
Separators: a review of uses and limitations
From Volume 11, Issue 2, April 2018 | Pages 61-66
Article

Orthodontic separators are routinely used to create space between teeth, usually molars and/or premolars, prior to the placement of orthodontic bands. Separators are also used to create space to facilitate interdental reduction. Orthodontic auxiliaries can also be used for a variety of other purposes, which will be described. Additional indications are:
Separators are simple orthodontic auxiliaries, which are cheap and easily available. They have many benefits, however, there are also risks associated with the use of separators, most commonly discomfort but also localized periodontal disease if the separator is retained subgingivally.
Materials and types of separators
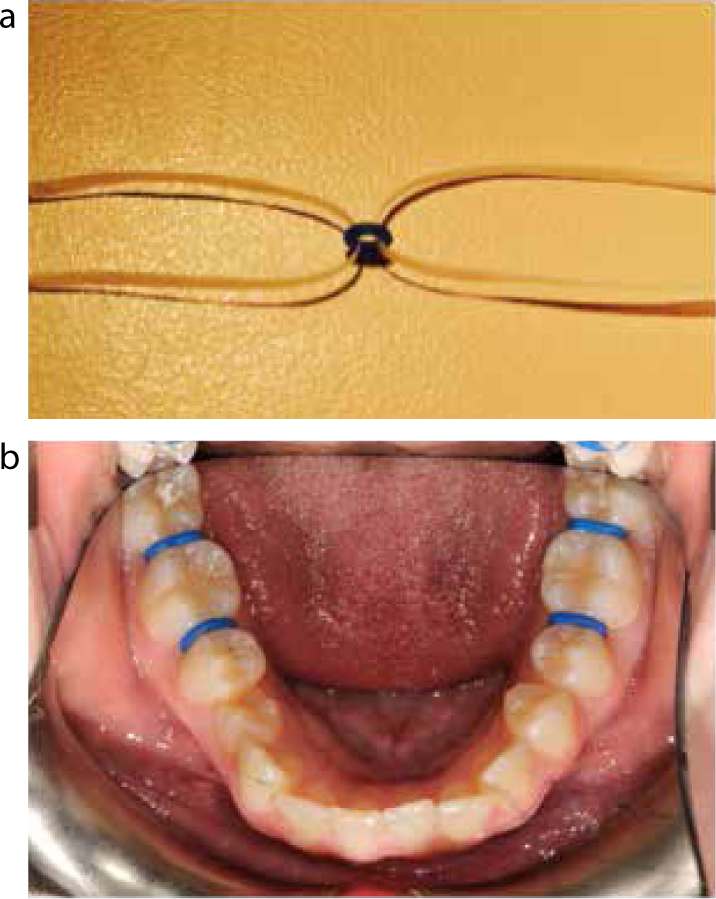
Various techniques have been described in Orthodontics to create space between teeth (Figure 1). These include elastomeric separators, brass wire, elastomeric thread,1 latex elastics, and a variety of spring separators.

Prior to steel or elastomeric separators, a brass wire was placed tightly against the contact point for about one week (Figure 2). This was uncomfortable and could be traumatic to the gingivae.2 Brass wire has been superseded by elastomeric materials and, less commonly, steel springs, which can also cause a level of discomfort. Elastomeric modules are very popular as they are easy to use, are low cost but are extremely effective. Although separators are usually prefabricated, steel springs may be constructed at the chairside.3 Steel separators are available in a number of preformed designs and shapes where different types have been described, such as Kesling and NEET springs. They are placed by manipulating one leg of the spring into the embrasure, after which pressure on the spring allows the second spring to be placed under the contact point. Although elastomeric separators have been shown to provide greater separation than spring separators (0.3 mm compared to 0.4 mm after 5 days),4,5 both auxiliaries provide an adequate amount of separation for the placement of orthodontic bands. Elastomeric separators can be more difficult to insert than other materials. However, they are less likely to be lost, have a short span of force application and may be left in situ for a greater period of time, although ideally not exceeding two weeks.5,6,7 Elastomeric separators are more cost-effective than other forms of separator, can vary in width (Figure 3), and are usually fabricated in bright or bold colours so that they may be easily identified and removed. However, clear separators are also available for anterior teeth if needed. Elastomeric separators are commonly circular, although other shapes, such as Dumbbell separators, are also available. Elastomeric separators are placed by stretching and slipping through the contact point, either by using two pieces of floss threaded through the centre, two mosquito clips or using separating pliers (Figure 4).


