Todd JE, Dodd T Children's Dental Health in the United Kingdom, 1983: A Survey Carried out by the Social Survey Division of OPCS, on Behalf of the United Kingdom Health Departments, in Collaboration with the Dental Schools of the Universities of Birmingham and Newcastle.London: HMSO; 1985
Thiruvenkatachari B, Harrison JE, Worthington HV, O'Brien KD Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children. Cochrane Database Syst Rev. 2013; 11 https://doi.org/10.1002/14651858.cd003452.pub3
McNamara JA Components of class II malocclusion in children 8–10 years of age. Angle Orthod. 1981; 51:177-202
Luca L, Francesca C, Daniela G Cephalometric analysis of dental and skeletal effects of Carriere Motion 3D appliance for Class II malocclusion. Am J Orthod Dentofacial Orthop. 2022; 161:659-665 https://doi.org/10.1016/j.ajodo.2020.12.024
Clermont A, Albert A, Bruwier A Effects of the Class II Carriere motion appliance in phase I treatment: a randomized controlled trial. J Clin Orthod. 2022; 56:285-293
Benson PE, Tinsley D, O'Dwyer JJ Midpalatal implants vs headgear for orthodontic anchorage – a randomized clinical trial: cephalometric results. Am J Orthod Dentofacial Orthop. 2007; 132:606-615 https://doi.org/10.1016/j.ajodo.2006.01.040
Barakat D, Bakdach WMM, Youssef M Treatment effects of Carriere motion appliance on patients with class II malocclusion: a systematic review and meta-analysis. Int Orthod. 2021; 19:353-364 https://doi.org/10.1016/j.ortho.2021.05.005
Carrière L A new Class II distalizer. J Clin Orthod. 2004; 38:224-231
Wilson B, Konstantoni N, Kim KB Three-dimensional cone-beam computed tomography comparison of shorty and standard Class II Carriere motion appliance. Angle Orthod. 2021; 91:423-432 https://doi.org/10.2319/041320-295.1
Kim-Berman H, McNamara JA, Lints JP Treatment effects of the Carriere motion 3D appliance for the correction of Class II malocclusion in adolescents. Angle Orthod. 2019; 89:839-846 https://doi.org/10.2319/121418-872.1
Yin K, Han E, Guo J Evaluating the treatment effectiveness and efficiency of Carriere Distalizer: a cephalometric and study model comparison of Class II appliances. Prog Orthod. 2019; 20 https://doi.org/10.1186/s40510-019-0280-2
Sandifer CL, English JD, Colville CD Treatment effects of the Carrière distalizer using lingual arch and full fixed appliances. J World Fed Orthod. 2014; 3:e49-e54
Biggs EV, Benavides E, McNamara JA Three-dimensional evaluation of the carriere motion 3D appliance in the treatment of Class II malocclusion. Am J Orthod Dentofacial Orthop. 2023; 164:824-836 https://doi.org/10.1016/j.ajodo.2023.05.031
Lombardo L, Cremonini F, Oliverio T Class II correction with carriere motion 3D appliance and clear aligner therapy. J Clin Orthod. 2022; 56:187-193
Areepong D, Kim KB, Oliver DR, Ueno H The Class II Carriere motion appliance. Angle Orthod. 2020; 90:491-499 https://doi.org/10.2319/080919-523.1
Zymperdikas VF, Koretsi V, Papageorgiou SN, Papadopoulos MA Treatment effects of fixed functional appliances in patients with Class II malocclusion: a systematic review and meta-analysis. Eur J Orthod. 2016; 38:113-126 https://doi.org/10.1093/ejo/cjv034
Pancherz H Treatment of class II malocclusions by jumping the bite with the Herbst appliance. A cephalometric investigation. Am J Orthod. 1979; 76:423-442 https://doi.org/10.1016/0002-9416(79)90227-6
Jones G, Buschang PH, Kim KB, Oliver DR Class II non-extraction patients treated with the forsus fatigue resistant device versus intermaxillary elastics. Angle Orthod. 2008; 78:332-338 https://doi.org/10.2319/030607-115.1
Franchi L, Alvetro L, Giuntini V Effectiveness of comprehensive fixed appliance treatment used with the forsus fatigue resistant device in Class II patients. Angle Orthod. 2011; 81:678-683 https://doi.org/10.2319/102710-629.1
Antonarakis GS, Kiliaridis S Maxillary molar distalization with noncompliance intramaxillary appliances in Class II malocclusion. A systematic review. Angle Orthod. 2008; 78:1133-1140 https://doi.org/10.2319/101507-406.1
Class II malocclusion is a relatively common orthodontic presentation. Management can include various approaches depending on the severity of the malocclusion, the patient's age, wishes, expectations and the clinician's experience. As well as the increased overjet commonly seen in Class II malocclusion, the overbite usually, but not always, is increased. Managing and controlling both the anteroposterior and vertical elements of the malocclusion simultaneously can be very efficient and lead to a reduced overall treatment duration. The Carriere Class II 3D motion appliance (CMA) is a relatively new concept in managing Class II malocclusion. The simple design makes CMAs more comfortable than other appliances. The distal force on the posterior maxillary segment is applied by elastics, worn from the anterior hook to a button or hook on the mandibular first molar. The protocol for mandibular anchorage includes the use of a removable Essix-type clear retainer that has been modified posteriorly to accommodate the bonded buccal tubes or hooks on the mandibular molars. This article presents two cases where patients were concurrently treated with CMA and lower fixed appliances.
CPD/Clinical Relevance: Correction of Class II malocclusion can be made more efficient if both the anteroposterior and vertical components are addressed simultaneously.
Article
Class II malocclusion is a relatively common orthodontic presentation. Despite its prevalence, the management of Class II malocclusion has always represented a challenge.1,2 The aetiology of Class II malocclusion can be multifactorial in nature and is most likely due to a combination of several dento-alveolar and skeletal factors, among which the most common is mandibular retrognathia.3,4 Correct diagnosis and identification of the cause of Class II and any other vertical component to the malocclusion is paramount for adequate treatment.3,4
Several options can be used to correct an increased overjet. However, the management approach for Class II malocclusion depends on several factors, including, but not limited to: the patient's age, preferences and compliance; the aetiology of the malocclusion; and the clinician's experience and preferences.5 Most Class II malocclusions are efficiently treated in the late-mixed dentition using various methods, including headgear, distalizers, functional appliances, premolar extractions and fixed appliances with Class II intermaxillary elastics. Molar distalization is one approach for treating Class II malocclusion,6,7 especially when functional appliances are not thought to produce the desired correction owing to suboptimal compliance or older age. Depending on the type of discrepancy, orthognathic surgery may also be indicated.
In 2004, the Carriere motion appliance (CMA) was introduced by Dr Luis Carriere.8 The appliance was manufactured and designed to correct Class II occlusion by correcting the molar relationships at the start of treatment. The CMA has become more popular during the past decade as a versatile intermaxillary Class II corrector. The clinical principle of Class II correction using the CMA is based on establishing a Class I relationship at the beginning of treatment when patient compliance is high and before initiating the correction of the position and alignment of individual teeth with fixed appliances (or clear aligner therapy).
The CMA is a device that consists of an arm, a pad to be cemented to either the canine or the first premolar in the maxillary arch, equipped with a hook for applying an elastic, and another pad to be cemented to the maxillary first molar.4,8 The molar pad features a ball and socket-type structure that allows de-rotation of the maxillary first molar while contr olling its inclination during the correction of the posterior teeth as a single unit. The mandibular anchorage is enhanced by the use of a vacuum-formed retainer. However, various methods can be used to control the proclination of the mandibular incisors, including lingual holding arch or temporary anchorage devices.
