Mehboob B, Khan M, Fahad Q. Pattern and management of palatine bone fractures. Pakistan Oral Dent J. 2014; 34
Narula K, Shetty S, Shenoy N, Srikant N. Evaluation of the degree of fusion of midpalatal suture at various stages of cervical vertebrae maturation. APOS Trends Orthod. 2019; 9:235-240
Cienfuegos R, Sierra E, Ortiz B, Fernández G. Treatment of palatal fractures by osteosynthesis with 2.0-mm locking plates as external fixator. Craniomaxillofac Trauma Reconstr. 2010; 3:223-230 https://doi.org/10.1055/s-0030-1268519
Gala Z, Halsey JN, Kapadia K Pediatric palate fractures: an assessment of patterns and management at a level 1 trauma center. Craniomaxillofac Trauma Reconstr. 2021; 14:23-28 https://doi.org/10.1177/1943387520935013
Angelieri F, Cevidanes LH, Franchi L Midpalatal suture maturation: classification method for individual assessment before rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2013; 144:759-769 https://doi.org/10.1016/j.ajodo.2013.04.022
Rimell F, Marentette LJ. Injuries of the hard palate and the horizontal buttress of the midface. Otolaryngol Head Neck Surg. 1993; 109:499-505 https://doi.org/10.1177/019459989310900319
Hoppe IC, Halsey JN, Ciminello FS A single-center review of palatal fractures: etiology, patterns, concomitant injuries, and management. Eplasty. 2017; 17
Cornelius Carl-Peter, Gellrich Nils, Hillerup Søren, Kusumoto Kenji, Schubert Warren Closed treatment for palatoalveolar fracture, complex injury. AO Surgery Reference. 2009;
Liu S, Xu T, Zou W. Effects of rapid maxillary expansion on the midpalatal suture: a systematic review. Eur J Orthod. 2015; 37:651-655 https://doi.org/10.1093/ejo/cju100
Angelieri F, Cevidanes LH, Franchi L Midpalatal suture maturation: classification method for individual assessment before rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2013; 144:759-769 https://doi.org/10.1016/j.ajodo.2013.04.022
Knaup B, Yildizhan F, Wehrbein H. Age-related changes in the midpalatal suture. A histomorphometric study. J Orofac Orthop. 2004; 65:467-474 https://doi.org/10.1007/s00056-004-0415-y
Korbmacher H, Schilling A, Püschel K Age-dependent three-dimensional microcomputed tomography analysis of the human midpalatal suture. J Orofac Orthop. 2007; 68:364-376 https://doi.org/10.1007/s00056-007-0729-7
Non-surgical management of a traumatic mid-palatal suture diastasis by novel use of an orthodontic appliance Fiona Jenkins Orthodontic Update 2025 16:1, 41-44.
Authors
FionaJenkins
BDS MDentSci FDS(Orth) MFDS M.Orth RCS(Eng)
Consultant in Orthodontics, St Luke's Hospital, Bradford Teaching Hospitals
Sutures are formed during embryonic development at the sites of approximation of the membranous bones of the craniofacial skeleton. They afford major sites of bone expansion during postnatal craniofacial growth, and also influence facial fracture patterns through offering a path of least resistance to force. There are some studies that have shown that the mid-palatal suture (MPS) fuses at 11–13 years and 14–16 years in females and males, respectively. This means that during childhood, the suture is open; thus force applied to the palate at this time tends to split the bone in the midline between the two unfused palatal shelves. The understanding of this biological process allows orthodontists to correct transverse growth discrepancies of the maxilla. Various appliances, including the hyrax appliance, can be used to allow rapid maxillary expansion (RME) by expanding the suture. Paradoxically, the same appliance can be used to allow rapid maxillary contraction (RMC) by contracting the suture. This method of application using a hyrax appliance is rare. We present a case report where this method of application allowed closure of a traumatic mid-palatal suture diastasis, correction of a traumatic transverse discrepancy of the maxilla and avoided an invasive surgical intervention in a 15-year-old male.
