Kamaluddin JM, Cobourne MT, Sherriff M, Bister D. Does the Eastman correction over- or under-adjust ANB for positional changes of N?. Eur J Orthod. 2012; 34:719-723 https://doi.org/10.1093/ejo/cjr108
Ishikawa H, Nakamura S, Iwasaki H, Kitazawa S. Seven parameters describing anteroposterior jaw relationships: postpubertal prediction accuracy and interchangeability. Am J Orthod Dentofacial Orthop. 2000; 117:714-720
Midtgard J, Bjork G, Linder-Aronson S. Reproducibility of cephalometric landmarks and errors of measurements of cephalometric cranial distances. Angle Orthod. 1974; 44:56-61
Baumrind S, Frantz RC. The reliability of head film measurements. 2. Conventional angular and linear measures. Am J Orthod. 1971; 60:505-517 https://doi.org/10.1016/0002-9416(71)90116-3
Periago DR, Scarfe WC, Moshiri M Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod. 2008; 78:387-395 https://doi.org/10.2319/122106-52.1
Pittayapat P, Limchaichana-Bolstad N, Willems G, Jacobs R. Three-dimensional cephalometric analysis in orthodontics: a systematic review. Orthod Craniofac Res. 2014; 17:69-91 https://doi.org/10.1111/ocr.12034
Juerchott A, Saleem MA, Hilgenfeld T 3D cephalometric analysis using magnetic resonance imaging: validation of accuracy and reproducibility. Sci Rep. 2018; 8 https://doi.org/10.1038/s41598-018-31384-8
Heil A, Lazo Gonzalez E, Hilgenfeld T Lateral cephalometric analysis for treatment planning in orthodontics based on MRI compared with radiographs: A feasibility study in children and adolescents. PLoS One. 2017; 12 https://doi.org/10.1371/journal.pone.0174524
Lin HH, Lo LJ. Three-dimensional computer-assisted surgical simulation and intraoperative navigation in orthognathic surgery: a literature review. J Formos Med Assoc. 2015; 114:300-307 https://doi.org/10.1016/j.jfma.2015.01.017
Houston WJ, Edler R. Long-term stability of the lower labial segment relative to the A-Pog line. Eur J Orthod. 1990; 12:302-310 https://doi.org/10.1093/ejo/12.3.302
Ricketts RM. Planning treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod. 1957; 27:14-37
Hsu BS. Comparisons of the five analytic reference lines of the horizontal lip position: their consistency and sensitivity. Am J Orthod Dentofacial Orthop. 1993; 104:355-360
Songra G, Mittal T, Williams J Assessment of growth in orthodontics. Orthod Update. 2017:16-23
Riolo ML. An atlas of craniofacial growth: cephalometric standards from the University school growth study, the University of Michigan.Ann Arbor: Center for Human Growth and Development, University of Michigan; 1974
Hans MG, Broadbent BH, Nelson SS. The Broadbent–Bolton Growth Study – past, present, and future. Am J Orthod Dentofacial Orthop. 1994; 105:598-603 https://doi.org/10.1016/S0889-5406(94)70145-8
Behrents RG.: University of Michigan; 1984
Al-Jewair T, Stellrecht E, Lewandowski L, Chakaki R. American Association of Orthodontists Foundation Craniofacial Growth Legacy Collection in the orthodontic literature-use and trends: a systematic review. Am J Orthod Dentofacial Orthop. 2018; 153:15-25 https://doi.org/10.1016/j.ajodo.2017.07.015
Bjork A. The use of metallic implants in the study of facial growth in children: method and application. Am J Phys Anthropol. 1968; 29:243-254 https://doi.org/10.1002/ajpa.1330290217
Rogers K, Campbell PM, Tadlock L Treatment changes of hypo- and hyperdivergent Class II Herbst patients. Angle Orthod. 2018; 88:3-9 https://doi.org/10.2319/060117-369.1
von Bremen J, Pancherz H. Association between Bjork's structural signs of mandibular growth rotation and skeletofacial morphology. Angle Orthod. 2005; 75:506-509
Lamparski DG. Skeletal age assessment utilizing cervical vetebrae. Am J Orthod Dentofacial Orthop. 1975; 67:458-459
Baccetti T, Franchi L, McNamara J. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod. 2005:119-129
Szemraj A, Wojtaszek-Slominska A, Racka-Pilszak B. Is the cervical vertebral maturation (CVM) method effective enough to replace the hand-wrist maturation (HWM) method in determining skeletal maturation?-A systematic review. Eur J Radiol. 2018; 102:125-128 https://doi.org/10.1016/j.ejrad.2018.03.012
Rainey BJ, Burnside G, Harrison JE. Reliability of cervical vertebral maturation staging. Am J Orthod Dentofacial Orthop. 2016; 150:98-104 https://doi.org/10.1016/j.ajodo.2015.12.013
Engel TP, Renkema AM, Katsaros C The cervical vertebrae maturation (CVM) method cannot predict craniofacial growth in girls with Class II malocclusion. Eur J Orthod. 2016; 38:1-7 https://doi.org/10.1093/ejo/cju085
Gabriel DB, Southard KA, Qian F Cervical vertebrae maturation method: poor reproducibility. Am J Orthod Dentofacial Orthop. 2009; 136:478 e471-477 https://doi.org/10.1016/j.ajodo.2007.08.028
Predko-Engel A, Kaminek M, Langova K Reliability of the cervical vertebrae maturation (CVM) method. Bratisl Lek Listy. 2015; 116:222-226 https://doi.org/10.4149/bll_2015_043
Brodie AJ. On the growth pattern of the human head. From the third month to the eighth year of life. Am J Anat. 1941;
Bjork A, Skieller V. Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983; 5:1-46 https://doi.org/10.1093/ejo/5.1.1
Popovich F. The Burlington Orthodontic Research Centre. Am J Orthod. 1957; 43:291-293
Papageorgiou SN, Koretsi V, Jager A. Bias from historical control groups used in orthodontic research: a meta-epidemiological study. Eur J Orthod. 2017; 39:98-105 https://doi.org/10.1093/ejo/cjw035
Antoun JS, Cameron C, Sew Hoy W Evidence of secular trends in a collection of historical craniofacial growth studies. Eur J Orthod. 2015; 37:60-66 https://doi.org/10.1093/ejo/cju007
Martin DC, Danforth ME. An analysis of secular change in the human mandible over the last century. Am J Hum Biol. 2009; 21:704-706 https://doi.org/10.1002/ajhb.20866
Tsichlaki A, O'Brien K, Johal A Development of a core outcome set for orthodontic trials using a mixed-methods approach: protocol for a multicentre study. Trials. 2017; 18 https://doi.org/10.1186/s13063-017-2098-x
Pae EK, McKenna GA, Sheehan TJ Role of lateral cephalograms in assessing severity and difficulty of orthodontic cases. Am J Orthod Dentofacial Orthop. 2001; 120:254-262 https://doi.org/10.1067/mod.2001.116825
Nijkamp PG, Habets LL, Aartman IH, Zentner A. The influence of cephalometrics on orthodontic treatment planning. Eur J Orthod. 2008; 30:630-635 https://doi.org/10.1093/ejo/cjn059
Devereux L, Moles D, Cunningham SJ, McKnight M. How important are lateral cephalometric radiographs in orthodontic treatment planning?. Am J Orthod Dentofacial Orthop. 2011; 139:175-181 https://doi.org/10.1016/j.ajodo.2010.09.021
Manosudprasit A, Haghi A, Allareddy V, Masoud MI. Diagnosis and treatment planning of orthodontic patients with 3-dimensional dentofacial records. Am J Orthod Dentofacial Orthop. 2017; 151:1083-1091 https://doi.org/10.1016/j.ajodo.2016.10.037
Han UK, Vig KW, Weintraub JA Consistency of orthodontic treatment decisions relative to diagnostic records. Am J Orthod Dentofacial Orthop. 1991; 100:212-219 https://doi.org/10.1016/0889-5406(91)70058-5
Durao AR, Pittayapat P, Rockenbach MI Validity of 2D lateral cephalometry in orthodontics: a systematic review. Prog Orthod. 2013; 14 https://doi.org/10.1186/2196-1042-14-31
Rischen RJ, Breuning KH, Bronkhorst EM, Kuijpers-Jagtman AM. Records needed for orthodontic diagnosis and treatment planning: a systematic review. PLoS One. 2013; 8 https://doi.org/10.1371/journal.pone.0074186
Atchison KA. Radiographic examinations of orthodontic educators and practitioners. J Dent Educ. 1986; 50:651-655
Steiner C. Cephalometrics in clinical practice. Angle Orthod. 1959; 29:8-29
Orthodontic indications for lateral cephalograms are diagnosis, prescription, prediction and research. Benefits of taking these radiographs must be weighed against the risks of radiation exposure. Various cephalometric analyses have been described, and these are commonly used for diagnosis and treatment planning, but unavoidable errors of both projection and identification can complicate radiographic interpretation. The use of the cervical vertebral maturation technique for growth prediction has been contentious, but may have a useful role in aiding treatment timing. Research outcomes in orthodontics have focused heavily on cephalometrics, but this is starting to change, especially with the development of 3D analysis techniques.