This article introduces the concept of concurrent use of the CMA with lower labial multi-bracketed fixed appliances, and presents and discusses cases treated with this treatment modality.
Case 1
History
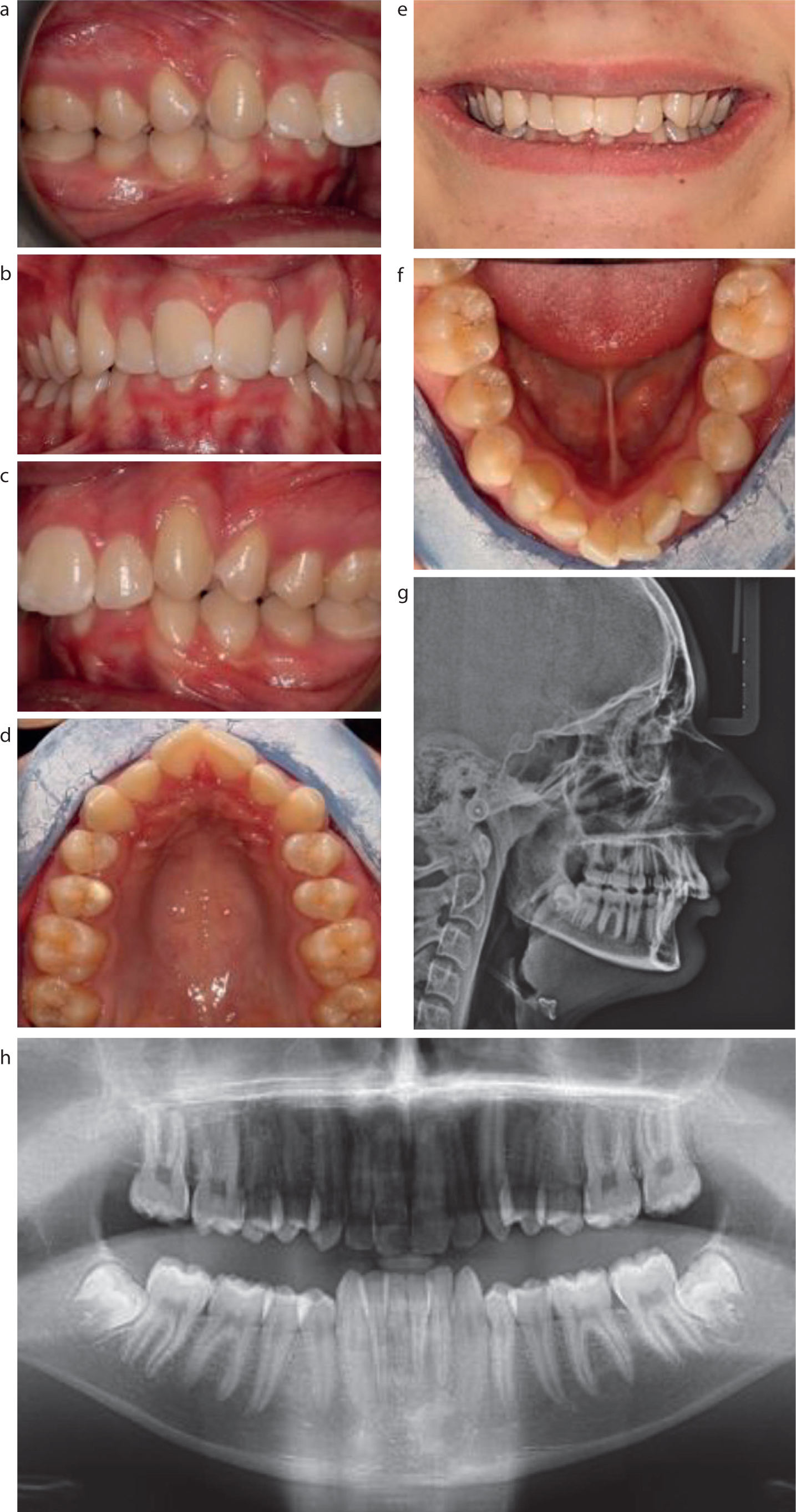
A male patient aged 16 years 4 months presented with a chief complaint of ‘upper teeth stick out’. The medical and dental histories were non-contributory. The patient had not had previous orthodontic treatment (Figure 1).
Figure 1. (a–h) Case 1: A 16-year-old male patient presented in the permanent dentition with a Class II division 1 incisor relationship, overjet of 10 mm, deep overbite, ¾ unit Class II molar and canine on the right, ½ unit Class II molar and canine on the left, V-shaped arches and crowding.
Extra-oral assessment
The patient showed a convex profile with a moderate skeletal II pattern and reduced lower anterior face height. There was no obvious facial asymmetry. The lips were potentially competent at rest, and the lower lip trapped behind the upper incisors. The maxillary midline was 2 mm to the left of the facial midline, while the mandibular midline coincided with the midpoint of the chin and the facial midline (Figure 1).
Intra-oral assessment
The patient presented in the permanent dentition and displayed a Class II division 1 incisor relationship. The malocclusion was complicated by an increased overjet (OJ = 10 mm), increased overbite, which was complete and atraumatic, molar and canine relationships of ¾ unit Class II on the right and ½ unit Class II on the left, dental crowding, maxillary dental centreline deviation by 2 mm to the left and narrow V-shaped dental arches (Figure 1). The maxillary canines were distally angulated (indicating dento-alveolar compensation in the sagittal plane) and the mandibular canines were upright.
Radiographic assessment
A lateral cephalogram radiograph was obtained under standardized conditions. Cephalometric analysis revealed a Class II skeletal relationship owing to mandibular retrognathia in relation to the cranial base and maxilla, as reflected by the increased Wits appraisal and a reduced SNB angle (Table 1). The lower anterior face height and the angle of the maxillary–mandibular planes were slightly reduced, although, within normal limits. The upper and lower incisor inclination was average (Table 1).
Case 1
Case 2
Cephalometric measurement
Pre-treatment
Post-treatment
Pre-treatment
Post-treatment
Norm
Anterio-posterior
SNA (°)
81
81
80
80
82 ± 3
SNB (°)
76
77
75
75
79 ± 3
ANB (°)
5
4
5
5
2 ± 2
Wits (mm)
11
9
7
6
0 ± 1
Vertical
Mx–Mn planes angle (°)
26
29
25
27
27 ± 4
S-N/Mn planes angle (°)
31
33
32
34
35 ± 4
S-N/Mx planes angle (°)
5
5
7
7
8 ± 3
Upper anterior face height (mm)
56
56
55
55
55 ± 3
Lower anterior face height (mm)
60
63
59
60
66 ± 3
Anterior face height ratio (%)
52
53
52
53
56 ± 4
Dento-alveolar
Upper incisor/Mx plane (°)
110
108
105
110
109 ± 6
Lower incisor/Mn plane (°)
93
99
88
94
90 ± 6
Interincisal angle (°)
130
120
120
125
121 ± 10
Incisor overjet (mm)
10
2
6
2
2 ± 1
Lower incisor tip/APg (mm)
-1.5
-0.5
-2
-1
2 ± 2
Soft tissues
ULip–E Plane (mm)
-4
-5
-2
0
-3 ± 2
LLip–E Plane (mm)
-2.5
-2
-2
0
-2 ± 2
Naso-labial angle (°)
146
145
90
90
110 ± 5
An orthopantomogram was obtained under standardized conditions. The panoramic radiograph demonstrated the presence of all permanent teeth except for the maxillary third molars. The bone levels were normal, the roots were of normal length, and there was no evidence of pathology.