Indications
The primary use of separators is to facilitate the placement of orthodontic bands, which are most commonly placed between the molar teeth (Figure 5). The ideal separator should be easy to insert, cause minimal discomfort, separate the teeth adequately, should not be lost while chewing food and should remain between teeth until removed by the orthodontist. Once an adequate amount of space is created, these elastics may be lost during eating and brushing, which may allow the teeth to rebound to their original position.5

The degree and speed of separation varies with the material. Elastomeric separators are often placed for several days and have been shown to provide 0.11 mm of separation 24 hours after placement, which is adequate for the placement of bands. This space increases with time, with 0.28 mm created after 72 hours. Space creation is similar for both the more common circular shape and dumbbell shape of elastomeric separators. However, steel separators of the Kesling or NEET design require more time to allow sufficient separation, with 0.06 mm formed after one day and 0.15 mm after two days.5
The development of enamel bonding technology has provided an alternative to the use of bands and therefore the need for separators. The additional appointment for separator insertion is avoided, allowing the placement of fixed appliances to be more convenient and efficient. Many operators, however, continue to utilize bands as the terminal attachment of fixed appliances, as loss of bonded attachments can delay completion of treatment. Molar bands have been shown to have a reduced failure rate compared to molar tubes.6 Molar tubes are thought to enable the patient to maintain oral hygiene more easily than bands, although Nazir et al found bonded molars experienced greater demineralization.6 Bands are also necessary for the construction of palatal and lingual arches and fixed expansion arches, such as Quadhelix or Rapid Maxillary Expansion appliances.
Interproximal reduction of the teeth may be used to create space for the alignment of teeth8,9 and to reduce the dark triangles that may appear after the alignment of the anterior teeth.10 The placement of separators prior to reduction has been advocated to improve mechanical and visual access to the contact area. Elastomeric separators may be more beneficial than steel springs as they can depress the papilla, reducing the likelihood of gingival trauma.8 Clear elastomeric modules are available to be used in the labial segment, in comparison to the darker colours more often utilized posteriorly.
1. Management of ectopic teeth
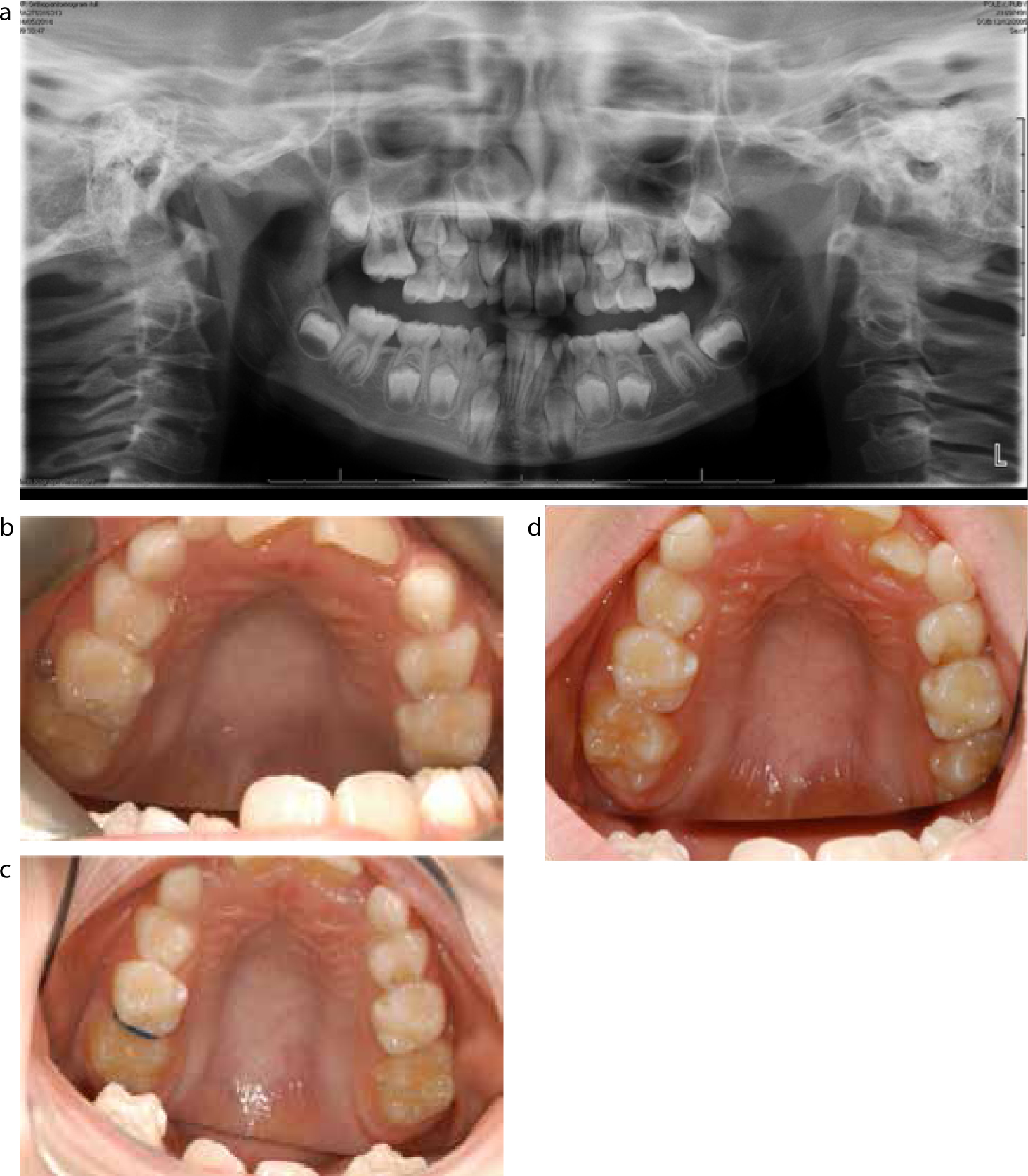
Separators have been used to upright ectopic teeth (Figure 6). Seehra et al used a combination of disking the distal aspect of upper second premolars and placement of separators to disimpact maxillary first permanent molars.11 Whilst one tooth responded favourably, the other did not and required extraction of the second permanent premolar to allow eruption. Rajesh et al improved access by exposing the second molar completely, using laser excision of the overlying mucosa under local anaesthetic prior to placing the separator.12 Placement of separators to upright a first molar is simple, cheap and, if effective, avoids extraction of a primary molar in a young child.