CPD/Clinical Relevance: The range of uses of lateral cephalograms in orthodontic practice and some of the latest research regarding the use of cephalometrics in treatment planning is described.
Article
Cephalometrics uses lateral skull radiographs to assess the positions of the skeletal bases and the inclination of the associated dental structures with respect to the rest of the facial skeleton. Radiographic landmark identification allows angular or linear measurements to be made, and is now most commonly performed digitally.
Leonardo da Vinci was one of the first to use head measurements and a variety of lines related to specific head structures to assist his studies of the human form,1 and it was Birdsall Holly Broadbent Senior who is credited with the development of modern cephalometry.2 Indeed by the 1950s, the technique had become so widespread that a Californian orthodontist, Cecil C Steiner, stated ‘those of you who are not using cephalometrics in your everyday clinical practices now must soon bow to its importance, accept the added burden it imposes, and master its mysteries if you are to discharge your full obligation to your patients’.3 In the latter half of the 20th century the significance of cephalometrics in treatment planning was questioned4 and coincided with the increasing recognition of the importance of minimizing radiation exposure. The importance of cephalometry in the 21st century will be described in this article, alongside alternative approaches.
There are four main purposes of cephalometry; diagnosis, prescription, prediction and research.5 These are discussed in turn.
Diagnosis
Use of the lateral skull radiograph should only be considered as an adjunct to a thorough clinical examination. Indications for cephalometry are outlined in current BOS guidance, where flowcharts are available to help decide whether a pre-treatment lateral cephalometric radiograph is indicated, dependent upon the age of the patient and the malocclusion.6 Lateral skull radiographs can aid localization of unerupted teeth, especially in the anteroposterior dimension, and are used to assess dilacerated teeth.
Analysis of lateral skull radiographs can help determine the aetiology of the malocclusion, with population norms being used as a guide. A number of cephalometric analyses have been described and contain dental, skeletal and/or soft tissue assessments. Only selected analyses will be described below.
Common cephalometric analyses
One of the first clinically oriented cephalometric analyses was described by Downs in 1948.7 His analysis was based on a group of 20 people with ideal occlusions. Ten cephalometric measurements were described, with the Frankfort plane being the key reference plane. Downs reported notable variation around the mean values for each measure and stated how it was important to use all the measurements together, rather than focus on any single measurement in isolation.
It was not until Steiner in 1960 that the line SN was adopted as the horizontal reference plane.8 The Steiner analysis however, is reportedly based on his cephalometric measurement of just two Hollywood stars.
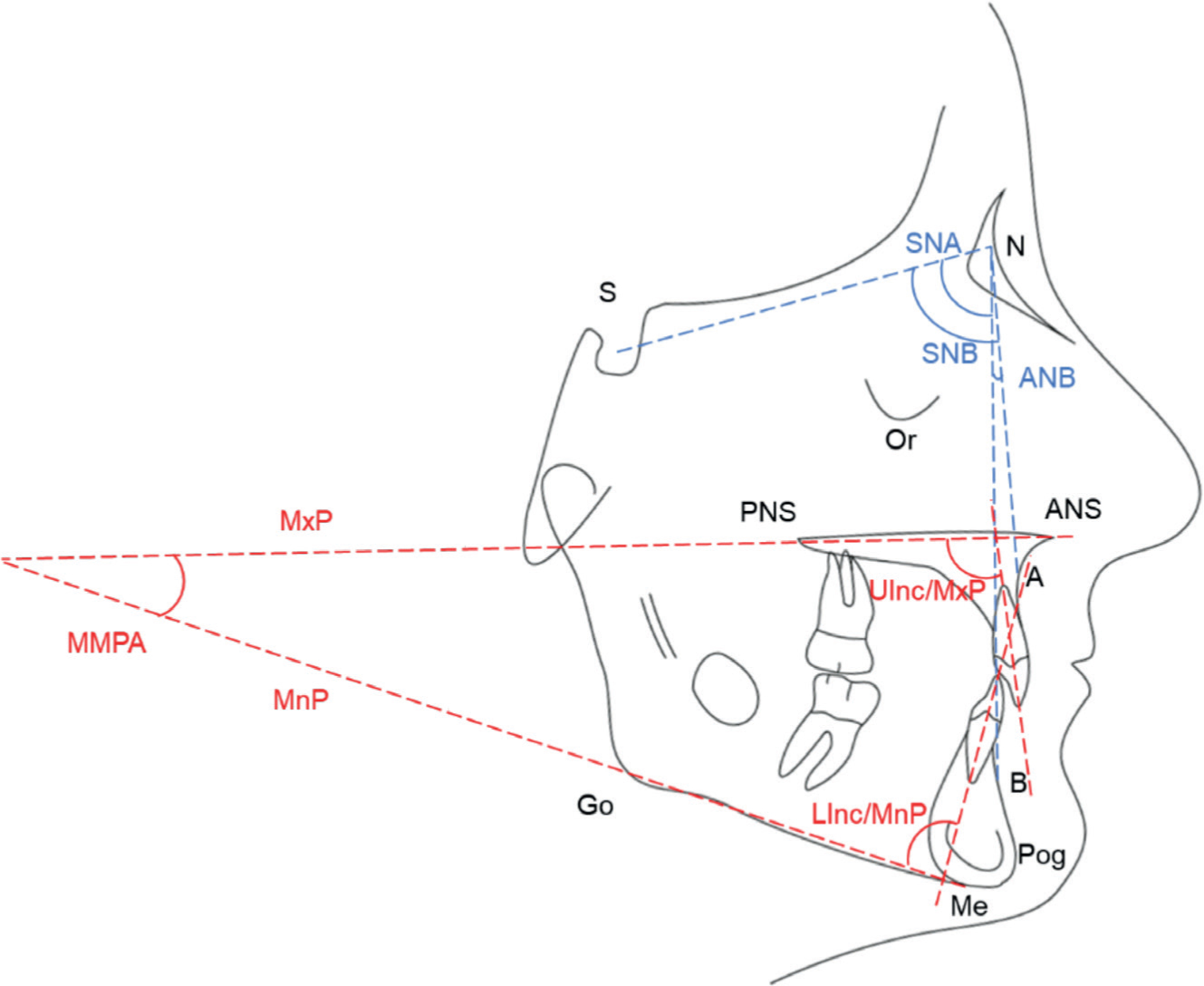
Probably the most popular analysis used in the UK is the Eastman analysis, based on the work of Ballard who analysed 250 London school children of various ages,9 and which was subsequently refined by Mills.10 Commonly used cephalometric points, planes and angles are depicted in Figure 1, with Eastman standard norms and abbreviations listed in Table 1. Cephalometric assessment of skeletal pattern can be determined by comparing the relationship of the maxilla and mandible with the cranial base using angles SNA and SNB. The ANB angle, the difference between SNA and SNB, classifies the skeletal pattern (ANB <2° =Class 3; ANB >4° = Class 2; ANB between 2° and 4° = Class 1).