Aetiology
The Class II and increased overjet resulted from the underlying skeletal II pattern caused by mandibular retrognathia. The increased overbite was due to the reduced lower face height and maxillary mandibular plane angle. The lower lip trap was a result of the increased overjet caused by the Class II sagittal relationship. The narrow maxillary arch was due to the dento-alveolar compensation in the transverse plane caused by an apparent narrow lower arch owing to the skeletal II sagittal relationship.
Treatment aims and rationale
The aims of treatment were to:
Correct the Class II molar and canine relationships to Class I;
Relieve crowding;
Reduce and normalize the overjet;
Reduce and normalize the overbite;
Establish a Class I incisor relationship;
Correct the centrelines and co-ordinate arches.
Case 2
History
A female patient aged 15 years 6 months presented with a chief complaint of ‘deep bite’. The medical and dental histories were non-contributory. The patient had not had previous orthodontic treatment (Figure 2).
Figure 2. (a–h) Case 2: A 15-year-old female patient presented in the permanent dentition with Class II division 2 incisor relationship, overjet of 6 mm, deep overbite, ¾ unit Class II molar and canine on the right, ½ unit Class II molar and canine on the left and mild crowding.
Extra-oral assessment
The patient showed a convex profile with a moderate skeletal II pattern and reduced lower anterior face height. There was no obvious facial asymmetry. The lips were potentially competent at rest, and the lower lip trapped behind the upper incisors. (Figure 2).
Intra-oral assessment
The patient presented in the permanent dentition and displayed a Class II division II incisor relationship. The malocclusion was complicated by an increased overjet (OJ = 6 mm), increased overbite, which was complete and atraumatic, ¾ unit Class II molar and canine relationship on the right, ½ unit Class II molar and canine relationship on the left and dental crowding (Figure 2).
Radiographic assessment
A lateral cephalogram radiograph was obtained under standardized conditions. Cephalometric analysis revealed a Class II skeletal relationship owing to mandibular retrognathia in relation to the cranial base and maxilla, as reflected by the increased Wits appraisal and a reduced SNB angle (Table 1). The lower anterior face height and maxillary–mandibular plane angle were slightly reduced, although within normal limits. The upper and lower incisor inclinations were average (Table 1).
An orthopantomogram was obtained under standardized conditions. The panoramic radiograph demonstrated the presence of all permanent teeth. The bone levels were normal. The roots were of normal length, and there was no evidence of pathology.
Aetiology
The Class II and increased overjet resulted from the underlying skeletal II pattern caused by mandibular retrognathia. The increased overbite was due to the reduced lower face height and maxillary mandibular plane angle. The lower lip trap resulted from the increased overjet caused by the Class II sagittal relationship. The narrow maxillary arch was a result of the dento-alveolar compensation in the transverse plane caused by an apparent narrow lower arch due to the skeletal II sagittal relationship.
Treatment aims and rationale
The aims of treatment were to:
Correct the Class II molar and canine relationships to Class I;
Relieve crowding;
Reduce and normalize the overjet;
Reduce and normalize the overbite;
Establish a Class I incisor relationship and co-ordinate arches.
Treatment options for Cases 1 and 2
The options for correcting the Class II relationship presented to the patient were:
Accept the malocclusion;
Manage with removable functional appliances;
Class II correction with fixed Class II correctors;
Carriere motion appliance followed by fixed appliances;
Distalization of the maxillary arch with the aid of skeletal anchorage;
Extraction of two maxillary premolars and attempt camouflage;
Orthognathic surgery.
The shared decision reached for both patients was the Carriere motion appliance, followed by fixed appliances with the view of revising the treatment plan and potentially considering distalization of the maxillary arch with the aid of skeletal anchorage and extraction of two maxillary premolars and attempt camouflage.
With regards to managing the overbite, considerations were given to various options, including using anterior bite turbos, adding reverse curve of Spee in the lower archwire, and using Class II intermaxillary elastics, among others. A shared decision was made to manage initially with intermaxillary elastics and levelling the mandibular curve of Spee before resorting to other options.
Treatment plan and progress for Cases 1 and 2
The plan aimed to correct the sagittal and vertical elements of the malocclusion simultaneously and involved concurrently fixing lower arch appliances and A CMA (Figure 2). The lower arch was bonded with pre-adjusted edgewise appliances (0.022” x 0.028” slot size) with MBT prescription and self-ligating bracket design.
The mandibular second molars were bonded from the outset to help provide vertical control to level the deep mandibular curve of Spee. The archwire was cinched back to prevent excess lower incisor proclination in an attempt to control the lower arch length.
MBT bracket prescription was preferred owing to the beneficial lingual crown torque prescription, which is important in controlling lower incisor inclination and counteracting uncontrolled proclination induced by the Class II elastics.
The initial alignment archwire (0.14” NiTi) was ligated for one visit. This progressed to 0.016” x 0.022” NiTi archwire on visit 2, 0.019” x 0.025” NiTi archwire on visit 3 and 0.019” x 0.025” SS archwire on the forth visit. The appointment intervals were approximately 6 weeks.
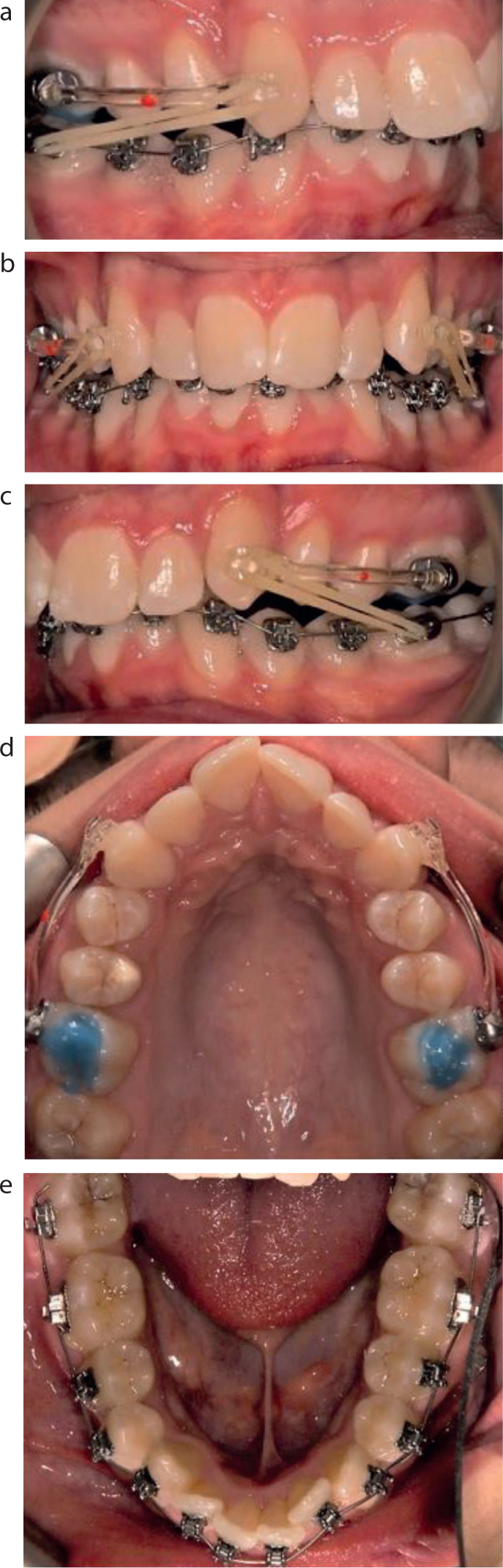
The CMA was placed after selecting the optimal canine–molar arm length (Figure 3). At the first visit, the patient was instructed to wear force 1 elastics (6 oz, 1/4”) on a full-time basis for 3 months. This was followed by force 2 elastics (8 oz, 3/16”) for a further 3 months. The total duration of active Class II correction with The CMA was 6 months.
