Proffit WR, Phillips C, Dann C 4th. Who seeks surgical-orthodontic treatment?.. Int J Adult Orthodon Orthognath Surg. 1990; 5:153-160
Bailey LJ, Haltiwanger LH, Blakey GH, Proffit WR Who seeks surgical-orthodontic treatment: a current review. Int J Adult Orthodon Orthognath Surg.. 2001; 16:280-292
Fowler P, Haworth J, Steenberg L Vertical segmental anterior mandibular distraction to aid closure of a severe anterior open bite associated with an accentuated reverse curve of Spee. J Orthod.. 2021; 48:444-450 https://doi.org/10.1177%2F14653125211000056
Björk A, Skieller V Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod.. 1983; 5:1-46 https://doi.org/10.1093/ejo/5.1.1
Björk A Prediction of mandibular growth rotation. Am J Orthod.. 1969; 55:585-599
Linder-Aronson S Effects of adenoidectomy on dentition and nasopharynx. Trans Eur Orthod Soc. 1972; 177-86
Zheng W, Zhang X, Dong J, He J Facial morphological characteristics of mouth breathers vs. nasal breathers: A systematic review and meta-analysis of lateral cephalometric data. Exp Ther Med. 2020; 19:3738-3750 https://doi.org/10.3892/etm.2020.8611
Arat M, Iseri H Orthodontic and orthopaedic approach in the treatment of skeletal open bite. Eur J Orthod.. 1992; 14:207-215 https://doi.org/10.1093/ejo/14.3.207
Kiliaridis S, Egermark I, Thilander B Anterior open bite treatment with magnets. Eur J Orthod.. 1990; 12:447-457 https://doi.org/10.1093/ejo/12.4.447
Giancotti A, Garino F, Mampieri G Use of clear aligners in open bite cases: an unexpected treatment option. J Orthod.. 2017; 44:114-125
Proffit WR, Turvey TA, Phillips C The hierarchy of stability and predictability in orthognathic surgery with rigid fixation: an update and extension. Head Face Med. 2007; https://doi.org/10.1186/1746-160X-3-21
Bondemark L, Holm AK, Hansen K, Axelsson S, Mohlin B, Brattstrom V, Paulin G, Pietila T Long-term stability of orthodontic treatment and patient satisfaction. A systematic review. Angle Orthod.. 2007; 77:181-91 https://doi.org/10.2319/011006-16r.1
Arpornmaeklong P Shand JM, Heggie AA Skeletal stability following maxillary impaction and mandibular advancement. Int J Oral Maxillofac Surg.. 2004; 33:656-663 https://doi.org/10.1016/j.ijom.2004.01.004
Ow A, Cheung LK Skeletal stability and complications of bilateral sagittal split osteotomies and mandibular distraction osteogenesis: an evidence-based review. J Oral Maxillofac Surg.. 2009; 67:2344-2353 https://doi.org/10.1016/j.joms.2008.07.003
Mobarak KA, Espeland L, Krogstad O, Lyberg T Mandibular advancement surgery in high-angle and low-angle class II patients: different long-term skeletal responses. Am J Orthod Dentofacial Orthop.. 2001; 119:368-381 https://doi.org/10.1067/mod.2001.110983
Skeletal discrepancies. Part 2: assessment, aetiology and management of high angle cases Kyle Durman Hannah Batsford Peter Fowler Orthodontic Update 2025 16:3, 130-134.
Authors
KyleDurman
BS BDS DDS MOrth
Post-CCST Trainee in Orthodontics, Royal Devon and Exeter Hospital
This is the second article in a three-part series considering skeletal discrepancies in the vertical and transverse dimensions. Discrepancies in the vertical dimension are a relatively common finding, presenting challenges for the orthodontist in terms of treatment planning, management and relapse.
CPD/Clinical Relevance: This article aims to increase awareness of the aetiology and management of patients presenting with increased Frankfort/maxillary mandibular planes angle and anterior lower face height, commonly described as ‘high angle’.
Article
The vertical dimension is one of the three spatial planes used to assess orthodontic hard and soft tissue relationships. It is important to be able to assess the vertical dimension, understand the aetiology of the malocclusion and be able to manage patients with an increased Frankfort/maxillary mandibular planes angle (F/MMPA) and anterior lower face height (ALFH).