CPD/Clinical Relevance: This article highlights the importance of considering a patient's age and anatomical development when exploring treatment options. It is prudent to take advantage of this to enhance the natural biological healing process.
Article
Traumatic midface injuries can occasionally result in fractures of the hard palate. These fractures may occur as isolated injuries, but are more commonly associated with comminuted midfacial fractures.1 Even so, they are usually found in fewer than 10% of patients with mid-face fractures, although some isolated studies report a much higher incidence.2 Owing to their low incidence, they are often overlooked, causing post-operative malocclusion in trauma patients, resulting in potentially avoidable extensive surgical, orthodontic and/or restorative treatment to manage residual malocclusion.3 Palatal fracture patterns can be classified as follows:
We present a case of a 15-year-old male who attended our emergency department following a motorized bike accident. He presented with a minimally displaced Le Fort 2 facial fracture and a Type III (sagittal) fracture of his palate. The traumatic mid-palatal suture diastasis resulted in an upper midline central incisor diastema and tendencies towards a posterior scissor bite on the right hand side, causing aesthetic and functional challenges for management.
Surgical intervention would have required arch bar reduction of the fractured segments of the maxilla, transpalatal rigid plate fixation of the palate and post-operative intermaxillary fixation to stabilize the occlusion. This procedure under a general anaesthetic would afford the benefits of a direct reduction and fixation of the fracture. However, the risks would include: periodontal damage to teeth; hardware exposure or infection; oronasal communication; palatal mucosa necrosis; and the need for a secondary general anaesthetic to remove arch bars and the fixation plate to prevent maxillary growth disturbance. To avoid surgical intervention, a joint oral and maxillofacial surgical and orthodontic treatment plan was agreed to consider a non-surgical approach.
Maxillary expansion treatments have been used for more than a century to correct maxillary transverse deficiency.4 Rapid maxillary expansion (RME) is an effective procedure that is able to produce transverse skeletal effects on the maxilla by opening the mid-palatal suture.5 A Hyrax expander is a type of tooth-bourne RME that makes use of a special screw, HYRAX (hygenic rapid expander). It is essentially a jackscrew with an all-wire frame.6 The screws have heavy gauge wire extensions that are adapted to follow the palatal contours and soldered to bands on premolar and molar. Each quarter turn of the screw produces approximately 0.2 mm of lateral expansion.
The amount of skeletal or dento-alveolar effect of the RME is directly correlated with the stage of skeletal maturation of the palatal suture. The current evidence varies, in that some studies show that mid-palatal suture maturation could be observed as non-mature even in adults.7,8,9 One study evaluating the mid-palatal suture maturation stages in adolescents and young adults using cone-beam computed tomography (CBCT), however, concluded that fusion of the mid-palatal suture was completed after the age of 11 years in females and 14–17 years in males. Overall, it has been concluded that there is a significant variation in the timing of skeletal maturation among individuals as the palatal suture fuses. Generally speaking, the expansion by opening of the palatal suture progressively becomes more difficult as patients grow older.10,11
The understanding of this biological process allows orthodontists to correct transverse growth discrepancies of the maxilla. In the same way that the hyrax appliance can be used to to achieve rapid expansion, paradoxically, the same appliance can be used to allow rapid maxillary contraction (RMC) by contracting the suture. For this reason, owing to the patient's skeletal immaturity, a specialized ‘reverse hyrax’ device was designed and constructed to enable RMC of the maxilla.
Diagnosis and aetiology
A 15-year-old male sustained facial injuries following a motorized bike accident. No head and facial helmet protection was worn during the impact. Following a primary survey, head and cervical spinal injury was clinically and radiologically excluded. The primary patient complaint was the development of an upper central incisor diastema and malocclusion following the injury.