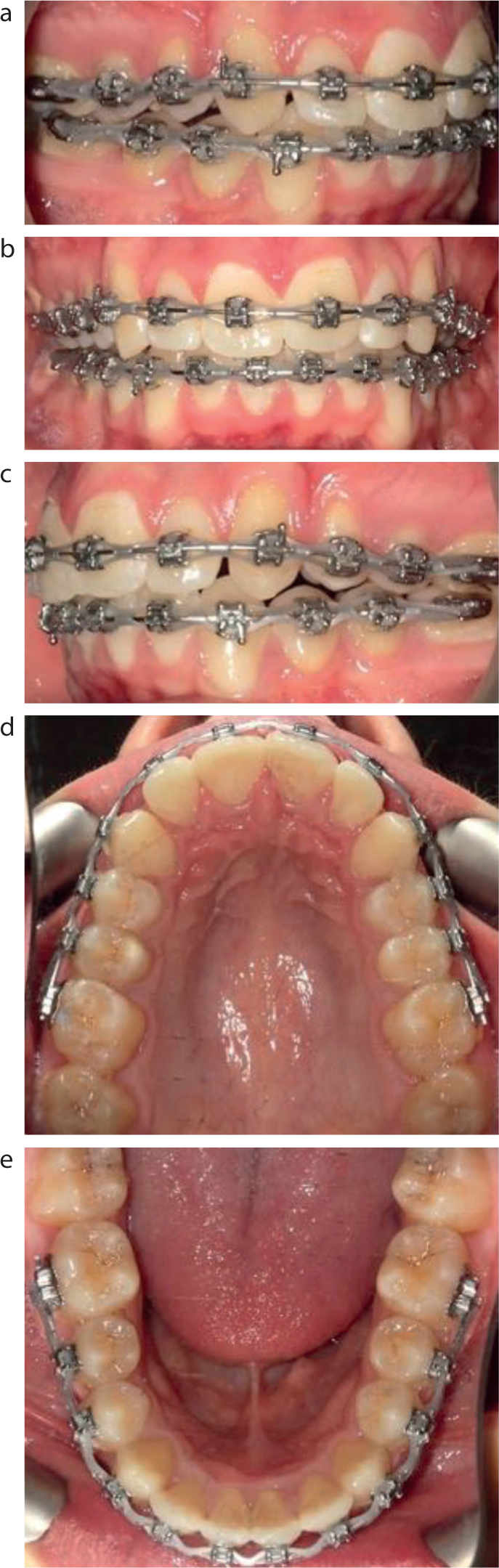
Figure 3. (a–e) Case 1: Treatment commenced by bonding the lower arch and fitting the Carriere motion appliance. Force 1 elastics (6 oz, 1/4”) were used for 3 months, followed by force 2 elastics (8 oz, 3/16”) for a further 3 months. The total duration for active distalization was 6 months.
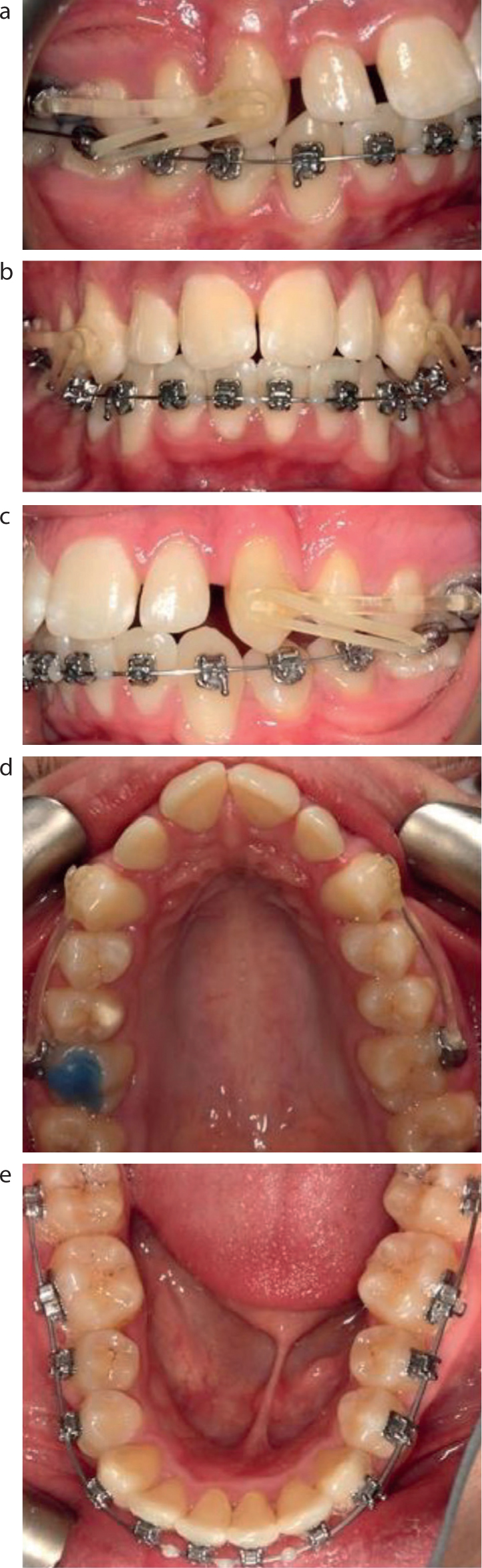
After 6 months of treatment, full sagittal correction was achieved (Class I canine relationships), the CMA was removed, and the upper arch was bonded with pre-adjusted edgewise appliances (0.022” x 0.028” slot size) with MBT prescription and self-ligating bracket design (Figures 4 and 5).
