Steel J, O'Sullivan I.: The Information Centre for Health and Social Care; 2011
: BSP; 2016
Lang NP, Adler R, Joss A, Nyman S. Absence of bleeding on probing. An indicator of periodontal stability. J Clin Periodontol. 1990; 10:714-721
Silness J, Löe H. Periodontal disease in pregnancy. Part II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964; 22:121-135
Hodge P. Mouthwashes: Do they work and should we use them? Part 3: Safety of mouthwashes. Dent Update. 2016; 43:728-733
Cairo F, Cortellini P, Tonetti M, Nieri M, Mervelt J, Cincinelli S, Pini-Prato G. Coronally advanced flap with and without connective tissue graft for the treatment of single maxillaryo gingival recession with loss of inter-dental attachment. A randomized controlled clinical trial. J Clin Periodontal. 2012; 39:760-768
Cortellini P, Tonetti MS. Improved wound stability with a modified minimally invasive surgical technique in the regenerative treatment of isolated interdental intrabony defects. J Clin Periodontol. 2009; 36:157-163
Pini-Prato G, Franceschi D, Rotundo R, Cairo F, Cortellini P, Nieri M. Long-term 8-year outcomes of coronally advanced flap for root coverage. J Periodontol. 2012; 83:590-594
Matuliene G, Pjetursson BE, Salvi GE Influence of residual pockets on progression of periodontitis and tooth loss: results after 11 years of maintenance. J Clin Periodontol. 2008; 35:685-695
Gkantidis N, Christou P, Topouzelis N. The orthodontic-periodontal interrelationship in intergrated treatment challenges: a systematic review. J Oral Rehabil. 2010; 37:377-390
Hamp S-E, Nyman S, Lindhe J. Periodontal treatment of multirooted teeth. Results after 5 years. J Clin Periodontol. 1975; 2:126-135
Abbott PV, Castro Salgado J. Strategies for the endodontic management of concurrent endodontic and periodontal diseases. Aust Dent J. 2009; 54:S70-S85
McGuire MK, Nunn ME. Prognosis versus actual outcome. III The effectiveness of clinical parameters in accurately predicting tooth survival. J Periodontol. 1996; 67:666-674
Miller PDPhiladelphia: Blakiston Company; 1938
Miller PD A classification of marginal tissue recession. Int J Periodont Rest Dent. 1985; 5:8-13
Roccuzzo M, Bunino M, Needleman I, Sanz M Periodontal plastic surgery for treatment of localized gingival recessions: a systematic review. J Clin Periodontol. 2002; 29:178-194
Joss-Vassalli I, Grebenstein C, Topouzelis N, Sculean A, Katsaros C. Orthodontic therapy and gingival recession: a systematic review. Orthod Craniofac Res. 2010; 13:127-141
Heasman PA, Hughes FJ. Drugs, medications and periodontal disease. Br Dent J. 2014; 217:411-419
Lang NP, Berglundh T, Mombelli A. Peri-implant diseases: where are we now? Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011; 38:178-181
Lindhe J, Meyle J. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:282-285
In: Horner K, Eaton KA (eds). : Faculty of General Dental Practice (UK); 2013
Adult patients are increasingly interested in having orthodontic treatment but many of these patients have periodontal problems. A periodontal examination should involve a basic periodontal examination (BPE) as well as the identification of any mobility, recession and gingival overgrowth. Each BPE code indicates different investigations and treatment. The cause of any mobility, recession and gingival overgrowth needs to be identified and then treated appropriately. Periodontal treatment may involve input from the patient's general dental practitioner or, if more complex treatment is required, referral to a specialist. Any periodontal problems identified should be addressed prior to orthodontic treatment.
CPD/Clinical Relevance: This article details how to carry out a periodontal examination and considers the implications of the findings on the provision of adult orthodontic treatment.
Article
Anna C Greer
Periodontitis is ‘a chronic inflammatory disease of bacterial aetiology that affects the supporting tissues around the teeth’.1 The Adult Dental Health Survey 2009 classified 17% of dentate adults as having very good periodontal health,2 but this indicates that a large percentage of the UK population experiences some level of periodontal disease. Amongst other things, periodontal disease can result in recession, drifting, mobility, compromised aesthetics and tooth loss. Because of these changes, patients with current or previous periodontal disease may request orthodontic treatment. As part of an orthodontic assessment it is important to assess patients' periodontal status as it may impact on their orthodontic treatment. The aim of this paper is to describe how a periodontal examination should be carried out in adults and the implications of the results of the examination.