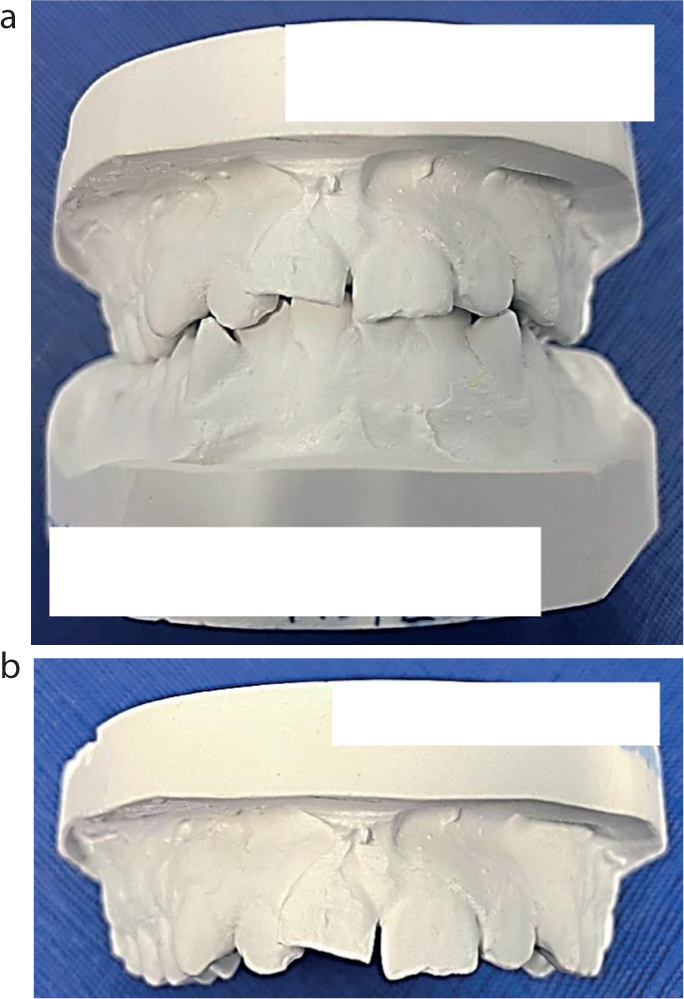
Comprehensive facial and intra-oral examination revealed palatal bruising following the course of the mid palatal suture and tendencies towards scissor biting posteriorly on the right side. The patient had a Class 2 intermediate incisor relationship, and there was a 1-mm upper central incisor diastema that the patient said he did not have before (Figure 1). There were no specific traumatic dental injuries with all teeth intact and immobile. The patient had had no previous dental treatment and was medically fit and well with no allergies.
Figure 1.
(a,b) Study models exhibiting the midline diastema.
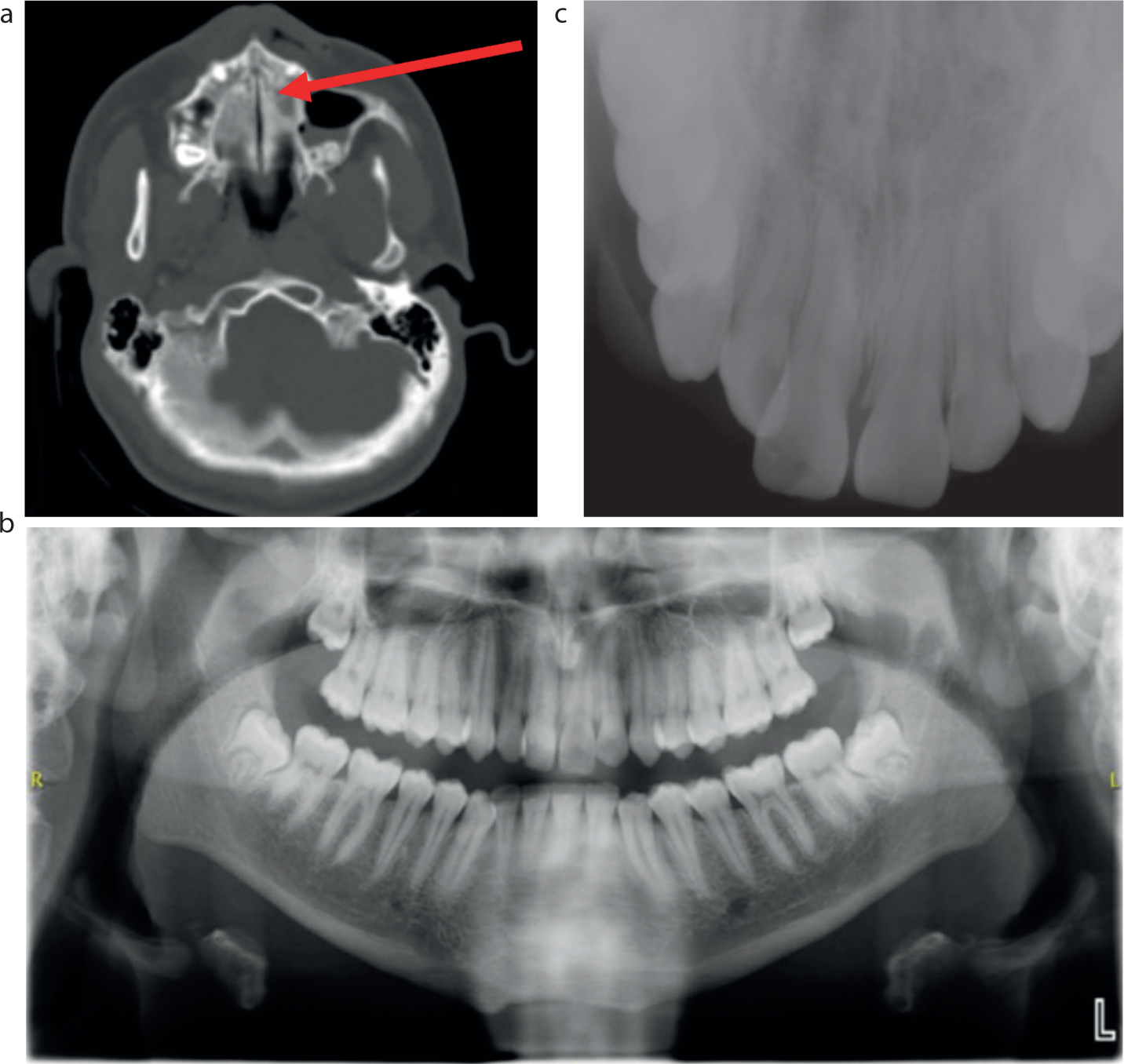
Computed tomography and plain film radiography confirmed a minimally displaced Le Fort II fracture and diastases of the mid-palatal suture (Type III palatal fracture) (Figure 2).
Figure 2.
(a) CT head axial view exhibiting the mid-palatal suture diastases. (b) OPG demonstrating the diastema between the UL1 and UR1. No dental trauma can be seen. (c) Upper standard occlusal imaging where the diastema between the UL1 and UR1 is visible.
Treatment aims and plan
The primary treatment aims were to reduce and stabilize the palatal fracture to allow appropriate healing and also re-establish occlusion in the correct position. Initial management included analgesia, antiseptic mouthwash, soft diet and maxillary sinus pressure control advice.
A joint orthodontic/oral and maxillofacial surgery multidisciplinary approach was undertaken. Clinical and radiological exam, as well as dental study cast and photographic analysis were used to formulate the definitive treatment plan: conservative management of the Le Fort II fracture, transverse contraction of the maxilla using a ‘reverse’ hyrax appliance and stabilization of the post-treatment occlusion.