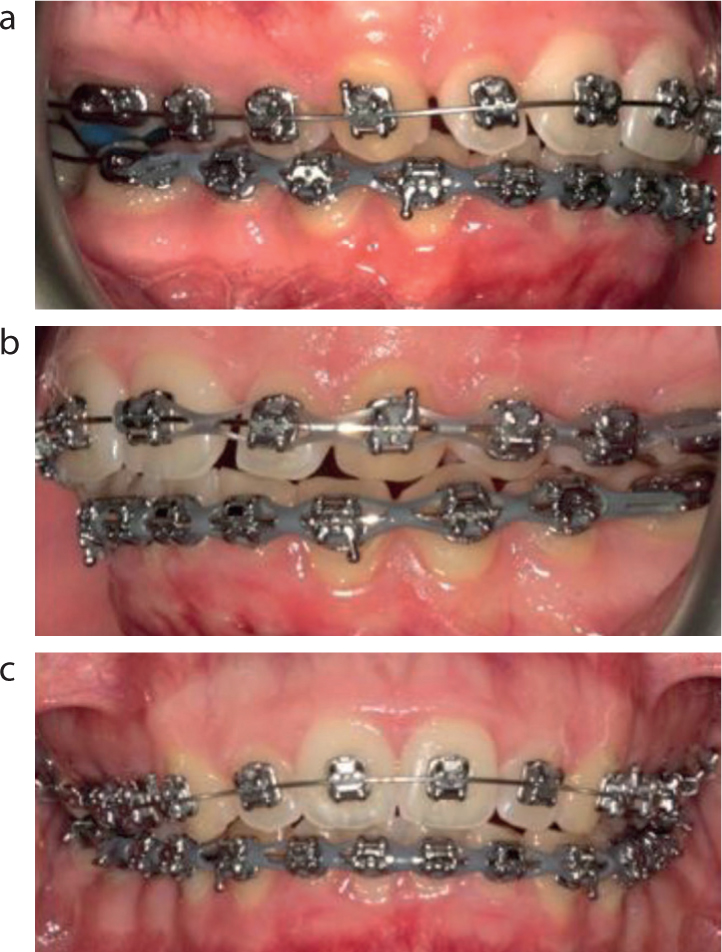
Figure 4. (a–e) Case 1: After 6 months of treatment, full correction of the molar and canine relationship and overbite was achieved. Distalization was stopped, and the upper arch was bonded at this stage.Figure 5. (a–c) Case 2: After 6 months of treatment, full molar and canine relationship and overbite correction was achieved. Distalization was stopped and upper arch was bonded at this stage.
The initial alignment archwire 0.14” NiTi was ligated in the upper arch. This progressed to 0.018”x0.025” NiTi archwire after one visit and 0.019”x0.025” SS archwire after two visits. The latter was the working archwire for the upper and lower arches (Figures 6 and 7).
Figure 6. (a–e) Case 1: After 10 months of treatment, full sagittal and vertical correction was achieved.Figure 7. (a–c) Case 2: After 10 months of treatment, full sagittal and vertical correction was achieved.
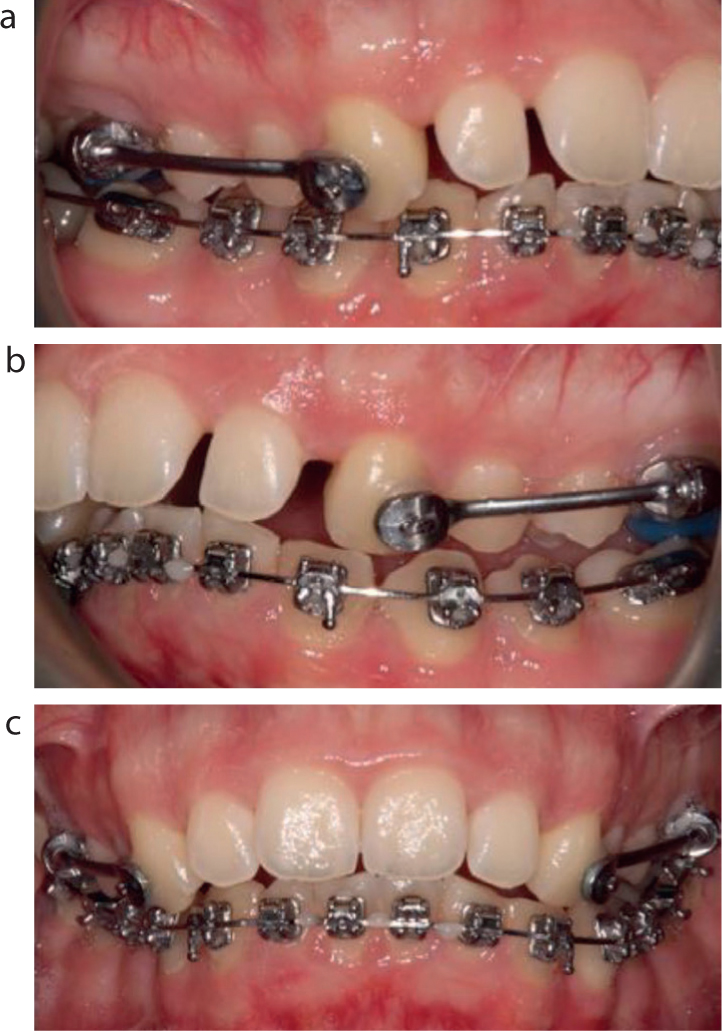
Upon removal of the CMA and bonding of the upper arch, light Class II intermaxillary elastics (4.5 oz, 3/16”) were prescribed to be worn on a part-time basis (night-time wear only) while waiting for the full expression of the mesial tip on the maxillary canine brackets. This was essential to provide anchorage and prevent the maxillary canines from tipping mesially without full root distal tip correction, causing a relapse of the canine relationship (Figure 8).
(a) Active distalization of the maxillary arch with concurrent mesialization of the mandibular arch. (b) The canine relationship is corrected mostly by distal tipping of the maxillary canine. (c) Part-time Class II intermaxillary elastics are used in the transition phase in order to allow the maxillary canine to upright and prevent relapse. (d) The transition from active distalization to anchorage phase is essential to prevent relapse of the canine relationship.
Treatment results for Cases 1 and 2
The overall treatment duration was 12 months for both cases.
Good aesthetic and occlusal results were achieved, camouflaging the underlying mild skeletal II pattern (Figures 9 and 10). A well-aligned and well-intercuspated Class I occlusion was achieved with good buccal interdigitation. Class I molar and canine relationships were established on both sides (Figures 9 and 10). The increased overbite was reduced to within average values, creating a more favourable interincisal angle. The overjet was reduced to a normal value, crowding was relieved, the arches aligned and levelled, and rotations and centreline discrepancies were corrected. A canine-guided occlusion with no non-working side interferences on lateral excursions was obtained. On the anterior excursion, there was anterior guidance and posterior disocclusion. The facial profiles in both patients showed minimal change (Table 1). For example, in Case 1, the upper lip retruded by 1 mm, the lower lip protruded by 0.5 mm and the nasio-labial angle reduced by 1° (Figure 11; Table 1). In Case 2, both upper and lower lips protruded by 2 mm (Table 1).
