Suri L, Gagari E, Vastardis H. Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004; 126:432-445 https://doi.org/10.1016/j.ajodo.2003.10.031
Leyland L, Batra P, Wong F, Llewelyn R. A retrospective evaluation of the eruption of impacted permanent incisors after extraction of supernumerary teeth. J Clin Pediatr Dent. 2006; 30:225-231 https://doi.org/10.17796/jcpd.30.3.60p6533732v56827
Ashkenazi M, Greenberg BP, Chodik G, Rakocz M. Postoperative prognosis of unerupted teeth after removal of supernumerary teeth or odontomas. Am J Orthod Dentofacial Orthop. 2007; 131:614-619 https://doi.org/10.1016/j.ajodo.2005.09.032
Katz RW. An analysis of compound and complex odontomas. ASDC J Dent Child. 1989; 56:445-449
Topouzelis N, Tsaousoglou P, Pisoka V, Zouloumis L. Dilaceration of maxillary central incisor: a literature review. Dent Traumatol. 2010; 26:427-433 https://doi.org/10.1111/j.1600-9657.2010.00915.x
Chaushu S, Becker T, Becker A. Impacted central incisors: factors affecting prognosis and treatment duration. Am J Orthod Dentofacial Orthop. 2015; 147:355-362 https://doi.org/10.1016/j.ajodo.2014.11.019
Foley J. Surgical removal of supernumerary teeth and the fate of incisor eruption. Eur J Paediatr Dent. 2004; 5:35-40
Mason C, Azam N, Holt RD, Rule DC. A retrospective study of unerupted maxillary incisors associated with supernumerary teeth. Br J Oral Maxillofac Surg. 2000; 38:62-65 https://doi.org/10.1054/bjom.1999.0210
Kokich VG, Crabill KE. Managing the patient with missing or malformed maxillary central incisors. Am J Orthod Dentofacial Orthop. 2006; 129:S55-63 https://doi.org/10.1016/j.ajodo.2005.11.007
Management of Bilateral Horizontally Impacted and Dilacerated Maxillary Central Incisors at the Nasal Floor: A Multidisciplinary Specialist Approach Paula Mairéad Sinnott Orthodontic Update 2025 14:4, 180-185.
Senior Orthodontic Registrar, Department of Orthodontics, University of Bristol Dental Hospital, University Hospitals Bristol NHS Foundation Trust, Bristol
In cases of horizontally impacted and dilacerated maxillary central incisors where alignment is attempted, treatment is often prolonged, and achieving an optimal result can be uncertain. We present a case of bilateral horizontally impacted maxillary central incisors lying against the nasal floor, associated with supernumerary teeth, further complicated by a dilaceration, where alignment of the impacted incisors was completed efficiently.
CPD/Clinical Relevance: To demonstrate an orthodontic case of how impacted dilacerated central incisors at the nasal floor were efficiently aligned.
Article
Impacted maxillary central incisors are relatively rare with a reported incidence of 0.06–0.2% in the general population.1 Impacted maxillary central incisors have a significant effect on dental and facial aesthetics, and this can be especially concerning for young children.2 A maxillary central incisor is generally considered to have delayed eruption if: there is eruption of contralateral teeth greater than 6 months previously; maxillary incisors remain unerupted more than 1 year following the eruption of mandibular incisors; or if there is a deviation of the normal eruption sequence, for example lateral incisors erupting before central incisors.3
The literature reveals multiple different causes of impacted maxillary incisors and include local causes, such as supernumerary teeth, dental malformations, dilacerations, ectopic position of the tooth bud,4 non-vital or ankylosed deciduous teeth,5 gingival fibromatosis and systemic conditions including cleidocranial dysplasia.6 Supernumeraries are the most common cause (56–60%) of maxillary incisor impactions, with tuberculate supernumeraries being more likely to hinder eruption than conical supernumeraries.7,8 Odontomes have been suggested by others to cause delayed eruption or impaction of maxillary central incisors in approximately 28–60% of cases,5 with complex odontomes more commonly causing impactions than their compound counterparts.9
The Royal College of Surgeons of England has published guidelines for the management of unerupted maxillary incisors that discuss the possible management considerations, including accepting the impaction, removing retained deciduous teeth, creating and maintaining sufficient space, removal of physical obstructions, such as supernumerary teeth, exposure and bonding of impacted incisors, or surgical removal.3 If a general anaesthetic is required for the removal of an obstruction, consideration should also be given to exposing and bonding the impacted tooth at the same time to avoid a second general anaesthetic.