Basic periodontal examination (BPE)
The basic periodontal examination (BPE) is the screening tool for assessing periodontal health. It should be performed on all dentate adult patients as part of the initial examination. To carry out a BPE, the mouth is divided into sextants and, for each sextant, the highest score is recorded. Third molars are only included in the assessment if at least one of the first and second molars is missing. A score is only recorded if a sextant has more than one tooth present. The BPE should not be used around dental implants.1,3
To carry out the BPE, a ball-ended World Health Organization (WHO) probe should be used (Figure 1). The probe should be walked around each tooth with a force of 20–25 grams. This is equivalent to the pressure required to make a fingernail bed blanch. Pressure sensitive probes are available (Figure 2). The codes used in the BPE are shown in Table 1.1,3
Figure 1. WHO probe.Figure 2. Pressure sensitive Florida probe.
BPE Score
Criteria
0
No bleeding on probing (BOP), no pocket depths greater than 3.5 mm, no calculus/overhangs
1
BOP, no pocket depths greater than 3.5 mm, no calculus/overhangs
2
Plaque retentive factors present, eg calculus or overhangs, no pocket depths greater than 3.5 mm
3
Pocket depths between 3.5 mm and 5.5 mm
4
Pocket depths greater than 5.5 mm
*
Furcation involvement
For each sextant, a number should be allocated. In addition to a number, a star may also be allocated to a sextant, depending on the presence of furcation involvement. For example, an upper right first molar with a pocket depth of 7 mm and furcation involvement would mean that a score of 4* would be allocated to the upper right sextant.3
What do the codes indicate?
A code 0 indicates good periodontal health. The absence of bleeding on probing (BOP) has been shown to be a reliable indicator of periodontal health.4 Patients with code 0 in all sextants are therefore ready for orthodontic treatment, with no further periodontal instruction necessary.
A code 1 indicates inflammation is present and that the patient's oral hygiene is not sufficient to control the inflammatory process. A code 1 could indicate BOP at one site or multiple sites. Therefore, BOP and plaque indices should be used to assess the distribution of the sites involved. There are a number of different indices for assessing plaque and BOP. Commonly, the presence or absence is recorded at 4 or 6 sites per tooth. The number of positive sites is divided by the number of sites examined in order to express plaque/BOP as a percentage.5 BOP is not a reliable indicator in smokers due to the altered vasculature of the gingival tissues.6 In smokers, lack of BOP should not be interpreted as lack of inflammation.
Patients with any code 1 sextants should be given oral hygiene instruction and then reviewed one month later and immediately prior to commencing orthodontic treatment. Ideally, patients should have no sites with plaque or BOP prior to commencement of orthodontic treatment.
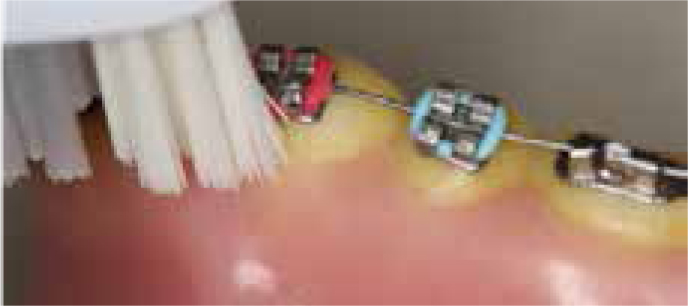
Oral hygiene instruction should include advice regarding the type of toothbrush and technique. Manual toothbrushes should be of medium stiffness and they should have a sufficiently small head to allow access. An electric toothbrush is also suitable, both before placement of the appliance and during appliance treatment. The patient should be shown how to hold the toothbrush directing the bristles at approximately 45 degrees to the gingival crevice (Figure 3).
Figure 3. Toothbrush technique.