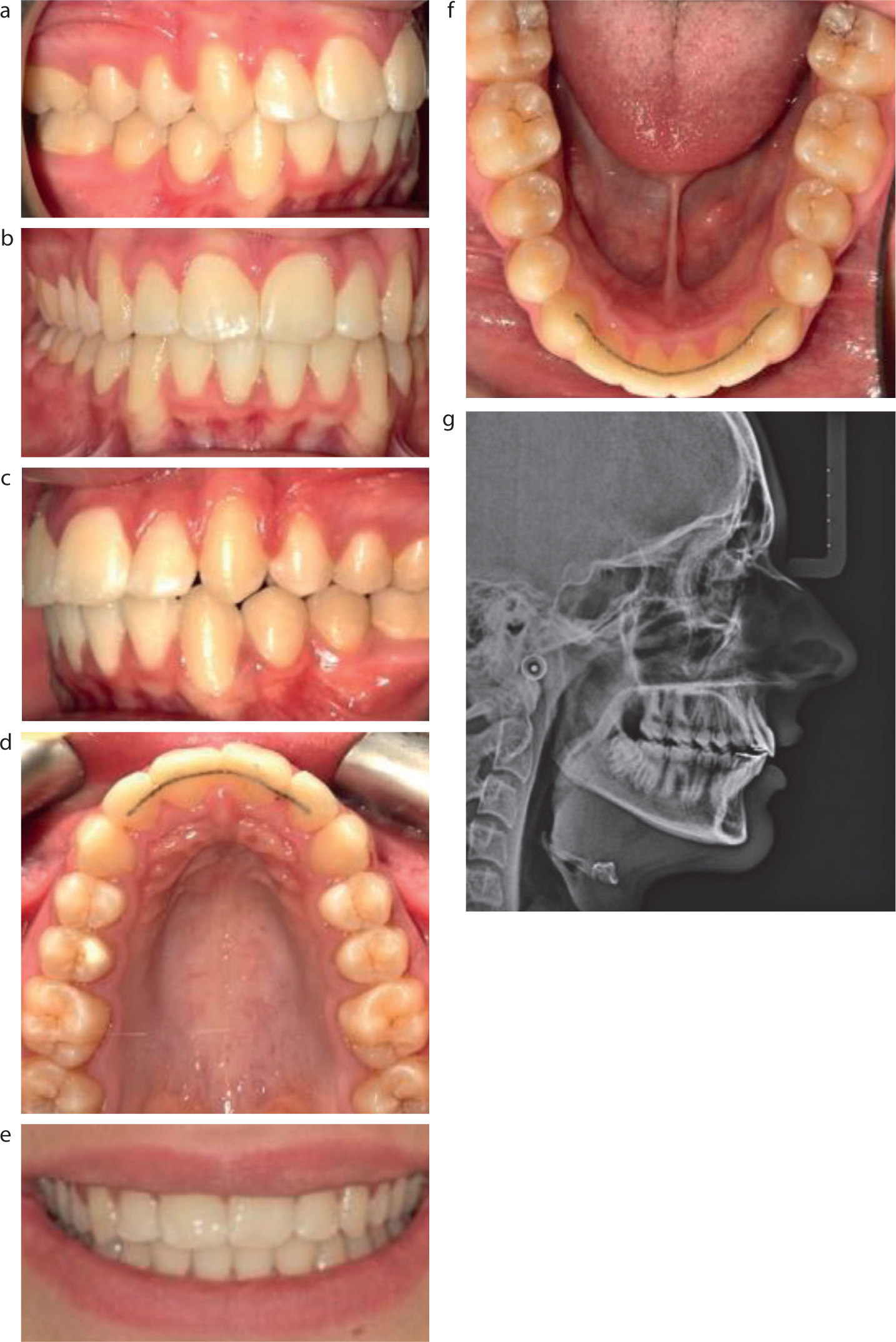
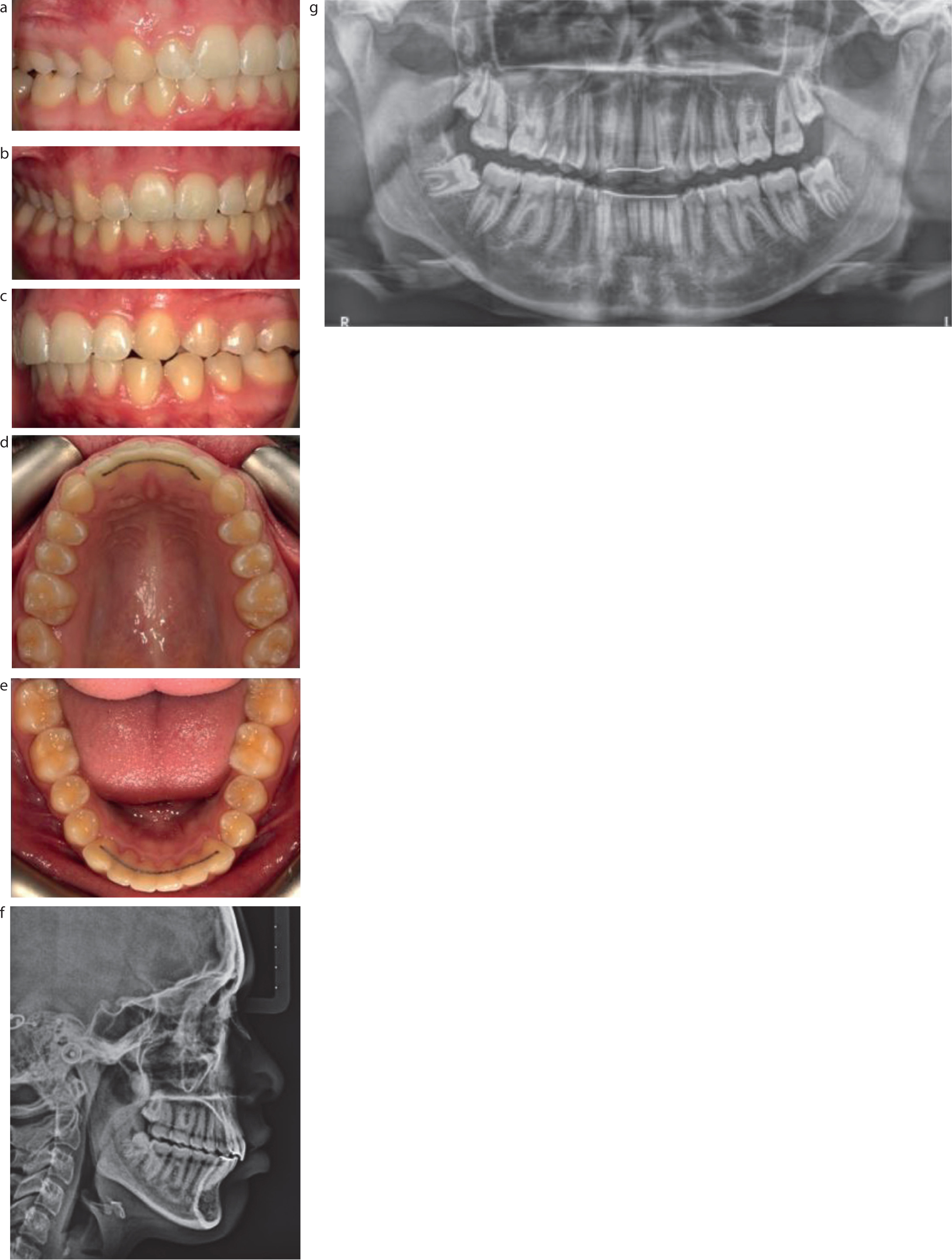
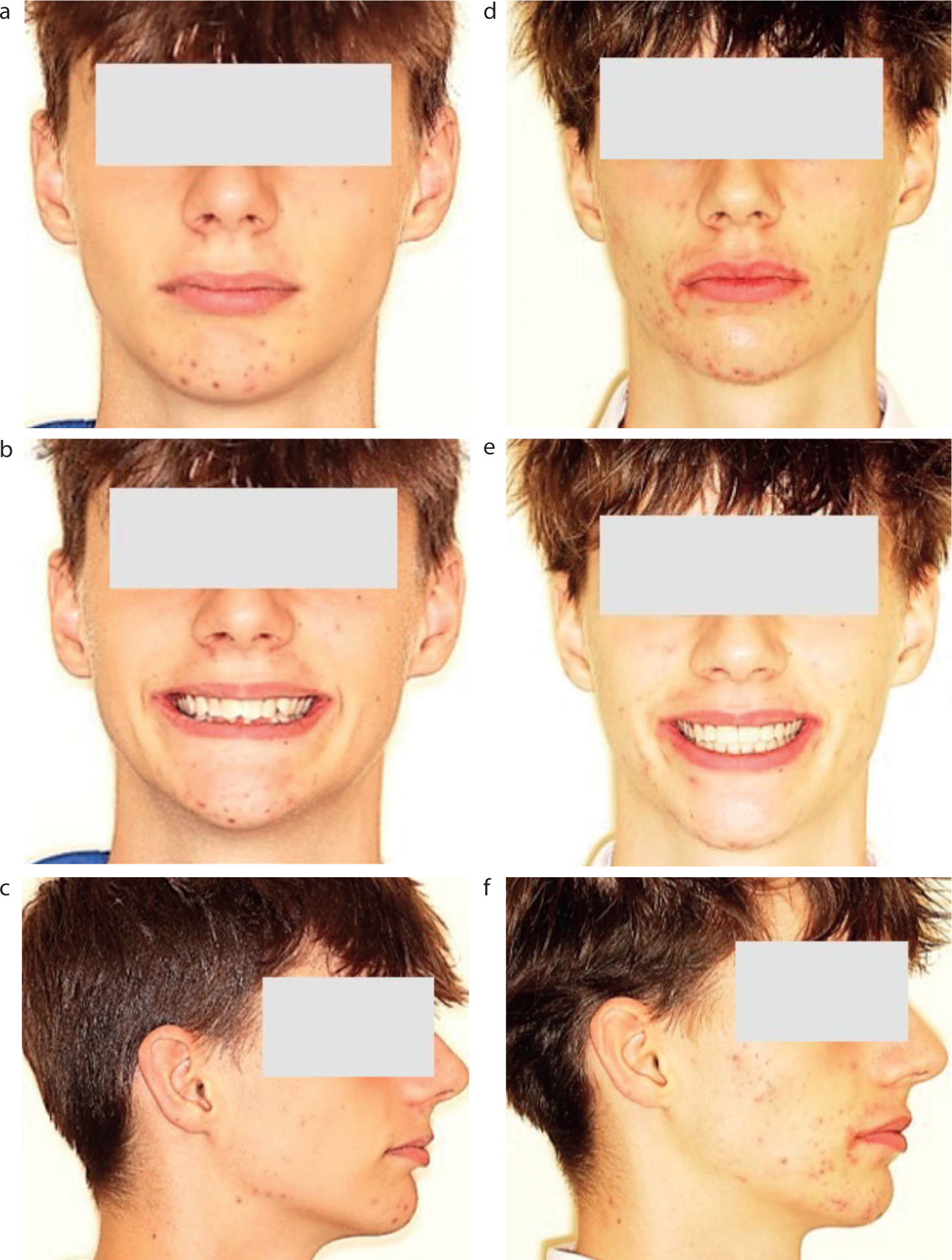
Figure 9. (a–g) Case 1: Post-treatment results after 12 months of treatment.Figure 10. (a–g) Case 2: Post-treatment results after 12 months of treatment.Figure 11.
Case 1: (a–c) Pre-treatment and (e–f) post-treatment extra-oral photographs.
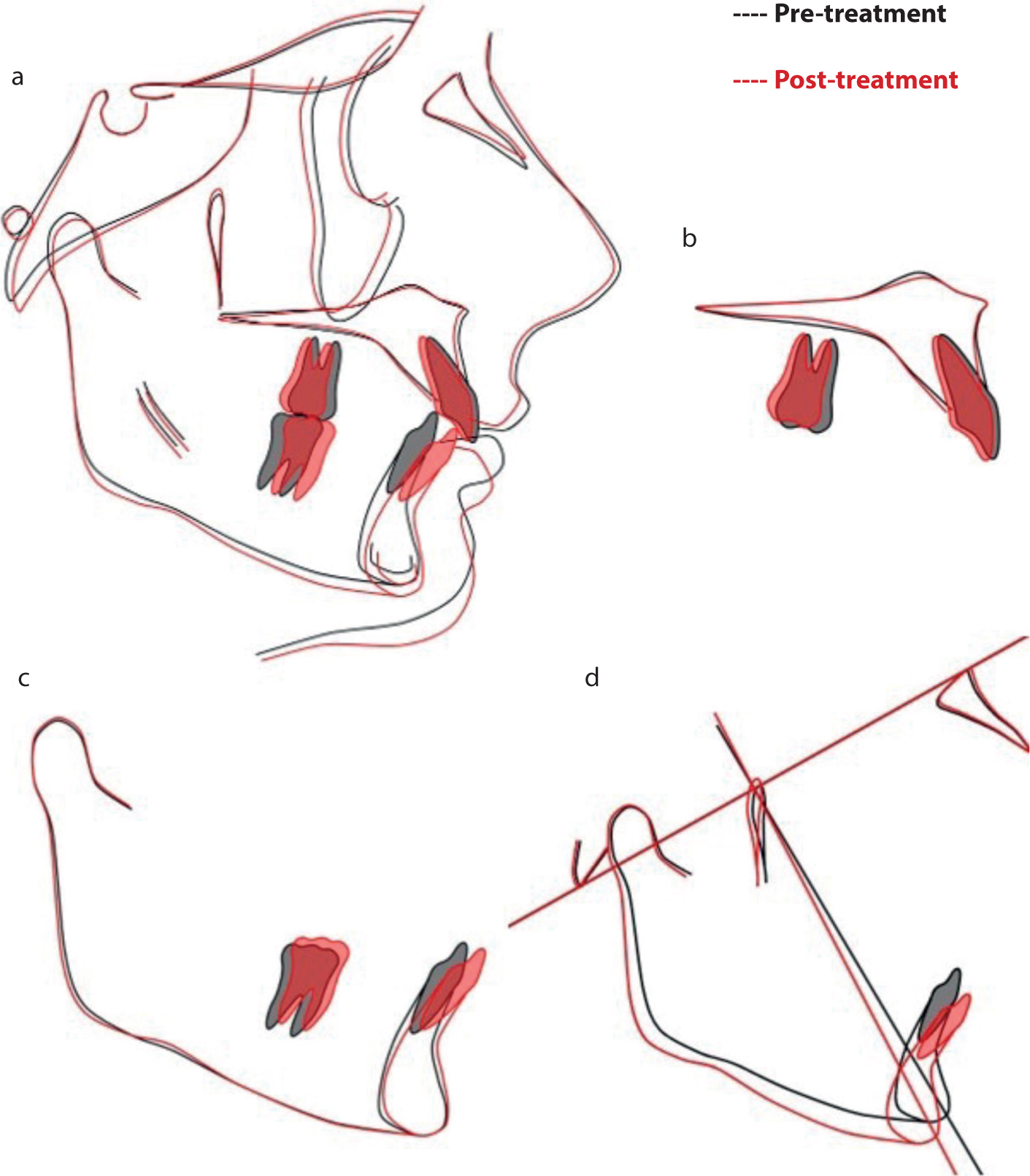
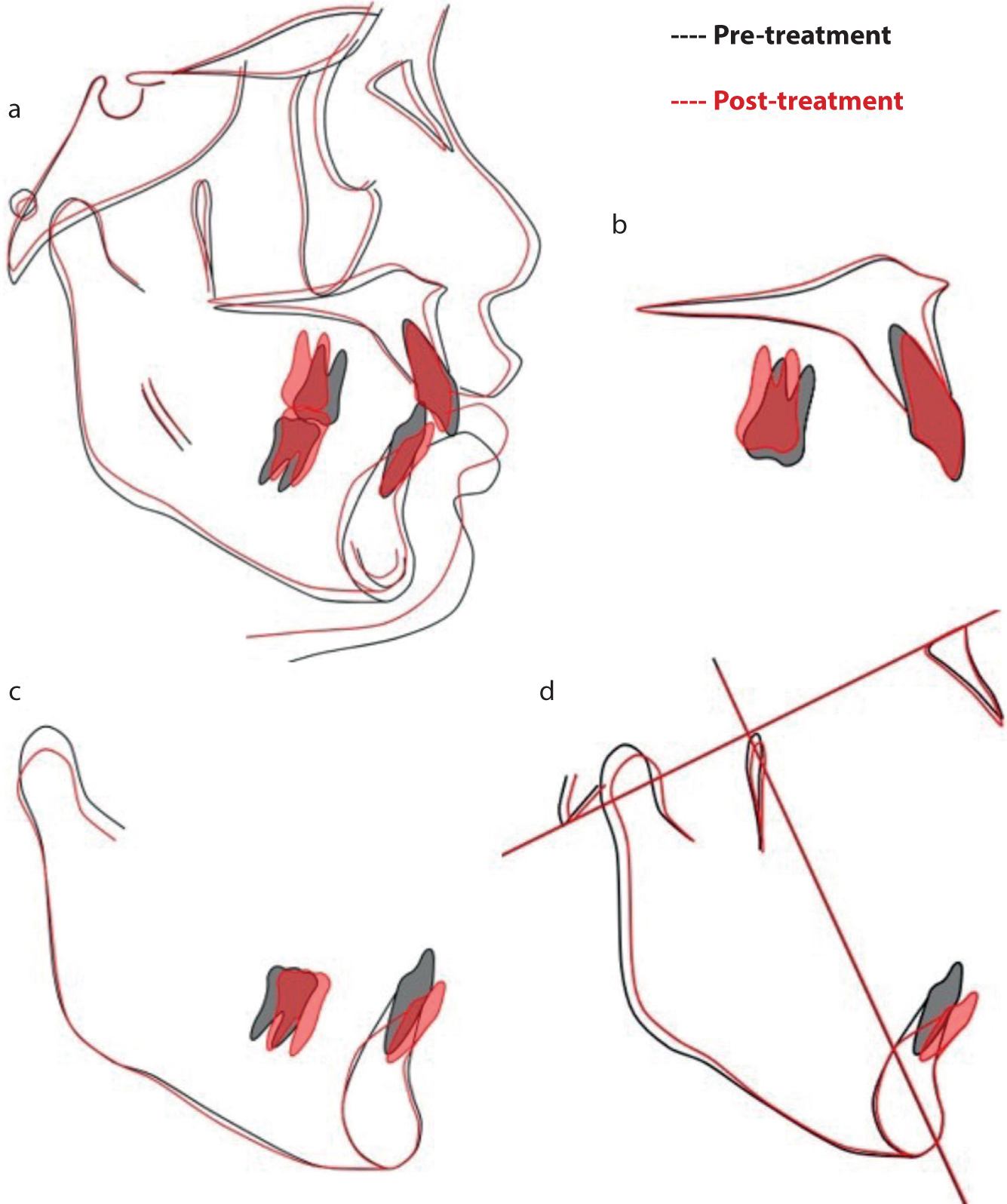
Regional cephalometric superimpositions of the mandible and maxilla showed similar overall dental movements in both cases (Figures 12 and 13). The upper incisors retroclined in Case 1 and remained relatively unchanged in Case 2. More notably, the upper molars distalized in both cases, whereas the lower molars moved mesially and extruded in both cases. The lower incisors proclined in both cases (6° proclination in both cases). Using the Ricketts' superimposition, it was concluded that the mandible in Case 1 rotated downwards and backwards (Figure 12d) and remained relatively unchanged in Case 2 (Figure 13d). Despite the backwards and downwards rotation of the mandible in Case 1, the lower lip was more protruded at the end of treatment. This can be explained by the lower incisor proclination, which was also seen in Case 2.
Figure 12.
Case 1: Pre- and post-treatment cephalometric superimpositions. (a) Overall superimposition registered on anterior cranial base. (b) Maxillary superimposition registered at ANS–PNS on best fit of palate. (c) Mandibular superimposition registered on Bjork's stable structures. (d) Ricketts' superimposition registered on the nasion–basion plane.Figure 13.