When exposure and bonding of impacted incisors is indicated, this can involve applying orthodontic traction using either fixed or removable orthodontic appliances. The benefits of aligning impacted maxillary incisors include improved dental aesthetics, psychological benefits, space maintenance and bone preservation. Potential limitations include prolonged treatment duration, poor gingival aesthetics, root resorption and the possibility of ankylosis preventing alignment of the tooth.10
The vertical position of impacted maxillary central incisors relative to the occlusal plane, has been reported to affect both the chance of successful eruption and the time period required for alignment of the impacted tooth.11 In this case, the central incisors were lying against the nasal floor, therefore, they were in an unfavourable position for spontaneous eruption. Another factor to consider is the stage of root development. It is commonly thought that teeth with immature apices have a greater potential for alignment than those with a closed apex.12,13 In this case, both central incisors had immature open apices, which was a favourable factor in aligning these teeth. An alternative management approach for impacted incisors that are in an unfavourable position is surgical removal. The lateral incisor may then be aligned into the central incisor position and camouflaged as the central incisor. Kokich and Crabill14 suggested using this approach and then re-opening the space for the maxillary central incisor using fixed appliances for eventual replacement of this tooth when the patient is in the permanent dentition. They proposed that this treatment approach has the benefit of preserving alveolar bone in the maxillary central incisor region, which can be beneficial for when the tooth is eventually replaced, because it may negate the need for a bone graft. Alternatively, surgical removal followed by restoratively replacing the tooth, may be a suitable approach in some cases. This case report describes the multidisciplinary management of a 9-year-old patient, who presented with bilateral horizontally impacted maxillary central incisors that were lying against the nasal floor, and further complicated by a dilaceration.