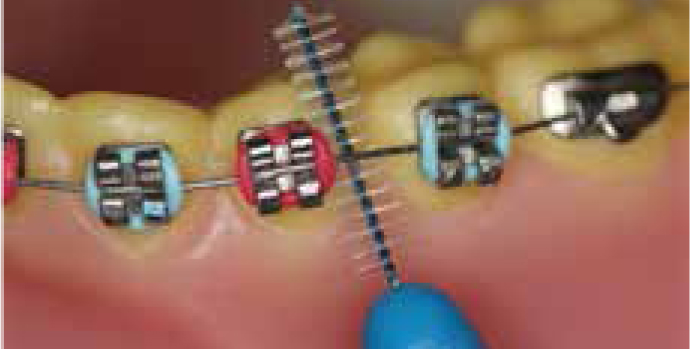
Additional cleaning measures should also be advised and demonstrated to the patient. Interdental cleaning measures are vital. Interproximal brushes, such as those with bristles and those made of soft rubber, are highly efficient when the correct size is used (Figures 4 and 5). Interproximal brushes should be as large as possible to clean between the teeth without crushing the soft tissues.
Mechanical cleaning is more effective than mouthwash for optimizing oral hygiene. Mouthwashes containing chlorhexidine gluconate are the only ones with the potential to prevent plaque formation, but these are not advisable for regular use due to staining and their side-effects.7
The authors are unaware of any definitive guidance on the percentage of sites with BOP that would indicate delaying orthodontic treatment. The literature relating to periodontal plastic surgery may, however, provide some guidance in this area. Similarly to orthodontic treatment, periodontal plastic surgery requires excellent levels of oral hygiene. Studies assessing these techniques restrict periodontal plastic surgery to patients who have ≤20% sites with BOP.8,9-10 Therefore, ≤20% sites with BOP might be considered an acceptable level prior to commencement of orthodontic treatment. This criterion still indicates BOP at 1 in every 5 sites and may be considered too high by some clinicians. The same criteria were also used for percentage of sites with plaque present. Therefore ≤20% sites with plaque might also be considered an acceptable level prior to commencement of orthodontic treatment. Anecdotally, many orthodontists in the UK suggest that a plaque score of less than 10% is required prior to commencing orthodontic treatment and we would support this lower threshold.
A code 2 means plaque retentive factors are present, such as calculus or overhanging restoration margins. These need to be removed to optimize oral hygiene and prevent periodontal disease progressing.3 Prior to orthodontic treatment starting, patients should be given oral hygiene instruction and any plaque retentive factors should be removed. Patients should be reviewed one month later and prior to commencement of orthodontic treatment. If they subsequently have BPE codes of 1 (ie presence of bleeding on probing) they should be managed as detailed above.
A code 3 and 4 requires greater input in terms of investigation and management. To ensure the correct diagnosis is made and a suitable treatment plan is devised, it may be beneficial to have input from a dentist experienced in periodontology. For patients with a code 3, full pocket charting should be recorded for that sextant. For patients with a code 4, full mouth pocket charting is indicated. All pocket charts should be accompanied by a record of sites with plaque and bleeding on probing. This link gives access to an interactive periodontal chart (www.periodontalchart-online.com).11
A number of parameters can be charted, including pocket depths, presence of plaque and presence of bleeding on probing.11 Radiographs should be taken of all sextants with a code 3 or 4. It is the clinician's decision as to which radiograph would be best but the crestal bone levels should be visible.1,3
For patients with a code 3 or 4, patient specific oral hygiene instruction and non-surgical periodontal treatment will be required. Non-surgical periodontal management includes removal of plaque retentive factors, as well as supra- and sub-gingival debridement. All pocket depths ≥4mm should be debrided under local anaesthetic. These patients should be re-assessed after 3 months. The BPE is not a monitoring tool; it does not include sufficient detail to measure disease resolution or progression. Therefore, patients with BPE codes 3 or 4 require periodontal pocket charts prior to and after non-surgical periodontal treatment.3
In patients not receiving orthodontic treatment, in the absence of BOP any pockets greater than or equal to 6 mm represent incomplete treatment and require further intervention.12 This may involve a further cycle of non-surgical periodontal treatment, the use of local or systemic antibiotics to supplement non-surgical periodontal treatment or periodontal surgery.1
For those wishing for orthodontic treatment, shallower pockets would be expected prior to commencement of appliance therapy. Although there is no definitive guidance, the authors would recommend that there should not be any pocket depths ≥4 mm prior to the commencement of orthodontic treatment. This is similar to the pocket depths expected prior to providing periodontal plastic surgery.8 The patient's periodontal health should be stable for 6 months prior to the initiation of orthodontic treatment.13 Orthodontic treatment should not be initiated in patients with active periodontal disease, ie patients with deep pocketing and/or bleeding on probing, as increased bone loss can occur.13
Teeth with furcation involvement – code * – require further investigation. Ideally, a Naber probe should be used for assessing furcation involvement (Figure 6). Table 2 shows Hamp's classification system for furcation involvement.14
Figure 6.