Cephalometric norms have often been based on small sample sizes and the scientific basis of analyses based on these norms is therefore sometimes weak. In 1956, Graber described some of the limitations of cephalometrics, in particular criticizing the reliance on arbitrary norms and stating that mathematical descriptions of morphology are likely to be an oversimplification.11 For example, when analysing the anteroposterior position of the jaws, there are problems associated with relying only on the ANB angle.12 The Eastman correction described by Mills (1970) attempts to correct for an aberrant position of nasion when SNA is too high or too low and the SN/MxP angle is normal.13 However, the Eastman correction is itself subject to error because in a study based on a geometrical model, the Eastman correction was shown to overestimate towards the opposite skeletal discrepancy when N was moved posteriorly towards S (ie direct measurements showed a Class 2 tendency, whereas the Eastman correction revealed a Class 3 tendency).14 An additional analysis such as the Wits appraisal, which relates anteroposterior discrepancy of the jaws to each other and not to the cranial base, is also recommended.15 This technique however, was only based on 21 male and 25 female subjects, and relies on correctly identifying the functional occlusal plane, the orientation of which changes with growth or treatment.
What are the errors in cephalometry?
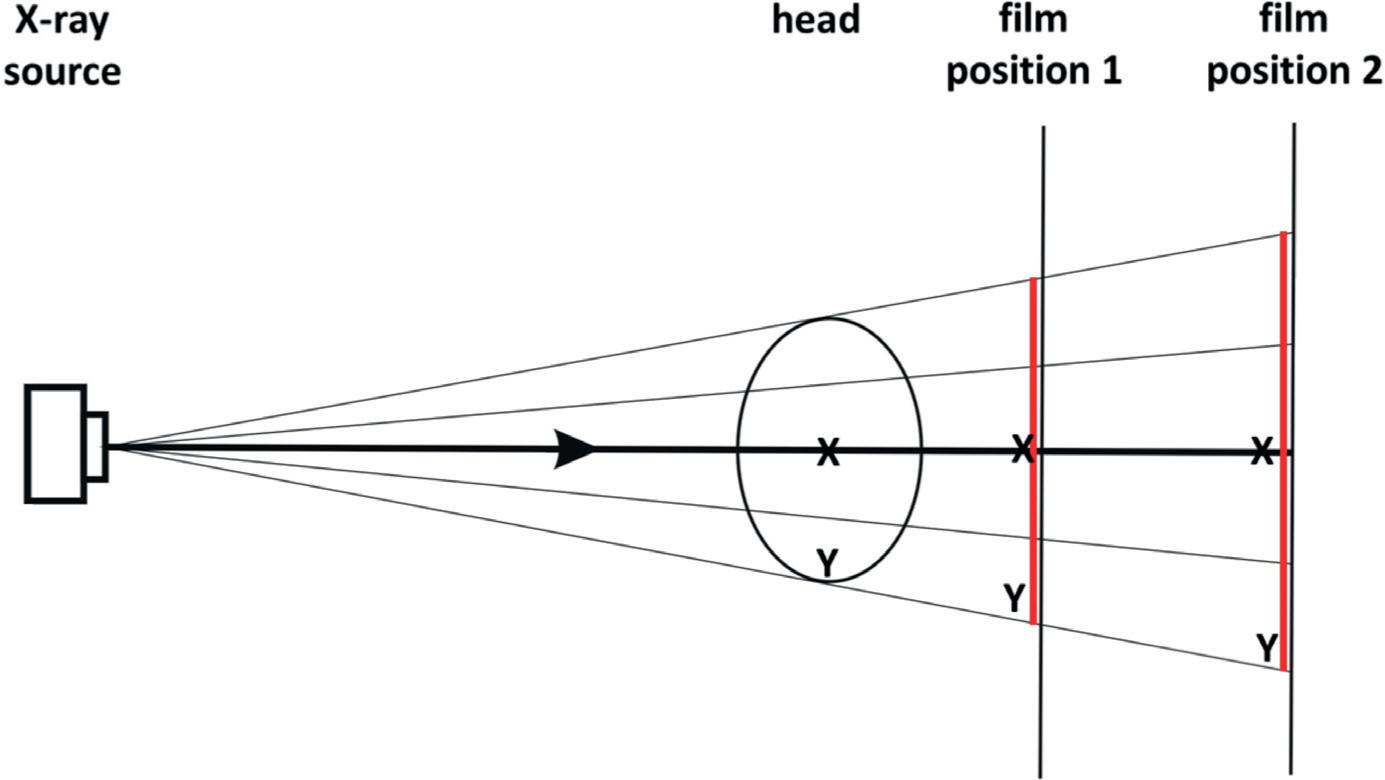
Considerable error can be associated with cephalometric measurements, with two general categories of error being described.16 The first category is errors of projection, relating to the radiograph being a 2D shadow of a 3D object, with non-parallel X-rays producing the shadow. These radiographs are always therefore distorted enlargements. The magnitude of the enlargement is related to distances between the focus of the X-ray beam, the head and the film. Objects close to the film and in the centre of the X-ray beam show the least magnification (Figure 2). As such, any change in orientation of the head away from natural head posture will lead to a corresponding distortion of the image.
Figure 2. Diagram of X-ray source, with beams diverging, showing two film positions and associated magnification. The magnitude of enlargement is related to the distance between the X-ray source, the head and the film. The film at position 2 shows greater magnification compared to position 1. The centre of the X-ray beam is associated with the least magnification. Structures at point Y are magnified more than structures at point X.
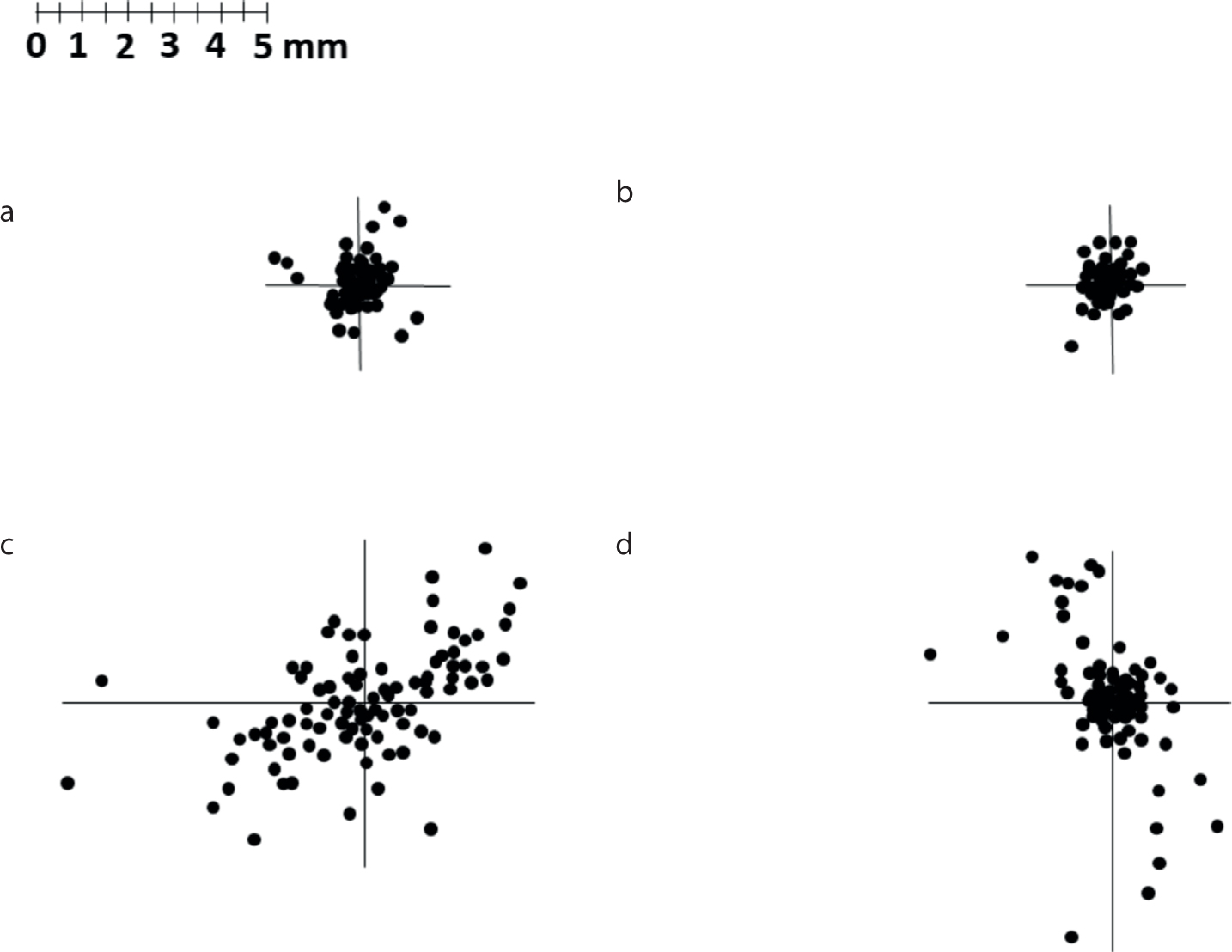
The second category is errors of identification. Landmark identification using points is associated with an ‘envelope of error’ (Figure 3). The magnitude of the error varies greatly from landmark to landmark and each landmark point has its own, usually non-circular, envelope of error. Sella has been identified as the most reliable point, because identification of the centre of a spherical shape is straightforward.17 Identifying the shallowest aspect of a gradual curve (eg A point or B point) is more prone to error compared to identifying an edge where two well-defined planes intersect (eg upper incisor edge)16 or a defined suture, for example the naso-frontal suture. In addition, the image resolution and contrast also affect point identification, as will X-ray image orientation.