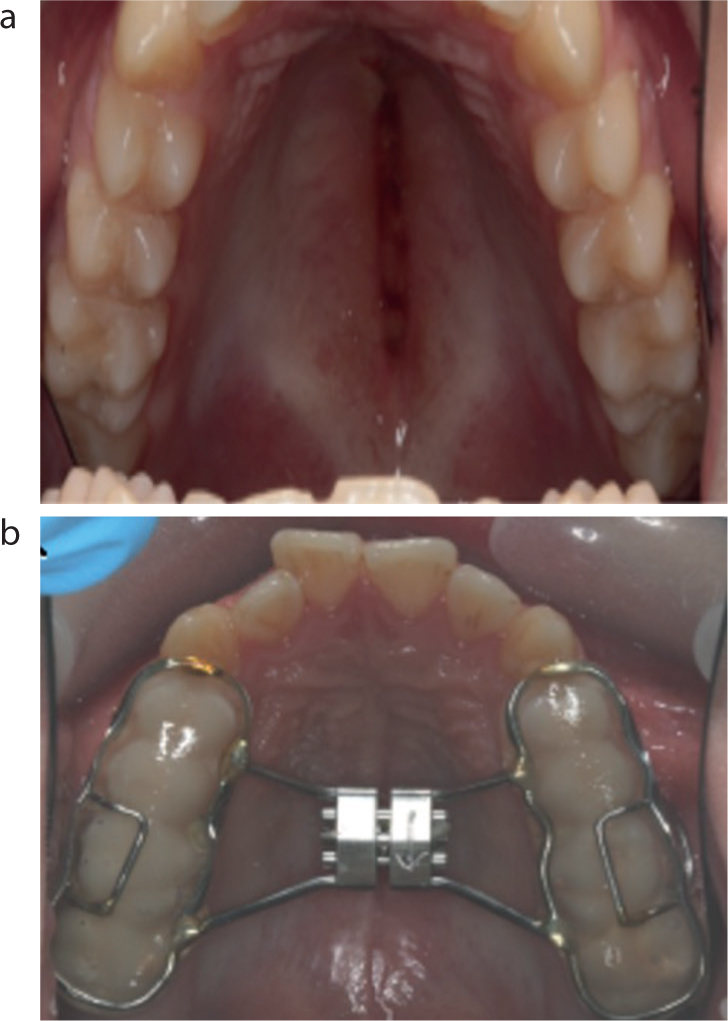
A ‘reverse’ hyrax appliance was constructed using the patient's upper dental study model cast. The laboratory technician was instructed to construct a conventional form of the appliance with the key mechanism ‘reversed’. This would allow for the appliance to contract when the key is turned from anterior to posterior. The patient was instructed on how to turn the key mechanism. The bonded RME appliance was fitted by the orthodontic team with anchorage of the upper premolars and molars (Figure 3). It was cemented with a light-cured glass ionomer cement (GC Fuji LC, GC UK Ltd). The key was then turned once (0.2-mm contraction). The patient was then instructed to turn the key twice a day for 2 consecutive days (2 x 0.2 mm x 2 = 0.8-mm contraction), all this with the aim of closing the 1-mm diastema.
Figure 3.
(a) Midline ecchymosis visible. (b) One week of treatment with the Hyrax appliance. The palatal split has been reduced.
Treatment outcome and follow up
On clinical review 7 days later, the diastema had completely closed, with the posterior transverse discrepancy corrected with the scissor bite tendency resolved (Figure 3). His incisor relationship remained as before the accident. The appliance remained in situ for a further 7 weeks to allow stabilization of the occlusion and to splint the palate. A final review was scheduled with both the orthodontic and oral and maxillofacial surgery team at week 8 to assess progress. At this appointment the appliance was removed. The palate had healed and was stable with no remaining diastema (Figure 3).
Discussion
Isolated palatal fractures are not common and are usually associated with concomitant midfacial fractures. Even in these instances, the incidence is low (around 10%).12 The most common causes of injury are assault and road traffic accidents. Clinical signs suggestive of these fractures include palatal ecchymosis in closed fractures, and lacerations of the upper lip or the palatal mucosa, loss of incisor teeth, occlusal disruption and maxillary tooth diastasis.13
René Le Fort (30 March 1869–30 March 1951) reported that fracture lines of the midface tend to travel through the path of least resistance. The palatal suture line is similar to the cranium and forms a strong synostosis during adolescence, with synostosis completion between the ages of 11and 13 years in females and 14 and 16 years in males (although the start and the advance of fusion of the MPS has been reported to vary greatly with age and sex).14 Thus in pre-adolescent patients any split would tend to be in the midline; however, these fractures are less common in children owing to the elasticity of their facial skeleton, delay in palatal suture synostosis, and the significant amount of force required to fracture the palate.15 It is this delay in the MPS synostosis that makes management of a traumatic MPS diastasis possible with an orthodontic appliance alone.