2. Construction of attachments on teeth
Elastomeric separators can be used to construct custom attachments. The elastomeric module can be filled with composite resin, placed on the previously etched tooth and cured. This is used as a template to construct attachments that can be bonded to teeth to allow traction to be applied, to achieve many tooth movements. These attachments can be used as point of force application to align or de-rotate a tooth via elastics or a power chain applied to the undercut created. The design has the advantage of being tooth-coloured, cheap, easy to replace and remove (Figure 7).

3. Pre-restorative/prosthodontic tooth movement
Separators may be used prior to restorative and prosthodontic treatment where they can regain interproximal space lost due to carious tooth loss and subsequent drifting of teeth.13,14 Recreating space can facilitate a more functional restoration and can aid in the creation of tight interproximal contact points. Separators have also been used to enable pre-restorative alignment of teeth15 and also allow pre-prosthetic optimization of an emergence profile in aesthetic crowns.16
Regaining lost space due to caries involvement
Menegh et al described the use of elastic orthodontic separators in conjunction with an incrementally modified acrylic crown to regain space, allowing the placement of a physiologically contoured restoration.14 Sufficient space for the prosthesis was achieved following two replacements of separator placement and temporary crown modification. The authors have advocated this method as an alternative to fixed orthodontic appliance therapy for the recovery of a small amount of space, however, the options to move teeth are limited.
Pre-restorative/prosthetic re-alignment of teeth
Elastic separators can be used to tip the desired tooth into its original position before a restorative procedure.15 This allows restoration of a normal crown contour and improves the tooth's long-axis alignment. Freitas-Júnior and Silva used a separator to help in prosthetic techniques to restore aesthetics and function in a patient successfully with a distally drifted maxillary lateral incisor.16
Improving interproximal contacts in posterior composite Class II restorations
The consistency of resin composites makes the condensation against the contact areas of adjacent teeth difficult in comparison to amalgam.17 A number of techniques have been advocated to overcome this problem, including pre-wedging, placing pressure on the contact area and anatomically shaped wedges.17,18 Placing an orthodontic separator adjacent to the surface to be restored prior to the restoration will cause slight separation and, once the space recovers, a tight contact point is created.19 However, an additional appointment for placement of the separator is needed.
Hall technique
Elastic separators can be very useful when fitting crowns with the Hall technique, a method of managing carious primary molars in children.20 This can be done over two visits; by placing the separators through the mesial and distal contacts (Figure 4), especially through tight contact points or if there has been loss of mesio-distal tooth width due to loss of marginal ridge(s), and then removing them 3−5 days later.