Figure 3. Graphical representation of distribution of error for selected dental landmarks (redrawn from Baumrind and Frantz16). (a) Lower incisor edge. (b) Upper incisor edge. (c) Lower incisor apex. (d) Upper incisor apex.
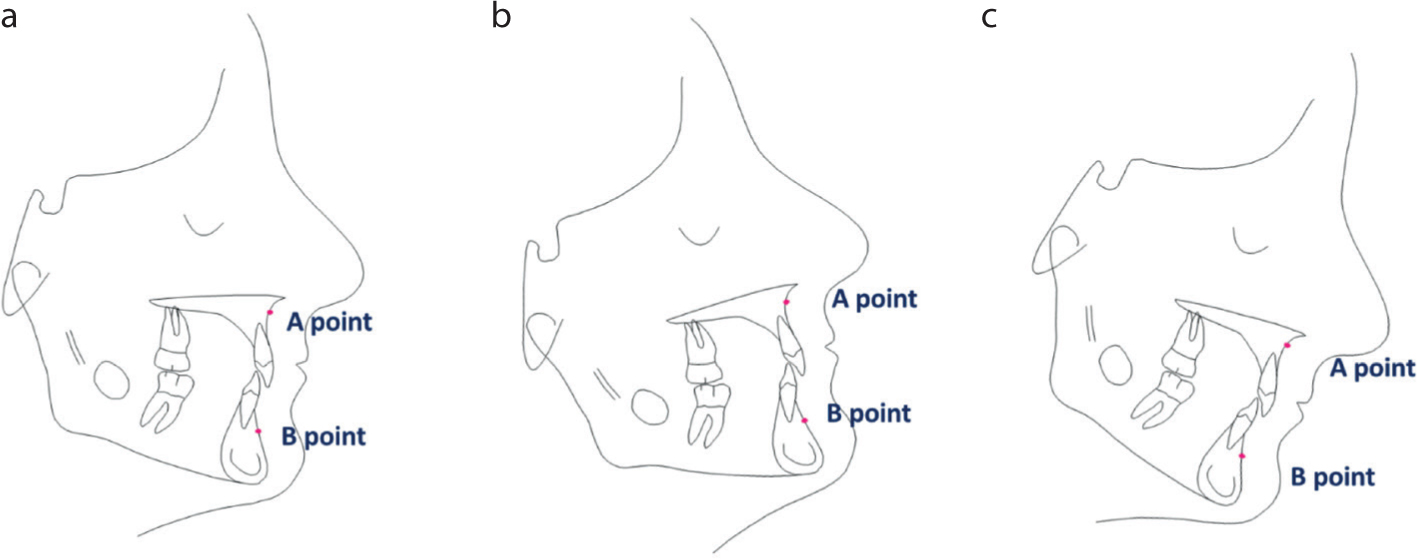
Angular and linear measurements are also necessarily affected by both projection and landmark identification errors. For linear measurements, the shorter the distance between two points, the greater the percentage error introduced by a measurement error of a given size. Different angular and linear measurements have different levels of reliability, and this is of critical importance in cephalometric superimposition. Baumrind and Frantz calculated that an observed ANB change of more than 1.12 degrees is required to be considered clinically significant, and not just the effect of error.18 As described in Figure 4, use of a horizontal reference plane is important.
Figure 4. The relative anteroposterior position of landmark points changes with alterations in head orientation. The anteroposterior position of A point in relation to B point changes as the orientation of the Frankfort plane alters, seemingly producing either a more Class 3 or more Class 2 skeletal pattern. This diagram shows the importance of a reproducible head position using a horizontal reference plane, such as the Frankfort plane.
The introduction and use of 3D cephalometry has increased in recent years, with techniques including CBCT,19 low-dose multi-slice CT or MRI. 3D imaging (Figure 5) may be particularly helpful for assessing facial asymmetry, due to better representation of the real morphology of the skull, unlike in traditional lateral cephalometry, where structures on the left and right are superimposed on each other.20 It is thought that 3D landmark identification and measurements are at least as reliable as traditional 2D cephalometric techniques.20
Figure 5. Cephalometric landmarks on CT-based 3D reconstruction. Co: left/right condylion (most superior point of condyle); Go: left/right gonion (midpoint on the curvature of the angle of the mandible); Po: left/right porion (most superior point of the external auditory meatus); Or: left/right orbitale (most inferior point on the infraorbital margin); Z: left/right zygion (most lateral point of the zygomatic arch); ANS: anterior nasal spine; PNS: posterior nasal spine; A: point A (point of maximum midline concavity on the maxilla); B: point B (point of maximum midline concavity on the mandibular symphysis); Pg: pogonion (most anterior point of mandibular symphysis); Me: menton (most inferior point of mandibular symphysis); Gn: gnathion (midpoint between Pg and Me); U1t: tip of the crown of the left/right first upper incisor; U1a: apex of the left/right first upper incisor; L1t: tip of the crown of the left/right first lower incisor; L1a: apex of the left/right first lower incisor.
Disadvantages of conventional radiography and CBCT include the radiation doses, which are often applied to young patients. In a child, the diagnostic reference levels (X-ray energy delivered to the patient) of a lateral cephalogram are about 34 times that of a typical peri-apical radiograph, whereas CBCT of an impacted maxillary canine is 230 times that of a typical peri-apical.21 MRI techniques, which do not use ionizing radiation, may provide a solution for the future. There is evidence that MRI (Figure 6) may provide good levels of diagnostic and therapeutic efficacy equivalent to traditional cephalometry, despite the fact that MRI is principally used in soft tissue diagnostics.22,23 Artefacts from metallic objects remain a limitation to this technique, which would be particularly relevant for mid-treatment cephalometric assessments.22 The lack of radiation associated with MRI would, however, facilitate justification of post-treatment imaging.