Definition of high angle and prevalence
The definition of ‘high angle’ in orthodontics is an increased F/MMPA more than one standard deviation above average (FMPA >32°).1 A high angle is associated with increased vertical facial proportions, with backward growth rotations of the mandible. Other terms used to describe a high angle include hyperdivergent, dolichofacial and long or adenoid face. Although these terms all refer to similar clinical features, the assortment of interchangeable terms indicate variations in facial morphology and possible aetiological features.
The prevalence of patients with a ‘long face’ is approximately 22%, and increased vertical proportions occur predominately in the lower third of the face, rather than the middle third of the face.2,3
Assessment of the vertical dimension
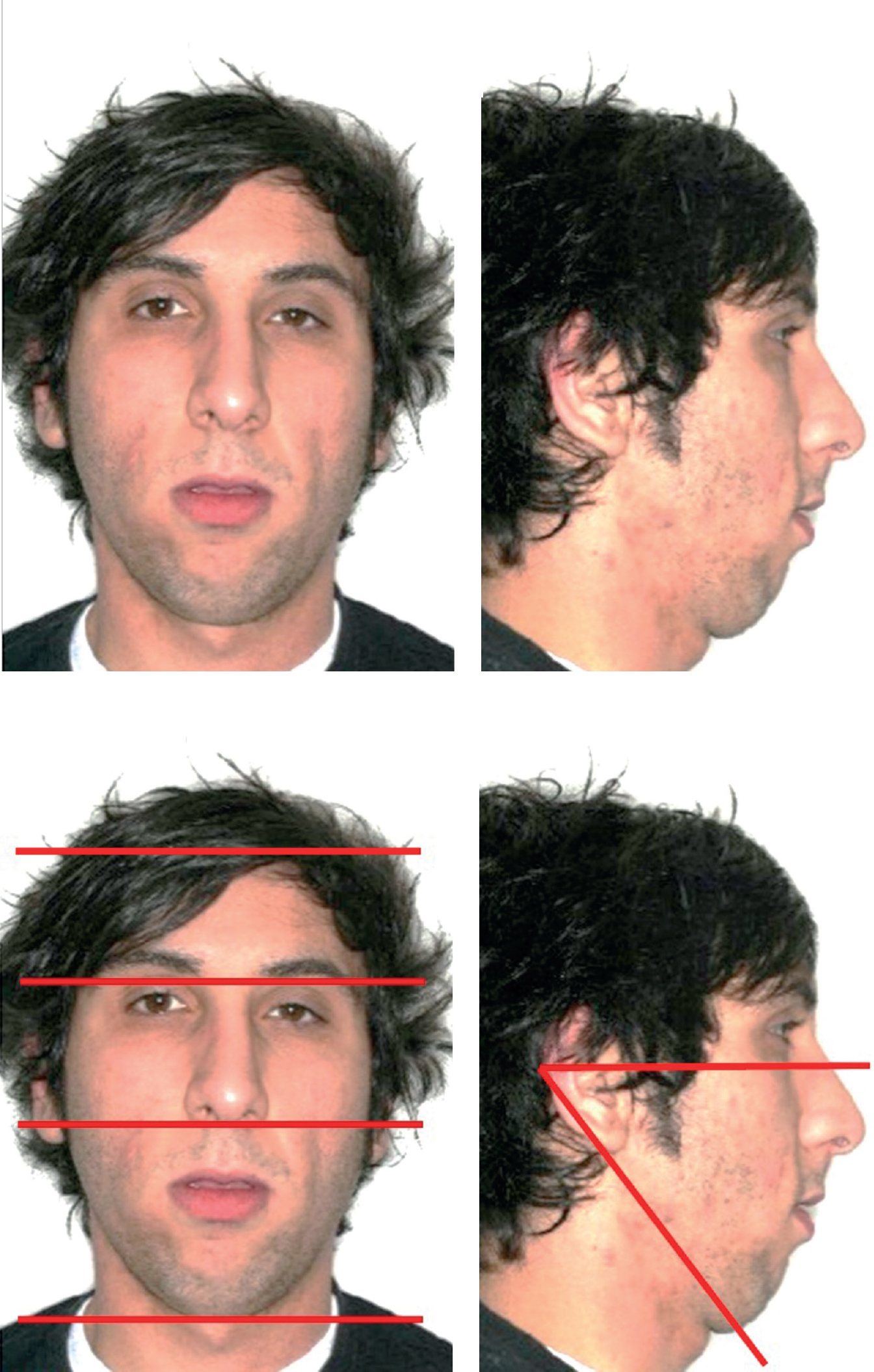
The skeletal vertical relationship can be assessed by two methods during the clinical extra-oral examination. The ALFH is a linear measure and is a proportion of the total anterior face height (TAFH). Clinically, an ALFH >50% of the TAFH is considered increased (Figure 1). This is measured by assessing the facial thirds and comparing the ALFH (columella to soft tissue menton) to the middle face height (glabella to columella). In profile, the FMPA is an angular measure and a patient's FMPA is classified as high (hyperdivergent) if the planes intersect anterior to the occiput. Further detail regarding clinical assessment of the vertical dimension is described in Part 1 of this series.
