates.
NP consultations rely on good-quality patient records and it is been suggested that first visits/NP appointments must be carried out in-office.21 Importantly, a significant minority of patients were deemed to benefit from an FTFC, as a clinical examination or supplemental radiographs were required. The former was often a consequence of suboptimal photographs taken by the patient prior to the consultation. Some may perceive an FTFC outcome as a failure from this teleorthodontics system; however, the RC is invaluable for service preparedness planning, where initial history taking, and consent can take place. The FTFC that follows would include the examination, investigations if required, confirmation of diagnosis and treatment, potentially, in one clinical contact.
GDPs are reported to generally support teleorthodontics for NP orthodontic referrals. Mandal and colleagues in 2005 carried out a randomized control trial, in which GDPs had to provide patient demographics, history, overjet, extra- and intra-oral photographs and radiographs electronically. GDPs were, however, concerned about the costs, increased surgery time and remuneration.22 Providing appropriate resources to support patients in taking their own photographs can aid in minimizing surgery time. Patient involvement in obtaining good records is advocated by the British Orthodontic Society.23 Queensway Orthodontics provide instructional videos for patients to take their own photographs using tablespoons as cheek retractors. Potentially this service could evolve to provide the patient with examples of suboptimal photographs, such as those with insufficient lighting, to improve the acceptability of the images.
Remote consulting presents particular challenges for young people and carries potential risks, such as safeguarding and digital exclusion due to socio-economic status and access to technology. Further research is needed to assess whether RCs contribute to worsening healthcare inequalities for orthodontic patients. Despite the vast positive patient feedback, teleorthodontics will not suit all orthodontic patients. Retaining choice and control over how to consult will be critical.
Conclusion
Teleorthodontics has the potential to augment traditional clinical services, such as during the COVID-19 pandemic and beyond. An overwhelming positive response towards teleorthodontics was obtained from patient and specialist orthodontic stakeholders. The applications of teleorthodontics should be assessed with future research, both in primary and secondary care.