4. Allow direct vision to assess cavitated carious lesions
Caries is a common disease. Encouraging remineralization through regular disruption of plaque biofilm and fluoride application can arrest lesions. Accessing approximal surfaces for an accurate diagnosis of caries, however, can be difficult.21 Separators have been used to help detect the presence of caries interdentally as it can aid direct vision of the carious lesion and help the decision as to whether it is cavitated. This approach has been advocated as an alternative or adjunct to radiographic examination22 and may be used as a reference or gold standard by which other techniques of caries detection are compared.23,24
5. Replacing a module to cushion the bite if bracket interference is present
An elastomeric separator can be used on lower premolar or incisor teeth, replacing the usual elastomeric module used to secure the archwire in the bracket slot if the bracket is in occlusal contact with the opposing tooth. The thicker design can provide a cushioning effect and could avoid the need for a biteplate or occlusal build-up to disengage the bite.
6. Extraction of erupted teeth
The placement of orthodontic separators for two weeks prior to extraction has been described to reduce the risk of fracture of the root, tip, crown and cortical plates.25 The author found the increased mobility of the tooth led to fewer complications in the removal of teeth with long roots, unusual root morphology (eg spindly roots) and dense bone.
Limitations/Risks
1. Pain and discomfort
The placement of separators can cause pain and discomfort and some patients report that this is the most painful part of the entire treatment. Simple analgesics are recommended. Most patients report pain during eating and chewing.26 The pain is worst on the second day after placement following which it steadily decreases.3 Although all types of separators may cause pain, the initial discomfort has been described as higher with brass wire in comparison to elastomeric separators.27
The use of analgesia to reduce the discomfort of separator placement has been widely reported. Two studies by Bernhardt et al28 and Law et al29 fulfilled the requirements of a Cochrane review30of pre-operative analgesia for additional pain relief in children and adolescents having dental treatment. Both of these papers looked at whether Ibuprofen reduced pain and discomfort following the placement of orthodontic separators. Bernhardt advised Ibuprofen both pre- and post-operatively, whilst Law only pre-operatively. Although both studies had a high risk of bias, they both found a reduction in the amount of pain which was statistically significant when a meta-analysis was carried out. Ibuprofen has been shown to have a superior analgesic effect compared to paracetamol.31
A number of other methods to reduce discomfort have been advocated, such as low level laser therapy (LLLT),32 Benzocaine 20% patches33 and transcutaneous electrical nerve stimulation (TENS).34 However, the use of analgesia and a soft diet are the most commonly used to reduce discomfort.
2. Localized periodontal disease
There have been numerous reports of damage to the periodontal tissues due to the retention of orthodontic separators. For instance, the placement of separators for 2 weeks to increase tooth mobility, to aid extractions, also demonstrates the periodontal effect. The separator can slide down the tooth due to the lack of stabilization and penetrate the gingival sulcus35 (Figure 8). The patient may present with a variety of clinical signs and symptoms, such as pain, discomfort, swelling, tooth mobility, gingival recession, extrusion and increased probing depths.35,36,37 Radiographic findings include periodontal bone loss, widening of the periodontal ligament, bone loss and intrabony defects. The ectopic separator may present as a slight radiolucency or radio-opacity or may not be visible at all.35

The cause of the symptoms is often misdiagnosed initially and may lead to a variety of failed treatment, such as subgingival debridement,38 flap surgery, splinting or extraction of the tooth.39 Diagnosis is complicated by variability in the radio-opacity of separators and the timeframe in which the symptoms may present. A swelling may form within days of placement, whilst others remain undetected and symptomless for a number of years after the completion of fixed orthodontic treatment.36 Removal of the orthodontic separator resolves the signs and symptoms, however, significant localized periodontal disease may lead to attachment loss and recession or may necessitate the extraction of the tooth.35,36
A number of methods to prevent and minimize the risks of separator retention have been suggested, such as reducing the time period for which they are placed, using radio-opaque separators and brightly coloured material to aid their visibility and removal.35 It is important to record on the record card the number and position of separators placed and record that they are removed. If the separator appears to have fallen out, the inter-proximal area of the gingiva should be inspected thoroughly to check that the separator has not worked its way below the contact point. When separators are placed, patients and parents must be made aware that retention is a possible complication and how important it is to note and report to the clinician if they fall out.
Conclusion
Orthodontic separators are primarily designed for use to create space prior to the placement of orthodontic bands. They can, however, be used for a variety of clinical situations by Orthodontists and General Dental Practitioners. They are versatile, easy to use and relatively cheap, making them a useful adjunct in the dental armamentarium. It is extremely important to appreciate that their use is not without risk, as inadequate monitoring following placement can lead to retained separators and serious damage to dental health.