Figure 1. (a–d) Patient with high Frankfort mandibular planes angle and anterior lower face height (61% of total anterior face height). The Frankfort and mandibular planes intersect anterior to the occiput.4
Cephalometric examination
Cephalometrically, the MMPA can be described as high if it is above the norm of 27° and is dictated by the ratio of the ALFH and posterior lower face heights (PLFH). The relationship between the PLFH and ALFH is also termed the Jarabak ratio, and is determined by dividing the posterior by the anterior face height and multiplying by 100. An increased vertical growth pattern is indicated by a score of less than 62%. Another angle, formed between the mandibular plane and the line Sella-Nasion can also be used as an assessment tool, with the average angle being 35°.1
Aetiology
Skeletal
The main aetiological factor for patients with a high angle is skeletal disharmony.
Implant studies performed by Bjork et al5 demonstrated that growth of the mandible may include a rotational component, with a backward (clockwise) growth rotation most likely in individuals with an increased ALFH and FMPA/MMPA.
The structural indicators for growth rotations identified by Bjork6 are described in Part 1 of this series.
Pathology
Some types of condylar pathology, such as condylar aplasia, idiopathic condylar resorption, condylar fracture, condylar hypoplasia and juvenile rheumatoid arthritis, can lead to a reduction in ramus height and a backwards rotation with an increased ALFH and FMPA/MMPA.
Airway
The effect of chronic nasal obstruction or mouth breathing on vertical craniofacial development is a controversial subject.7,8 It is thought that mouth breathing, or partial nasal obstruction, can lead to postural head changes that affect growth as well as an increase in anterior facial height, overeruption of posterior teeth and downwards and backwards rotation of the mandible.9
Muscle activity
Some neuromuscular conditions, such as cerebral palsy and muscular dystrophy, can lead to increased lower facial height due to weak facial muscles and decreased tonic muscle activity. It is thought that decreased masticatory muscle activity may lead to a high angle, although failure to gain jaw elevator strength may be the consequence rather than the cause of the high angle and long face morphology.
Features commonly associated with high angle cases
Intra-orally, high angle patients can present with a range of features. High angle patients can present with reduced overbite or open bite (Figure 2), although in one study only 13% of patients with excessive vertical dimensions had anterior open bites.1 There is likely to be a degree of dento-alveolar compensation present in the vertical dimension as the teeth and periodontium try to mitigate for the vertical skeletal pattern. Typically, the anterior teeth have reached their maximum eruptive potential. The upper incisors may be proclined due to loss of lower lip control. If the vertical skeletal discrepancy is severe, lip incompetence may cause the patient to adopt altered soft tissue behaviour to achieve an anterior oral seal during swallowing, such as a tongue to upper or lower lip swallow. These patterns result in a decreased overbite. However, atypical presentation is possible. For example, a normal or deep overbite may present in a high angle patient, and, in these circumstances, treatment mechanics aimed at managing the intra-oral features may be unfavourable for managing the skeletal features.
Figure 2. (a–c) Patient presenting with a significant anterior open bite.
It is common to observe other skeletal, soft tissue and dental features in patients presenting with a low angle (Table 1).
Table 1. Features that may be observed in high angle cases.
Factor
Features
Skeletal
Increased Frankfort and maxillary mandibular planes angles Increased anterior lower face height Long faces
Soft tissue
Incompetent lips Shallow labio-mental fold Forward resting tongue position or macroglossia Chronic nasal obstruction/mouth breathing
Dental
Reduced overbite or anterior open bite Reduced or reversed curve of Spee in the lower arch. Increased curve of Spee in the upper arch Incisors at maximum eruptive potential
Management options
Management options for patients with a high angle include:
No treatment/accepting the malocclusion
Growth modification
Orthodontic correction or camouflage
Orthognathic correction.