Figure 6. MRI sagittal section of the head. (Licence Link: https://commons.wikimedia.org/wiki/File:MRI_brain_sagittal_section.jpg (CC BY-SA 2.0). Author – deradian – A brain I has it (no changes made)).
To date, there is limited research-based evidence on the use of 3D cephalometry20 and, as with 2D techniques, true diagnostic efficacy is difficult to measure because it is impossible to check real landmark positions in patients. Since studies on patients can only describe ‘observer performance’ or ‘reliability of the methods’,20 cadaver studies or other in vitro methods might be used as an alternative means to identifying potential errors.
Prescription
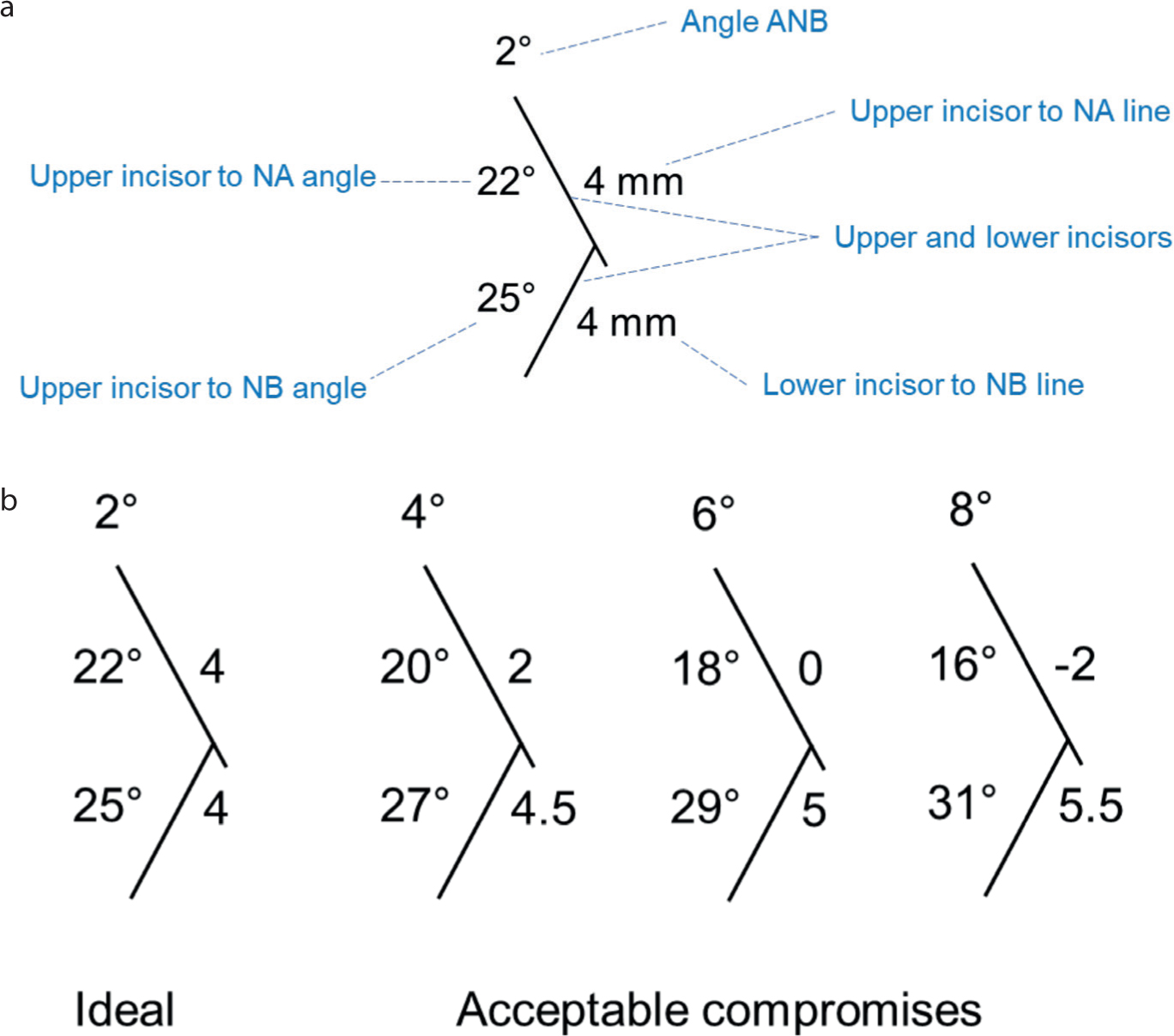
Assessment of skeletal pattern and inclinations of the labial segment teeth on lateral skull radiographs aids treatment planning and, therefore, prescription. Steiner proposed the use of cephalometrics as an adjunct to treatment planning, helping with extraction versus non-extraction decisions, choice of extractions, type of anchorage and in determining ‘acceptable compromises’ or camouflage (Figure 7).8
Figure 7. Steiner's sticks. (a) Average measurements used by Steiner for use for comparisons. (b) Steiner's acceptable compromises for the labial segment teeth in different skeletal patterns. This graphical representation became known as Steiner's sticks. Redrawn from Steiner.66
The lower incisor edge to upper incisor root centroid relationship can be analysed cephalometrically24 and has been identified as an important tool for diagnosis and treatment planning (Figure 8). It is a quick and straightforward technique for diagnosing all incisor relationships, but has a particularly important role in Class II cases. Stable overbite reduction can be planned by analysing the relationship of the lower incisor edge to upper incisor root centroid, informing decisions regarding the type of tooth movement required during treatment (eg tipping or bodily movement) or whether skeletal change is required.