Case report
A 9-year-old girl was referred to a joint orthodontic–paediatric clinic for assessment of her impacted maxillary central incisors, and for advice on the comprehensive management of these teeth. The patient had a history of trauma to the maxillary deciduous anterior teeth when she was approximately 3 years old. The teeth were not reported to have been displaced and no active treatment was required for the trauma.
Clinical assessment
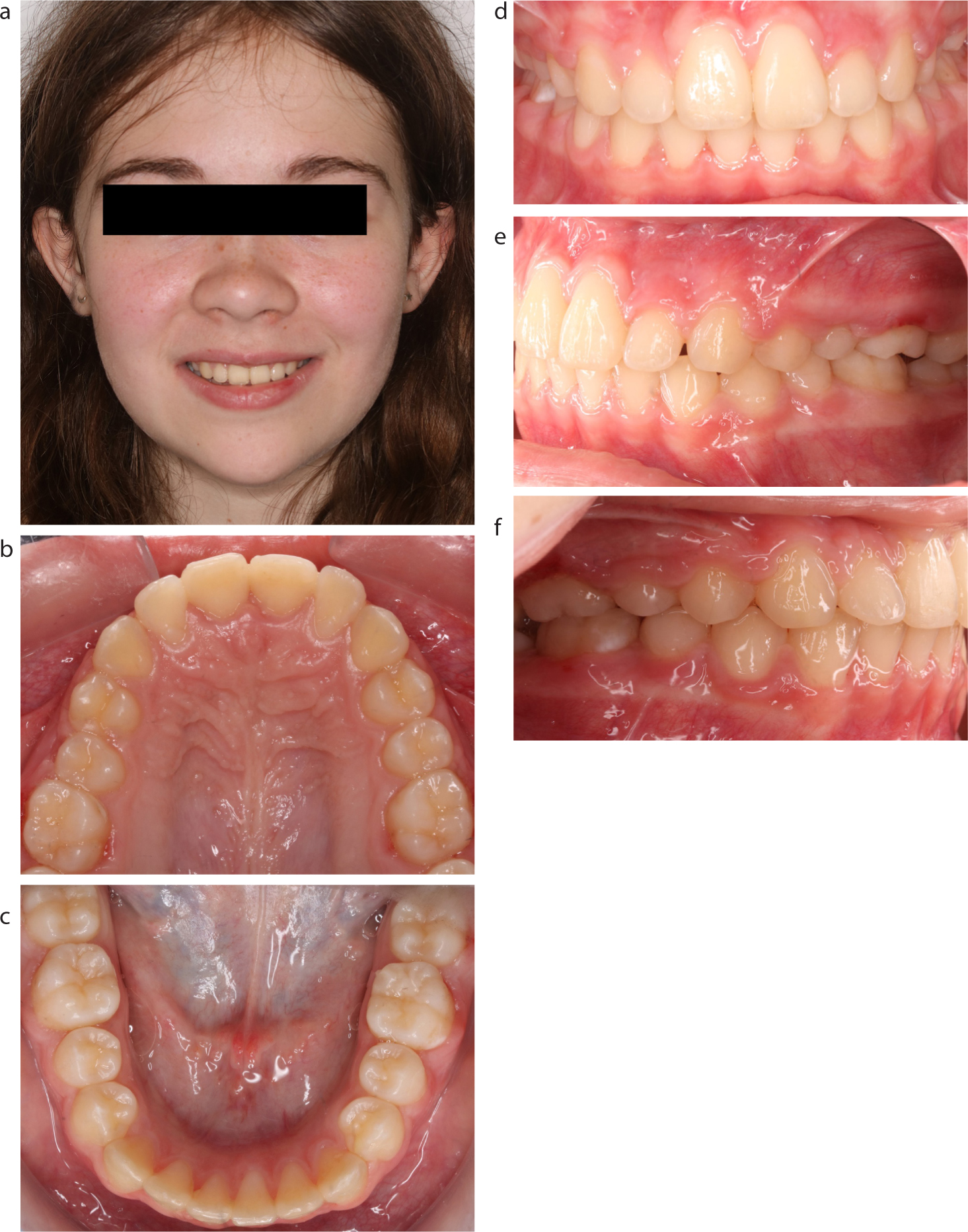
The patient presented with a Class I skeletal base relationship with average vertical proportions and no facial asymmetry. Intra-orally, the patient was in the mixed dentition with the absence of the maxillary right and left permanent central incisors, which could not be palpated. The patient had features of a Class II malocclusion with mild crowding in the lower arch and 16 mm of space available in the upper arch for the unerupted maxillary incisors (Figure 1).
Figure 1. Pre-treatment views: (a) frontal extra-oral; (b) upper occlusal; (c) lower occlusal; (d) frontal intra-oral; (e) left buccal; and (f) right buccal.
Radiographic assessment
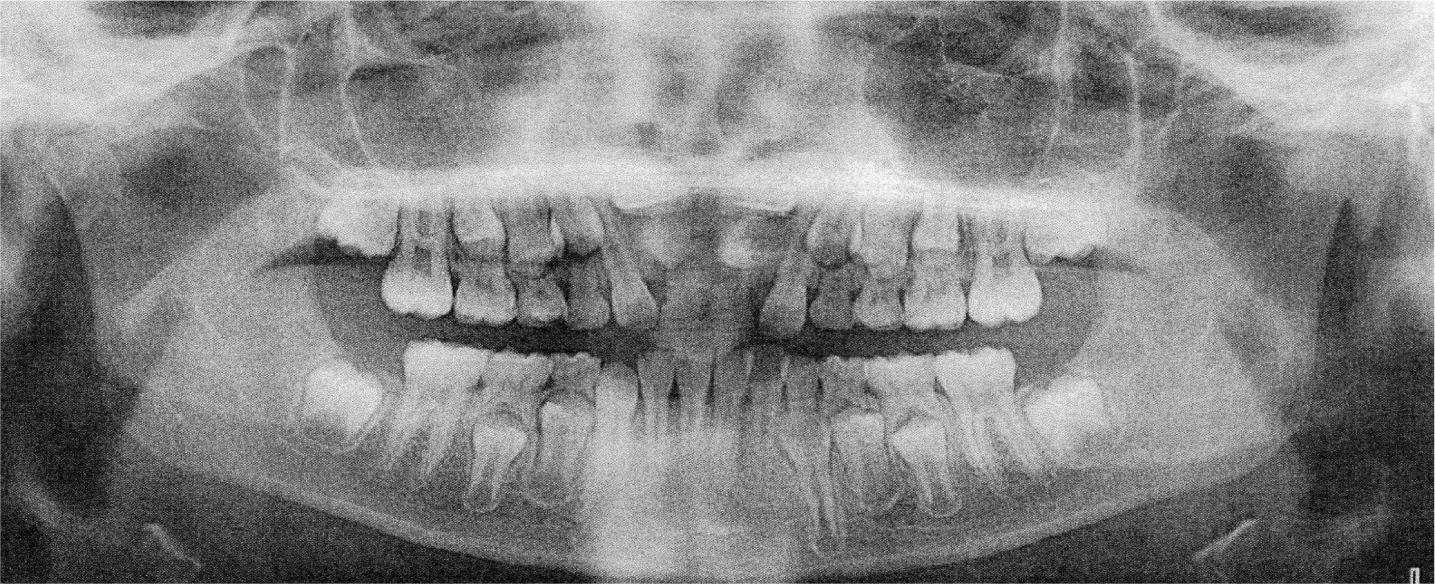
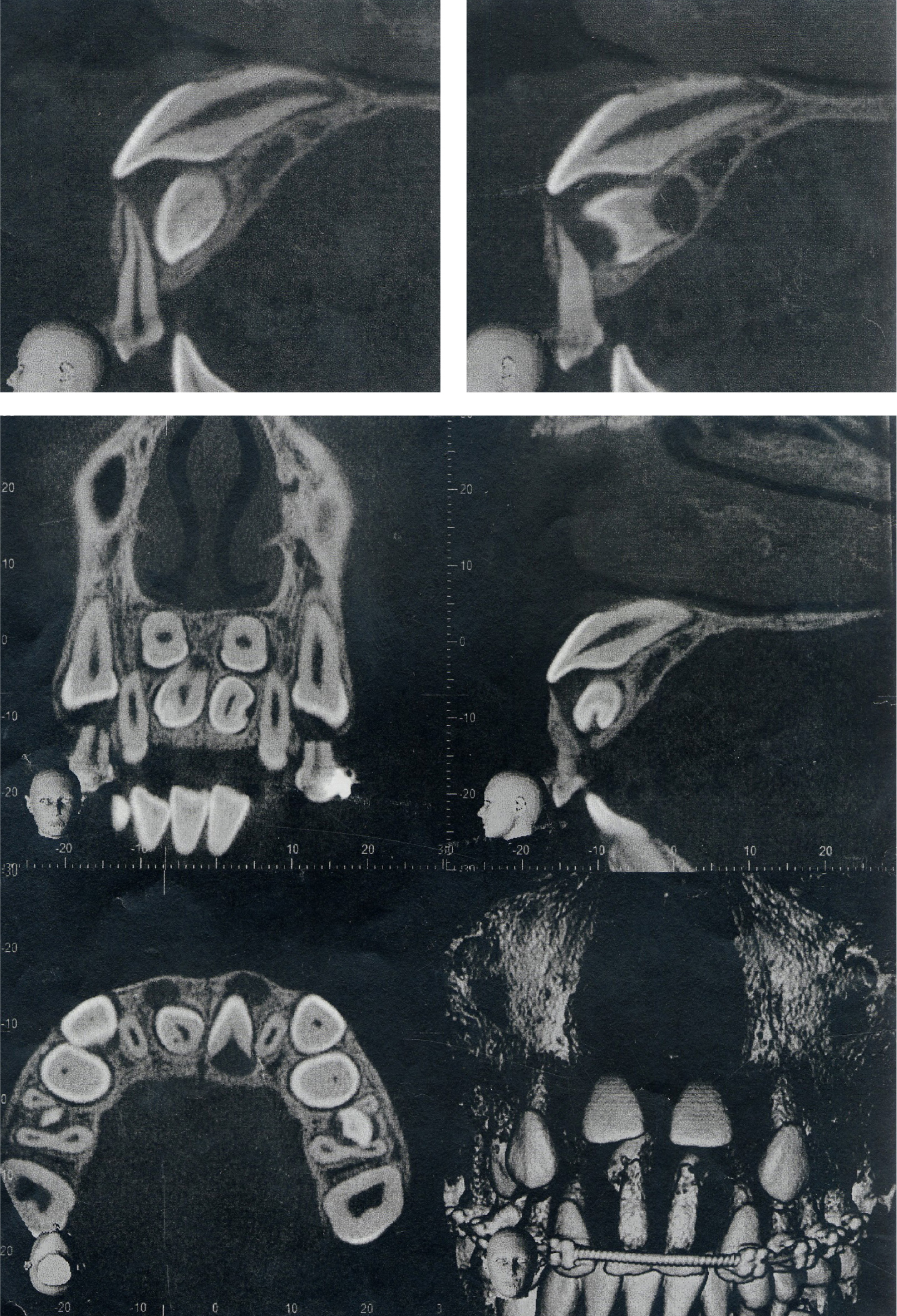
The dental panoramic tomograph (DPT), taken by the referring orthodontic department, showed the presence of two unerupted supernumeraries in the maxillary central incisor region associated with the impacted maxillary central incisors (Figure 2). A CBCT showed that the maxillary right and left central incisors were both horizontally impacted and were in a high position, lying against the floor of the nasal cavity. Both central incisors had open apices, and straight roots in the bucco-lingual direction. Both central incisors were associated with supernumerary teeth, lying below the crowns of the incisors (Figure 3). There was no evidence of