Orthodontic mechanics that can be employed to manage a high FMPA/ MMPA include:
Intrusion of the buccal segment teeth
Extrusion of the labial segment teeth.
Growth modification
High-pull headgear, chin cup therapy or functional appliances can be used to attempt growth pattern modification.
High-pull headgear
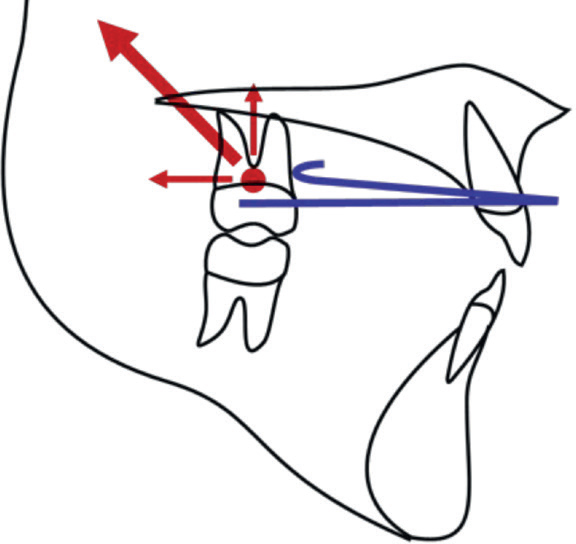
In high angle patients with good compliance, headgear can be used to deliver an extra-oral force to the upper teeth in order to intrude them and thereby reduce the lower anterior face height. This may be done using high-pull headgear (Figure 3), with bands placed on the upper first or second molars, or alternatively to an acrylic maxillary intrusion splint covering the occlusal surfaces of all the maxillary teeth, in order to try to intrude them. For headgear applied to the first molars, the force should be applied through the centre of rotation of the molar at the trifurcation of the roots, to avoid any mesial or distal tipping, which could exacerbate the vertical problem.
Figure 3. Resultant force (depicted by large red arrow) when high-pull (occipital) headgear is to be used to intrude the maxillary molars.
Low-pull (cervical) headgear should be avoided in high angle cases, as this will deliver an extrusive force to the molars and make managing the case more difficult.
Chin-cup
Chin-cup therapy can be used to limit vertical jaw growth, although evidence to support this approach is lacking, with a wide range of dentoalveolar and skeletal changes reported. There is no reliable protocol for its use and patient compliance is problematic.
Functional appliances
In a high angle patient with a Class 2 skeletal discrepancy and an anterior open bite, a modified twin block can be used during the pubertal growth period. High-pull headgear can be used in conjunction with functional appliances to attempt to restrain both horizontal and vertical maxillary growth. Alternatively, activator-type functional appliances can be used with bite blocks of at least 5–6 mm beyond the freeway space, with the anterior segment of acrylic removed.10 Frankel IV functional regulator appliances are also an alternative.
Orthodontic correction
Extraction choices
Extraction-based treatment and space closure in crowded arches, or simply space closure in a spaced arch, will help manage a high angle in two ways. The more anterior the extraction, the greater the anchorage balance shift towards lower labial segment retraction. The more posterior the extraction, the greater the tendency for mesial movement of posterior teeth and reduction of the ‘wedge’ effect. Space closure resulting from protraction of the buccal segments causes mandibular autorotation as the teeth move further from the terminal hinge axis.
Bracket placement
Conventionally, ideal bracket positioning for the straight-wire appliance is the facial axis point, which coincides with the centre of the crown both vertically and mesio-distally. However, placement of the incisor brackets more gingivally and the posterior brackets more occlusally can help correct mild vertical discrepancies.
Kim mechanics
In 1987, Kim described a method for correcting the generalized mesial inclination of the dentition in anterior open bite patients.11 These mechanics, now termed ‘Kim mechanics’, act to upright the buccal segments and encourage the occlusal plane of each arch to converge. Kim's therapy involved placing multi-loop edgewise archwires with counter-intuitive curves of Spee (increased in the upper and reversed in the lower), which acted to tip the molars and premolars distally. This was often complemented with extraction of the third permanent molars, to provide space for the necessary second molar movement. To avoid the otherwise inevitable bite opening anteriorly, he advised using anterior vertical elastics.