Figure 8. Lower incisor edge–upper incisor root centroid relationship. The upper incisor root centroid to lower incisor edge relationship is the distance between the perpendicular projections of these points on to the maxillary plane. The distance is positive when the lower incisor edge is in front of the upper root centroid, and negative if behind. The distance should be at least +2 mm for maximum stability. (a) Maximum stability. (b) Favourable relationship, such that tipping only movements are required (eg URA treatment). (c) Less favourable relationship, but treatable by bodily movement with fixed appliances and retraction of upper labial segments and slight proclination of lower labial segment. (d) Unfavourable relationship, with lower incisor edge behind the upper root centroid. This relationship is only treatable with functional treatment or orthognathic surgery. Redrawn and adapted from Houston.24
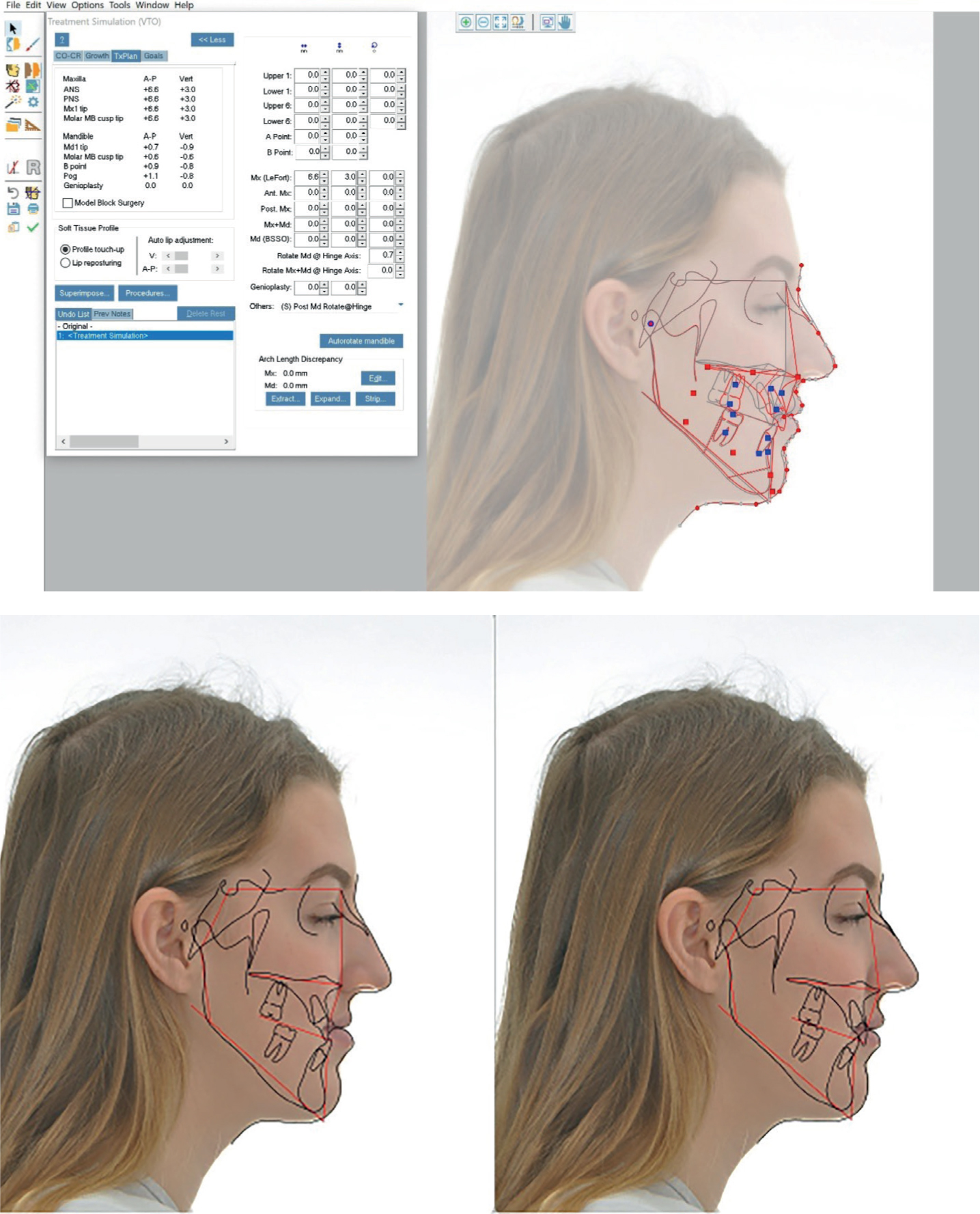
Cephalometric analysis of hard and soft tissue effects of joint orthodontic–surgical treatment is important for both the clinician and the patient when discussing treatment options and for informed consent. Planning techniques have evolved from manual manipulation of tracings and photographs to computerized prediction25 to the latest 3D-planning software and virtual surgical planning (Figure 9).26
Figure 9. Cephalometric surgical planning using Dolphin imaging.
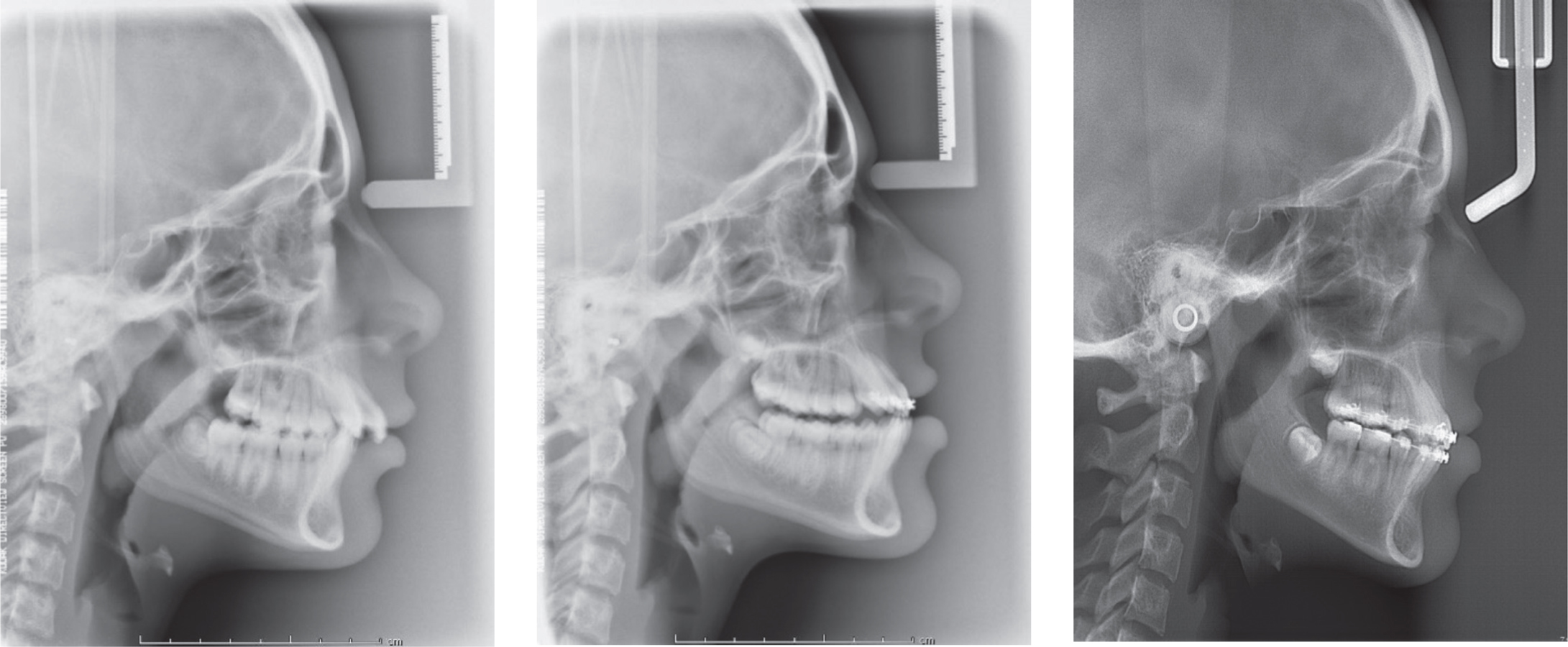
Mid-treatment cephalometric analysis is used to monitor treatment progress and to plan further treatment (Figure 10). For example, lateral cephalometry following a functional phase of treatment may facilitate planning for extractions, or assessment of inclination of the teeth during fixed appliance treatment may inform the retention protocol. For some ‘borderline’ cases, where the nature of the underlying problem is uncertain, therapeutic diagnosis may be employed, and the response to treatment is used to confirm or reject the original diagnosis.27
Figure 10. Pre-treatment, mid-treatment and near-end treatment cephalograms of the same patient. Note the changes in head orientation and the use of a difference machine for the near-end treatment cephalogram.