cystic change or root resorption of adjacent teeth and the deciduous maxillary central incisors were retained at the time of the CBCT. The dilaceration in the apical third of the root of the maxillary right central incisor was not evident on the CBCT because it was taken before the root had fully developed.
Figure 2. Pre-treatment orthopantomogram showing impacted upper central incisors and supernumerary tuberculate teeth.Figure 3. Cone beam CT showing impacted central incisors lying against the nasal floor
Aetiology
The horizontally impacted maxillary right and left central incisors were associated with two supernumeraries lying below the crowns of the incisors, preventing them from erupting.
Treatment
The treatment plan and rationale was as follows:
Surgical extraction of the two maxillary supernumerary teeth, and exposure and bonding with the placement of gold chains on the maxillary right and left central incisors by the paediatric dentistry department.
Upper removable appliance to attempt alignment of the impacted maxillary central incisors.
Review dental development and the overall malocclusion, and assess the need for upper and lower fixed appliances for comprehensive correction of the malocclusion.
Treatment progress
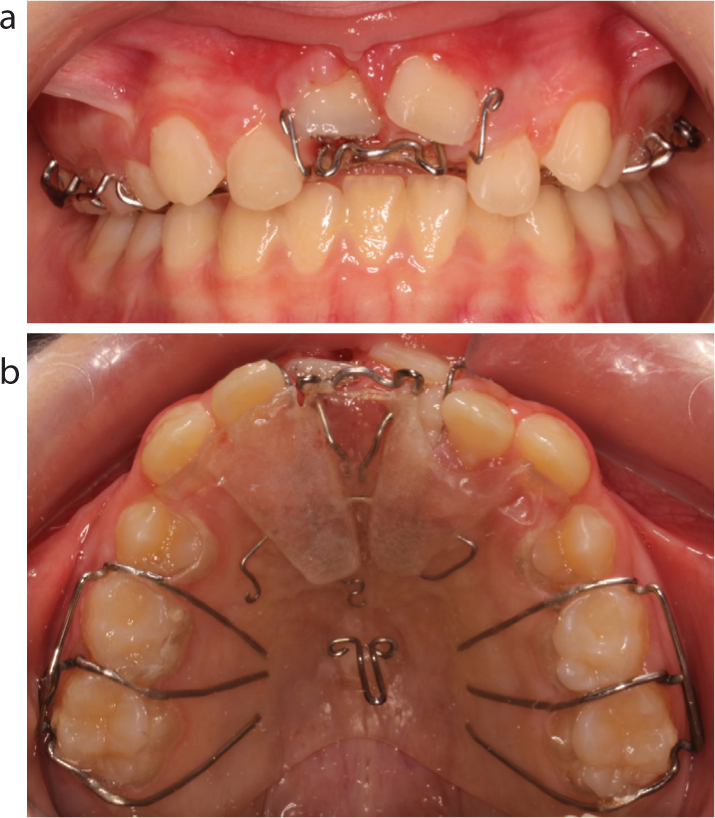
The maxillary central incisors were exposed and bonded using a closed technique with incisal edge attachments with a low profile to reduce the risk of gingival fenestration and poor gingival aesthetics compared to conventional gold chain attachments. Following this, an upper removable appliance was used to apply traction to the impacted incisors. Traction was applied via S-hooks formed from a 0.016” x 0.022” stainless steel archwire, which were attached to the chains on the incisal edge attachments on the central incisors. The patient applied elastics from these S-hooks to a hook on the palatal surface of the upper removable appliance to apply traction to the impacted incisors. The patient had excellent compliance, and the maxillary central incisors both