Posterior bite blocks
Occlusal coverage of the buccal segment teeth can affect the vertical relationship by two mechanisms. First, occlusal contact of the blocks may produce an intrusive force on the posterior teeth, and second, the lack of coverage of the anterior teeth may encourage their eruption. Bite blocks with full posterior acrylic coverage can be used either alone (Figure 4), or by incorporating repelling magnets or a spring-loaded mechanism. The devices typically have an upper and a lower component, which fit on to the posterior occlusal surfaces of the respective arches and deliver an intrusive force by means of the energy stored within the muscles of mastication and/or the spring or magnet. The use of repelling magnets is novel and used to achieve posterior intrusion,12 although there is limited knowledge about the long-term effects of magnetic forces on biological tissues and magnets are prone to oxidation in the oral environment. Aligner therapy has been reported to use the posterior bite block effect, where upper and lower aligner material over the contacting posterior teeth allow some improvement through relative molar intrusion.13
Figure 4. Posterior bite blocks incorporated into upper and lower removable appliances, with repelling magnets incorporated into the bite blocks.
Temporary anchorage devices
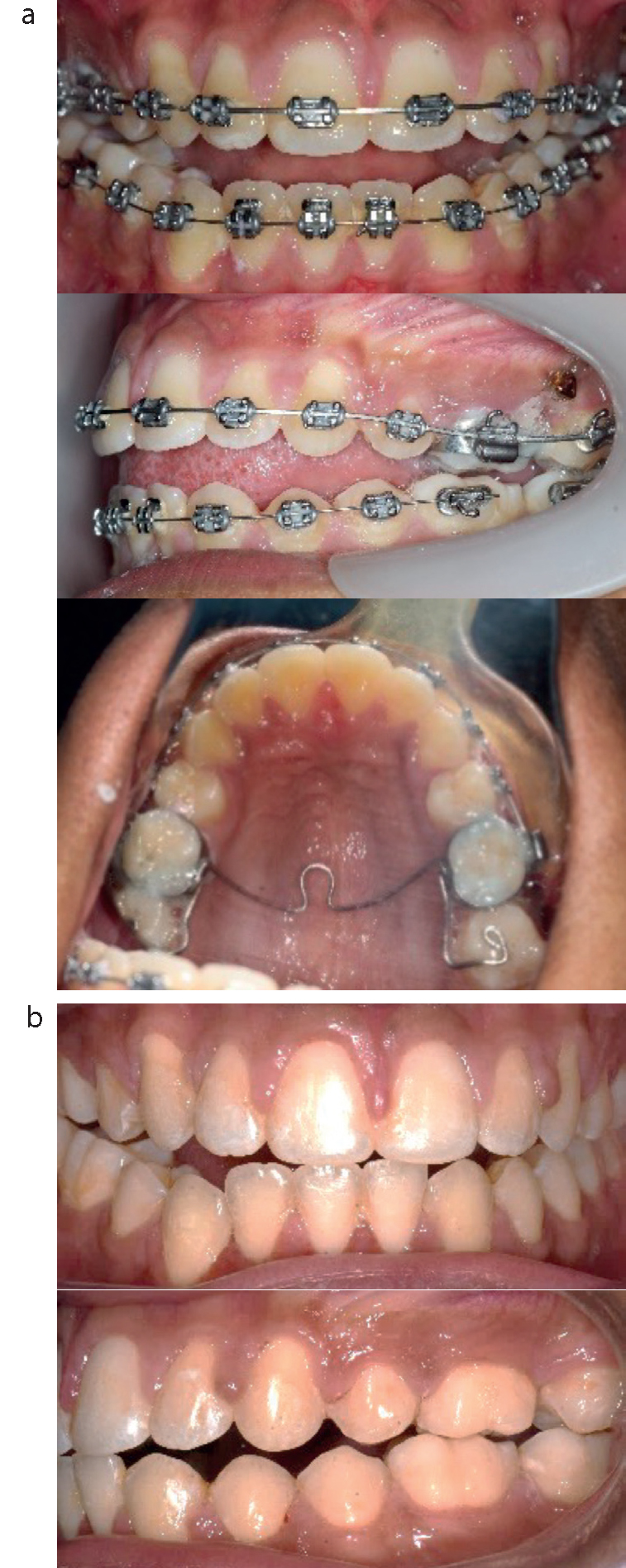
Temporary anchorage devices (TADs) can provide a means of skeletal anchorage for intrusion of the buccal segment teeth (Figure 5). In this case, they are placed into buccal cortical bone mesial and/or distal to the maxillary first molar, at the level of the mucogingival junction in the attached gingivae. A buccal-only force from the mini-screw results in buccal tipping of the molar, which will exacerbate the vertical problem. To avoid this, a palatal force component is necessary. This can be in the form of a TAD positioned in the palatal gingivae or in the palatal midline, or by placement of a transpalatal arch between the first molars, to resist the tipping. If a transpalatal arch is being used, this should be raised 3 mm away from the palate to avoid palatal trauma during intrusion. The intrusive force can be applied by means of elastomeric chain from the TAD to the molar band.