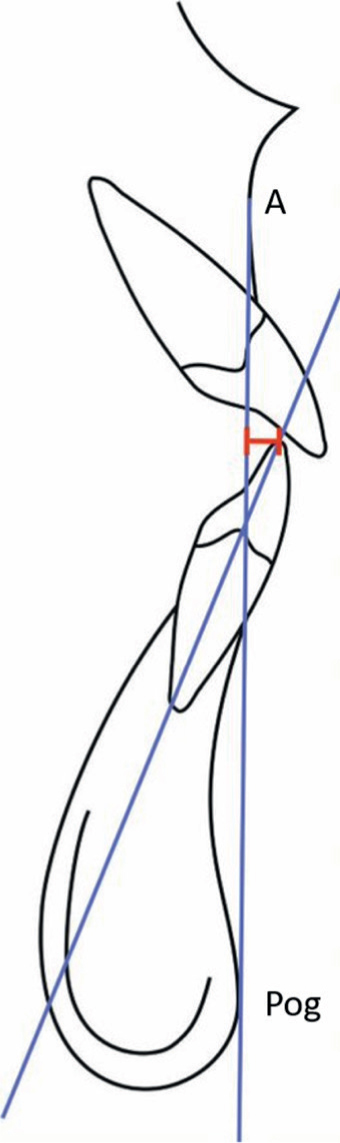
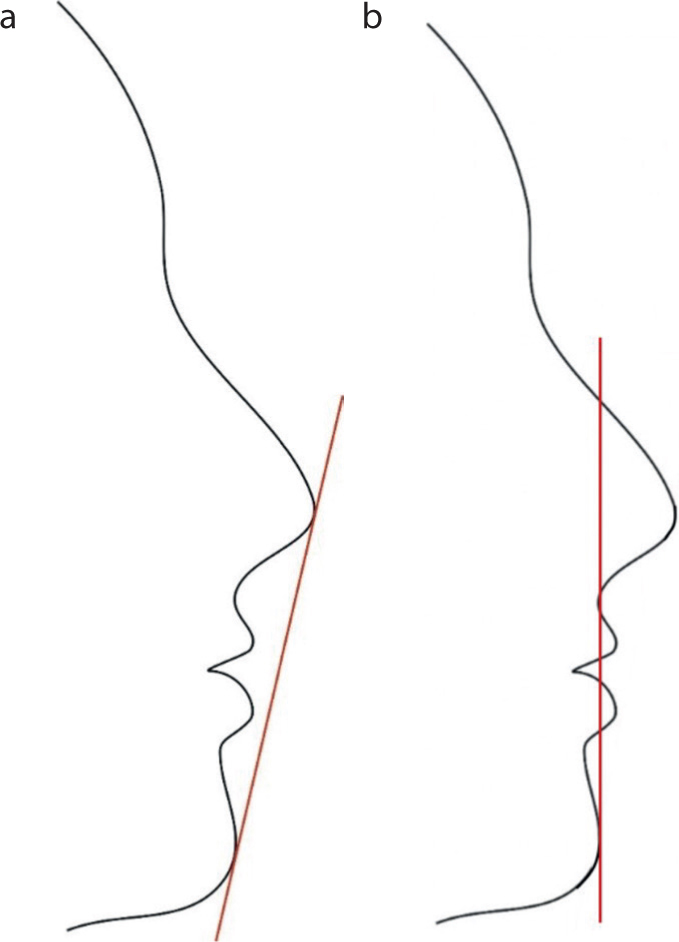
However, care must be used with some cephalometric analyses when prescribing orthodontic treatment. The importance of the relationship between the lower incisor edges to the A-Pog line (Figure 11) at the end of treatment for stability and appearance was advocated by Williams.28 The importance of this relationship was however rejected by Edler and Houston when the A-Pog line was not found to be a reliable guide to lower incisor stability.29 Ricketts' E-line (Figure 12) is an anterior reference line drawn from the tip of the nose to the chin point used to assess lip fullness.30 Although convenient, other planes to assess soft tissue profile may show better consistency and sensitivity, such as Burstone's B-line, a reference line bisecting the nose, drawn from soft tissue sub-nasale to soft tissue pogonion (Figure 12).31
Figure 11. The A-Pog line. The distance between the tip of the lower incisor and the A-Pog line is measured in millimetres (shown in red).Figure 12.
(a) Ricketts' E-line is drawn from the tip of the nose to soft tissue pogonion and is shown in red. Ideally, the upper lip is positioned 4 mm behind this line and the lower lip 2 mm behind. (b) Burstone's B-line is drawn from the soft tissue subnasale to the soft tissue pogonion and is shown in red. Ideally, the upper lip is positioned 3.5 mm in front of this line and lower lip 2.2 mm in front.
Prediction
It would be useful to be able to predict facial growth, both its timing and direction, particularly in the case of Class 2 and Class 3 skeletal patterns. Being able to predict the timing of facial growth would be beneficial, not only in terms of the correction of anteroposterior skeletal relationships, but also in the management of deep overbites and rate of tooth movement.32 Previously, serial cephalometric radiographs have been used to analyse the changes that occur during facial growth.33 These include the following studies.
The Michigan growth study
This study started in 1935 and lateral cephalograms of subjects were taken routinely until about 1970. The study resulted in publication of an atlas of craniofacial growth with cephalometric standards.34
The Burlington growth study
This project started in the Canadian town of Burlington in 1952 and 1258 children were enrolled, which represented nearly 90% of the children within the specified ages required. The population of the town in 1952 was 9000. For the serial experimental sample, six lateral cephalograms and one hand–wrist radiograph were taken between the ages of 3 and 21 years.35
The Bolton–Brush study
The collection contains data from around 6000 research subjects from two large studies (Bolton and Brush). The Bolton study was initiated by B. Holly Broadbent Sr (the father of modern cephalometry) in the 1920s and comprised annual cephalometric radiographs, alongside numerous other records, of subjects throughout babyhood, childhood and adolescence. Data continued to be gathered until 1959.36 The Brush inquiry ceased in 1942 and included 250,000 radiographs of 4000 children. More recent recalls of participants from these studies have confirmed that craniofacial growth continues throughout adulthood.37 More than 100 individuals were recalled in the early 1980s for new radiographs. There were increases in all of the facial dimensions, but vertical changes were the most prominent. Growth rotations of the jaws also continued into adult life.
These growth studies, and others, provide a wealth of data allowing treatment comparisons with untreated controls, matched for age and gender.38 It is highly unlikely that ethical approval would be obtained today for similar large-scale studies with repeated radiographs of healthy subjects.
Bjorks' structural signs
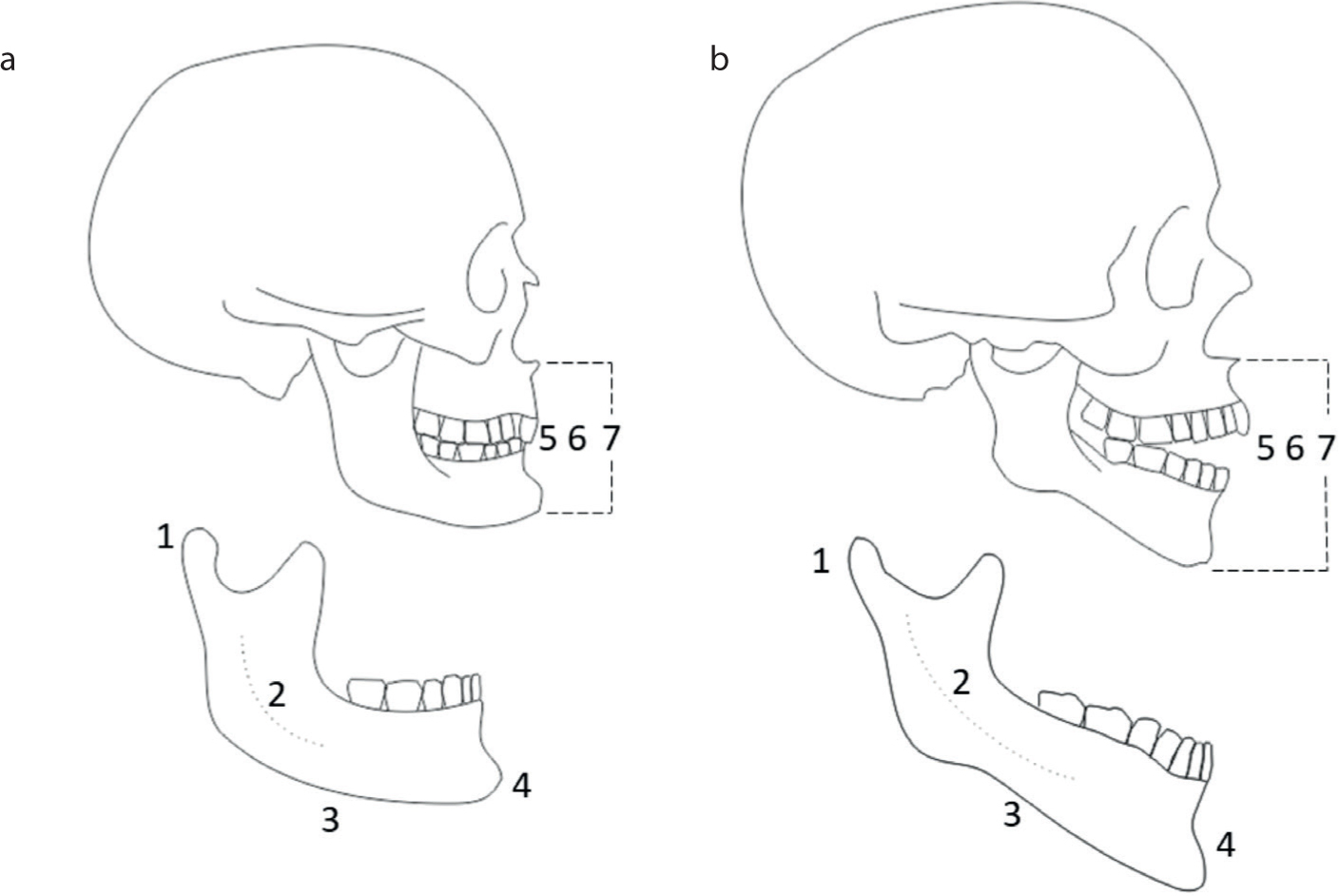
In the 1960s, Björk performed experiments whereby tantalum implants, measuring 1.5 mm in length and 0.5 mm in diameter, were placed subperiosteally to serve as fixed reference points in serial lateral cephalograms.39 Using this technique, Björk reported on seven signs visible on a lateral cephalogram (Figure 13) that can be used to help predict the direction of mandibular growth with particular reference to growth rotations.40 Forward rotation was found to be more common than backward rotation. Predicting the growth pattern prior to treatment may be very helpful. Extreme rotation may influence the path of eruption of teeth.40 In addition, Class II functional treatment of hyperdivergent patients may be more challenging than hypodivergent, as the backwards growth rotation may displace the chin downwards and backwards, negating the effects of the functional appliance.41 Unfortunately, evidence suggests that hypo- or hyperdivergent morphology cannot be reliably detected using Björk's structural signs of mandibular growth rotation. Although subjects with the extremes of hypo- or hyperdivergency were all correctly identified using this method in a study in 2005, no statistical association was found between the structural signs and type of growth rotation.42
Figure 13. Björk's structural signs of mandibular growth rotation. (a) Anterior growth rotation. (b) Posterior growth rotation. 1: inclination of the condylar head; 2: curvature of the mandibular canal; 3: shape of the lower border of the mandible; 4: inclination of the symphysis; 5: interincisal angle; 6: intermolar angle; 7: anterior lower face height.