erupted within 3 months (Figure 4). Following this, a sectional upper fixed appliance was placed from the maxillary right canine to the maxillary left canine, excluding the central incisors, to initially align adjacent teeth and then create more space for further alignment of the central incisors. Following successful completion of the initial phase of treatment to align the impacted maxillary central incisors, all the permanent successor teeth had erupted and the patient was in the permanent dentition with a mild Class II division 1 malocclusion with a 4 mm overjet and mild crowding in the upper and lower arches. A long cone peri-apical radiograph showed a dilaceration in the apical third of the root of the maxillary right central incisor with no other associated pathology evident (Figure 5). Upper and lower fixed appliances were planned on a non-extraction basis. This treatment plan was agreed to achieve alignment of the upper and lower arches, while minimizing the length of treatment. Figure 6 shows the final treatment result.
Figure 4. Upper removable appliance with erupted central incisors: (a) frontal view; and (b) occlusal view.Figure 5. Long cone peri-apical of the upper central incisors showing a mild apical dilaceration of the upper right central incisor.Figure 6. Debonded treatment views: (a) frontal extra-oral; (b) upper occlusal; (c) lower occlusal; (d) frontal intra-oral; (e) left buccal; and (f) right buccal.
Discussion
This case demonstrates a favourable treatment result using a multidisciplinary approach to ensure input from orthodontics, paediatrics and oral surgery with the management of the case. Excellent communication with the patient and her parents was crucial to the successful management of this case, especially with regard to ensuring that the associated risks and limitations were comprehensively discussed, as well as the compliance required by the patient with elastic wear and the likely prolonged nature of the treatment.