(a, b) Naber probe.
Grade
Indication
I
Less than 1/3rd the width of the tooth
II
Greater than 1/3rd but less than the width of the tooth
III
Through and through
Furcation involvement may indicate that a tooth has lost vitality. All teeth with furcation involvement should be assessed with a periapical radiograph taken using a paralleling technique. They should also be sensibility tested, for example with ethyl chloride or with an electric pulp tester.
If there has been loss of vitality, root canal treatment should be initiated or the tooth should be extracted.15 Teeth with furcation involvement have a poorer prognosis,16 therefore if teeth are to be extracted as part of the orthodontic treatment, any teeth with furcation involvement should at least be considered as candidates for extraction.
Aspects of periodontal assessment not included in the BPE
Tooth mobility is an important part of the periodontal assessment. It is regularly recorded using Miller's index (Table 3).17
Grade
Definition
I
0.2–1 mm horizontal movement
II
Between 1 and 2 mm horizontal movement
III
Vertical and/or >2 mm horizontal movement
If mobility is detected, its cause needs to be diagnosed. Causes of mobility include reduced bone support, trauma, dental abscesses and occlusal interferences. Periapical radiographs are required of any teeth exhibiting increased mobility. If mobility is due to reduced bone support, orthodontic treatment may be inadvisable as further periodontal bone loss and/or apical root resorption may further increase the mobility. Teeth that are mobile following trauma often have a poorer prognosis and should be assessed by a multidisciplinary team to develop an appropriate treatment plan.
Other aspects to consider during the periodontal examination are gingival recession and gingival biotype. Gingival recession is usually classified as per Miller's classification (Table 4).18 Teeth with Miller Class I and II defects usually respond well to treatment.19
Classification
Definition
I
Marginal tissue recession which does not extend to the mucogingival junction; no alveolar bone loss or soft tissue loss in the inter-dental area
II
Marginal tissue recession which extends to or beyond the mucogingival junction; no alveolar bone loss or soft tissue loss in the inter-dental area
III
Marginal tissue recession which extends to or beyond the mucogingival junction; alveolar bone loss or soft tissue loss in the inter-dental area
IV
Marginal tissue recession which extends to or beyond the mucogingival junction; alveolar bone loss or soft tissue loss in the inter-dental area with gross flattening and/or gross malposition of a tooth
In addition to periodontal disease, there are a number of other factors associated with gingival recession, including traumatic toothbrushing habits, oral piercings (Figure 7), previous orthodontic treatment and bruxism.20 The cause of the recession should be ascertained and the current tooth position should be evaluated in the context of its soft tissue and bony envelope. There is some evidence that patients with a thin gingival biotype are more likely to experience gingival recession.20 Patients with pre-existing gingival recession should be warned that their recession may worsen with orthodontic treatment.
Figure 7.
(a, b) Oral piercing and recession.