Cervical vertebral maturation
More recently, lateral cephalograms have been used to assess the timing of growth by measuring maturity of the cervical vertebrae (Figure 14). This method, first described by Lamparski43 and later refined by Baccetti, enables prediction of peak mandibular growth through analysis of the vertebrae C2, C3 and C4.44 This cervical vertebral maturation (CVM) technique has found favour over other radiographic methods, such as hand–wrist radiographs, because lateral cephalograms are already commonly prescribed in orthodontics and hence, radiation doses are limited. Hand–wrist radiograph assessment of skeletal maturity is the gold standard, but the CVM method is said to show a high level of correlation with hand–wrist radiographs,45 and is both reproducible and reliable.46 Some authors, however, have recently challenged the reported reliability of the CVM method,47,48,49 suggesting reproducibility is poor and that additional biological indicators need to be used. This is likely to be due to the subjectivity associated with assessment of shape changes.
Figure 14. The CVM method. The morphology of three cervical vertebrae (C2, C3, C4) is evaluated on lateral cephalograms. The CVM method can be used to detect optimal timing to start functional appliance treatment. CS1: the peak in mandibular growth will occur on average 2 years after this stage; CS2: the peak in mandibular growth will occur on average 1 year after this stage; CS3: the peak in mandibular growth will occur during the year after this stage; CS4: the peak in mandibular growth has occurred within 1 or 2 years before this stage; CS5: the peak in mandibular growth has ended at least 1 year before this stage; CS6: the peak in mandibular growth has ended at least 2 years before this stage. Redrawn from Baccetti et al.44
Research
Cephalometric analysis is a frequently applied technique for quantitative research in orthodontics. One of the first major studies on the growth of the human head was reported by Brodie in 1941, using serial lateral cephalograms on children from the Bolton and Brush studies.50 The morphogenetic pattern of the human skull was found to be established at an early age and did not change once attained. Björk's studies contributed greatly to the understanding of rotations and remodelling in relation to growth.51 Modern principles of minimizing radiation exposure have resulted in more stringent scrutiny of research protocols.
Cephalometric data from well-known growth studies (eg Bolton36 and Burlington52) are often used as control group data in research studies. Bias (deflation of treatment effects) is associated with studies where historical control groups are used. Papageiorgiou et al. compared trials including concurrent controls with those including historical controls and found that the design of the control group influenced the results, independently of the design of the intervention group.53 Studies with historical controls showed smaller treatment effects compared to studies with concurrent controls. As such, concurrent untreated controls or ‘active’ control groups, where patients receive a ‘standard of care’ treatment are advised.53
The impact of secular trends associated with cephalometric dimensions derived from historical growth studies was highlighted by Antoun et al.54 For example, over the 20th century, mandibular length increased, whereas height and breadth decreased.55 This is another reason why caution is required when interpreting results from clinical trials comparing treatment effects in contemporary patients to cephalometric measurements from historical growth studies.54
As previously discussed, many of the available cephalometric analyses have poor scientific justification and errors of both projection and landmark identification affect the validity of research findings. There has been a recent increase in qualitative orthodontic research in the UK.56 Attempts are currently underway to define a core outcome set for orthodontic trials,57 which is likely to place much less emphasis on cephalometric outcomes and more emphasis on outcomes important to the patient.
Do we still need lateral cephs?
Lateral cephalograms are still justified for a range of clinical or research purposes. Treatment plans from a group of 16 orthodontists changed significantly when a lateral cephalogram became available, particularly for bimaxillary protrusion and Class II division 2 cases. The number of non-extraction treatment plans reduced significantly when a cephalogram was provided for bimaxillary protrusion patients, whereas for Class II division 2 patients, information from the cephalogram reduced the number of extractions prescribed by about half. The assessment of severity of a case changed significantly when a lateral cephalogram was available.58
Several other reports, however, have shown that cephalometrics may have no influence or only minor influence on treatment decisions. 59,60 A group of orthodontists in Boston, USA, found that patients with a Class I malocclusion without skeletal discrepancies, such as open bites or crossbites, can be diagnosed and planned without a cephalometric radiograph.61 Study models alone were considered adequate for treatment planning for 55% of a group of Class II division 1 cases.62 A systematic review from 2013 reported that there is limited scientific evidence to support the use of lateral cephalometric radiographs in orthodontic treatment planning.63 A second systematic review, also published in 2013, similarly reported that there are few high-quality studies regarding which records are required for treatment planning, but that lateral cephalograms may not be routinely needed for Class II malocclusions.64
In teaching environments, it may be argued that there is a benefit to orthodontic trainees of taking pre- and mid-treatment cephalograms to analyse treatment changes. There is also evidence that orthodontic educators order more radiographs than practitioners.65 Lateral cephalometric radiographs at the end of treatment following removal of active appliances are unlikely to be indicated in the majority of cases.6 There may be rare instances where radiographs may be justified, such as in the assessment of relapse, where the aetiology of the relapse needs to be identified, and plans for re-treatment are required. The ALARP principle should always be followed and where possible, radiation-free techniques considered.
Conclusion
Cephalometry has roles in diagnosis, prescription, prediction and research. It remains an important element of the orthodontic diagnostic armoury for selected cases and can inform treatment planning decisions in a wide range of camouflage and surgical cases. Efforts to limit radiation dose will encourage use of alternative techniques, such as MRI, in the future. Although associated with some limitations, the CVM method may aid the timing of orthodontic treatment where synchronization with the pubertal growth spurt is helpful. The large growth studies of the past provide a wealth of data regarding untreated controls, but limitations are associated with their use as control data in modern studies. It is likely that the role of cephalometry will reduce in orthodontic research as patient-centred research becomes more common.