Treatment of a palatal fracture is planned and performed with the goal of restoring the transverse width of the palate, the anteroposterior projection of the maxillary arch, and the patient's prior occlusion. Treatment options range from orthodontic appliances, palatal splinting, arch bars for maxillomandibular fixation to internal fixation, with plates and screws placed under the palate mucosa and periosteum, together with alveolar plating.16 Our patient did not experience a true palatal fracture, but instead a diastasis of the MPS suture. This had not fully fused at the time of the injury, giving it the potential to move quickly and effectively under the correct applied forces. Even so, the treatment aims remain the same as in a true palatal fracture with, in this case, the addition of aesthetic benefit by closure of the diastema between the UL1 and UR1, as well as correction of the posterior transverse malocclusion.
The hyrax is a screw type of appliance that is traditionally used in orthodontic appliances to expand the upper arch. By turning the screw 1–2 times a day, a rapid expansion force can be applied. When the screw is turned 1–2 times a day, the periodontal ligament on the buccal surfaces of the teeth is compressed and lateral force builds up bilaterally in the posterior maxilla. The weakest point in a young patient is the midline suture, and this is split open, causing expansion of the maxilla. In this case, the hyrax screw was mounted in reverse so that turning the screw caused contraction of the upper arch.
A combined orthodontic/oral and maxillofacial surgery multidisciplinary approach helped devise the treatment plan. Knowledge of RME appliances, MPS maturation and morphology were used to create a hyrax appliance that contracted the maxillary arch instead of expanding it. The appliance was designed such that the key was turned in the opposite direction to usual, thus contracting and, therefore, reducing the diastasis. After 1 week of the appliance being in situ, the diastema and posterior scissors bite had been successfully treated. The appliance was left in situ for a total of 7 weeks for stabilization.
Management of these injuries is not well documented due to low incidence. However, in a study carried out in 2015, 13 patients underwent palatal fracture management using a palatal splint made from a rapid light-cure resin, sometimes in conjunction with intermaxillary fixation. It was deemed successful and cost-effective. Other documented treatments involve placing a palatal splint, then physically reducing palatal fractures by applying pressure laterally on the two maxillary halves while applying arch bars; however, there has been no report on the effectiveness of this method.10 Despite previous use of orthodontic appliances in palatal injuries, no cases of using a ‘reverse RME’ to treat a traumatic MPS diastasis have been recorded.
In this case, allowing healing of the bony segments in their current positions with no intervention was an option6. However, this would have left the patient with a residual upper central incisor diastema and occlusal discrepancy, potentially resulting in in the need for future restorative and/or orthodontic treatment. Furthermore, it would have left the patient unhappy in terms of aesthetics. Palatal fractures require rigid horizontal stability of the dentition along with restoration of midface projection and height.9 This case demonstrates the possibility to achieve this via non-invasive management. The treatment carried out was reliant on patient compliance; adapting to the intra-oral device, maintenance of oral hygiene and ensuring that correct instructions regarding the key turns was followed. It is also important to carry our regular reviews, and imperative to ensure succinct communication with the lab in construction of the appliance for a successful outcome.
Conclusion
In this case, a novel approach to reduction of a traumatic mid-palatal fracture was successfully employed, using an orthodontic appliance. It is important to think beyond the conventional approach in managing traumatic facial fractures and it is important that treatment planning is approached analytically and flexibly to bring a range of approaches to problem-solving. Current knowledge of well-known clinical practices, combined with a multidisciplinary approach made it possible to create a new and effective way of treating this type of injury.
Learning points
It is possible to use a rapid maxillary expansion orthodontic appliance in reverse to close a midline fracture.
It is important to be aware of the consequences of a traumatic mid-palatal suture diastasis, including restorative and orthodontic implications.
Consider a patient's age and anatomical development because this may affect treatment options. Take advantage of this to enhance the natural biological healing process.
Management of injuries in children may differ from that of adults with the same injury.
Use current clinical knowledge to find innovative ways to treat facial fractures, where appropriate.