A CBCT was indicated in this case to gain more information on the impacted maxillary central incisors and the associated supernumerary teeth, which could not be fully visualized on the plain film radiographs.15 However, the dilaceration in the apical third of the root of the maxillary right central incisor could not be seen on the CBCT because it was taken before the root had fully developed. A dilaceration is described as an acute deviation of the long axis of a tooth that can occur at the crown or the root of a tooth.16 The aetiology of dilacerations include developmental factors (70%)17 or environmental factors (20–30%), such as dental trauma at the time of development of the affected tooth.10 A removable appliance was used to provide good anchorage, facilitate the application of traction to the impacted incisors, and allow continual force to be applied as the patient changed the elastic daily. Increased patient compliance was, however, required with this treatment approach compared to using fixed appliances. Continual traction was especially important given the vertical distance of the two maxillary central incisors from the occlusal plane. There are varying reports of treatment duration for aligning impacted maxillary incisors, extending up to 18 months of orthodontic traction.7 In the case presented, despite the suboptimal position of the impacted maxillary central incisors and the dilaceration of the right maxillary central incisor root, both central incisors were successfully moved into the mouth within 3 months of applying orthodontic traction.
Summary
Impacted incisors that are a substantial distance from the occlusal plane can be amenable to alignment. To improve the likelihood of a favourable outcome, a multidisciplinary approach may be advised, permitting treatment plans to be formulated with the expertise of all relevant specialities.
CBCT can play a role in assessing impacted teeth and can facilitate orthodontic treatment planning in some cases.
Good communication with the patient and parents is essential to the successful management of cases involving complex impactions.