Case 2: Pre- and post-treatment cephalometric superimpositions. (a) Overall superimposition registered on anterior cranial base. (b) Maxillary superimposition registered at ANS–PNS on best fit of palate. (c) Mandibular superimposition registered on Bjork's stable structures. (d) Ricketts' superimposition registered on the nasion–basion plane.
Upper and lower bonded retainers were placed (UR2–UL2 and LR3–LL3), supplemented by full coverage upper and lower pressure-formed retainers that were prescribed to be worn on night-time basis indefinitely to ensure maintenance of the orthodontic result. The bonded retainer in the lower arch should prevent relapse of alignment of the lower labial segment and prevent late lower incisor crowding. The bonded retainer in the upper arch should prevent spaces from opening up in the upper labial segment.
Discussion
Recent research has shown the CMA to be an effective treatment option for Class II malocclusion.9,10,11,12,13
The effects of the CMA are mostly due to favourable dento-alveolar movements.14 Kim-Berman and colleagues showed that the CMA, followed by fixed appliances, produced primarily dento-alveolar effects, including changes in overbite, overjet, and molar relationships, with little lower incisor proclination.10 They also reported that the mandible was brought forward by heavy full-time elastics, although there was no statistically or clinically significant increase in mandibular length.10 Moreover, a recent systematic review found that the CMA, when used for treatment of Class II malocclusion, did not cause skeletal changes and that correction was largely dento-alveolar.7