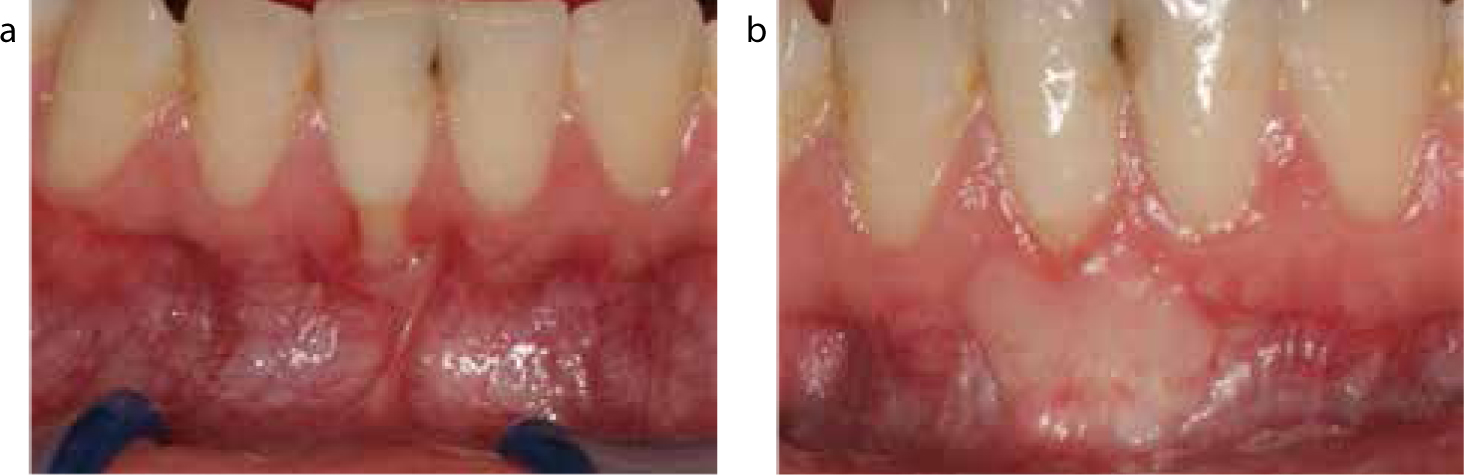
Many patients with localized labial gingival recession are concerned that the tooth will be lost. Most of these teeth have good interproximal and lingual/palatal bony support and the long-term prognosis is good if optimum oral hygiene is maintained. Treatment of recession defects may be indicated if there is sensitivity, aesthetic concerns or oral hygiene is impaired by the soft tissue morphology. A number of different surgical techniques are available, including the coronally advanced flap and sub-epithelial connective tissue graft (Figure 8). For treatment of recession, there is no clear evidence as to whether any root coverage procedures should be performed before or after orthodontic treatment.13 Input from a periodontal or a restorative specialist should be sought if root coverage procedures are being considered.
Figure 8. Connective tissue graft and frenectomy (a) before and (b) after treatment.
The presence of any gingival overgrowth should also be recorded. Gingival overgrowth may be due to plaque-related inflammation, repeated trauma or mouth breathing. It can also be drug-induced. Calcium channel blockers, cyclosporin and phenytoin are all known to cause gingival overgrowth (Figure 9). The treatment of drug-induced gingival overgrowth involves reinforcement of oral hygiene instruction, as well as generalized scaling. Root surface debridement of all periodontal pockets greater than or equal to 4 mm in depth should be carried out under local anaesthetic. In some cases, it is necessary to liaise with the general medical practitioner to see if the medication can be altered.1,21 It may be that a gingivectomy is required. Any overgrowth should have resolved prior to the commencement of orthodontic treatment.
Figure 9. Gingival overgrowth.
Adult orthodontic patients may also present with dental implants. The health of the peri-implant tissues should be assessed by recording pocket depth at six sites around the implant. The presence of BOP and suppuration should also be recorded. Gentle periodontal probing will not damage the implant surface or the peri-implant attachment. (As for a BPE, a force of 20–25 grams is advocated.) The presence of bleeding on probing and/or increasing probing depths suggests that inflammation may be present and requires further investigation by a clinician familiar with managing the peri-implant soft tissues.22,23 Radiographs of dental implants are not routinely required if the peri-implant tissues are stable.24
Conclusions
Adult patients with periodontal disease are increasingly presenting requesting orthodontic treatment. A periodontal examination should always involve a BPE, as well as the identification of any mobility, recession, gingival overgrowth and the extent of any furcation involvement. Rather than using the BPE, dental implants should have more detailed periodontal parameters recorded.
Any periodontal problems identified should be addressed prior to orthodontic treatment. This may involve treatment from the patient's general dental practitioner or, if more complex treatment is required, referral to a periodontal specialist or a restorative specialist.