Figure 5. (a) Mid-treatment. (b) Post-treatment. Anterior open bite correction using buccally positioned temporary anchorage devices and modified transpalatal arch with occlusal stops extending onto the occlusal surfaces of the upper second molars. Intrusive force is provided by elastic powerchain from the temporary anchorage devices to the transpalatal arch.
Anterior elastics
Extrusive force can be applied to the labial segment teeth with the use of inter-maxillary elastics. Several configurations have been proposed. The anterior box elastic (Figure 6) can be placed from hooks in the upper and lower lateral incisor/ canine regions, bilaterally. Alternatively, vertical elastics, without the horizontal component, can be placed directly from hook to hook. These formations will provide an extrusive force to the upper and lower incisors to encourage further eruption of the teeth. However, it should be noted that in high angle cases, dento-alveolar compensation often results in the incisors being at the limit of their eruptive potential. Any additional extrusion is therefore likely to be unstable and is a common cause of relapsed anterior open bite. Intermaxillary elastics that involve the posterior dentition should generally be avoided because equal extrusion of anterior and posterior teeth will tend toward bite-opening, as the posterior teeth are closer to the terminal hinge axis.
Figure 6. Anterior box elastics.
Surgical correction
Surgical treatment in the high angle patient is generally reserved for those with a significant vertical discrepancy and those who are unhappy with their facial, as well as dental, aesthetics. Surgery should only be carried out once growth has ceased, to minimize relapse caused by continued growth. The general principle of this treatment approach is to reposition the maxilla in a superior position and allow the mandible to autorotate to reduce the FMPA and ALFH.
Le Fort I osteotomy with posterior impaction of the maxilla
This is the most frequent surgical approach for management of a high angle case. Bone is removed in a tapered manner so that more bone is removed posteriorly than anteriorly. The terminal tooth contacts are then reduced which allows for autorotation of the mandible. As the entire maxillary complex is rotated, the upper incisors will retrocline relative to the lower incisors. Presurgical orthodontics may involve a degree of proclination of the maxillary incisors to compensate for this typically unwanted effect.
Le Fort I osteotomy with posterior segmental impaction of the maxilla
This procedure is undertaken less frequently, but can be particularly helpful if no movement of the upper incisors is desired. In this case the maxillary incisor position remains unaltered while a segmental impaction of only the posterior segments is carried out.
Bilateral sagittal split osteotomy
A mandibular advancement or set back may be combined with a Le Fort I posterior impaction if there is an underlying horizontal skeletal discrepancy, either prior to treatment or, more likely, as a result of the surgery to the maxilla. However, if a bilateral sagittal split osteotomy is used solely to correct an anterior open bite, there is a risk the pterygo-masseteric sling will be put under tension and lead to relapse of the open bite post-surgery.14
Retention and stability considerations
Correction of high angle malocclusions are prone to relapse if there is continued growth with posterior rotation. There is limited scientific evidence allowing conclusions to be drawn regarding the stability of open bite.15 Extrusion of anterior teeth is likely to be unstable if the teeth have already reached their maximum eruptive potential. Other studies have reported that anterior open bite correction is prone to relapse, with 80% of patients recorded as having positive overbite at their latest follow-up, irrespective of whether they were treated with orthodontics alone or a underwent a combined orthodontic-surgical approach.16
If a reduced overbite is treated while the patient is still growing, the use of a posterior bite plane as part of the retention phase may be considered until facial growth has ceased, although there is a lack of evidence to support this.17
Surgical correction of high angle Class 2 skeletal patterns is generally undertaken with caution. Significant relapse has been reported in female patients with high FMPA, who had undergone large mandibular advancements.18,19 A study by Mobarak et al reported that high angle Class 2 patients who had been treated with a combined orthodontic/orthognathic approach showed increased frequency and greater magnitude of horizontal relapse.20
Conclusions
Diagnosis and treatment of the high angle patient can present difficulties for the orthodontist. This article highlights possible management options to control and correct vertical changes during treatment, although a holistic approach to managing these cases is recommended.