The treatment effects in the cases described in this article correlate with those reported in the literature. In both cases, the Wits appraisal was reduced by 2 mm and 1 mm, respectively (2 mm reduction found by Kim-Berman et al10). The ANB angle decreased slightly by 1 degree in Case 1 and remained unchanged in Case 2 (1.1° reduction found by Kim-Berman et al10). Lower anterior facial height (ANS–menton) increased by 3 mm and 1 mm in Cases 1 and 2, respectively (3.7 mm increase found by Kim-Berman et al10). The dento-alveolar effects are also similar in overjet reduction, overbite reduction and molar–incisor relationship. Proclination of the lower incisors was 6° and 5° in Cases 1 and 2, respectively, compared to 4.9° that occurred during the CMA phase in the study by Kim-Berman et al.10
As with any non-surgical Class II correction that aims to mesialize lower molars and distalize upper molars, proclination of lower incisors is to be expected.16,17,18,19,20 The same side effect is seen in patients treated with a CMA.7,8,9,10,11,12,13,14
Perhaps most notable was that the lower incisors proclined irrespective of what anchorage control was used in the lower arch. In Kim-Berman et al,10 the lower incisors proclined by 4.9° when a lower vacuum-formed retainer was used. Areepong et al15 found that the increase in lower incisor proclination was not significantly different between the vacuum-formed retainer and lingual holding arch groups, 3.5° and 4.06°, respectively. Sandifer et al12 found that lower incisors proclined by 4.6° in the lingual holding arch group and by only 1.2° in the fixed appliance group.
This may suggest that, in terms of anchorage enhancement in the lower arch, fixed appliances may be more effective than lingual arch or vacuum-formed retainers in controlling the lower arch length and reducing lower incisor proclination. Hence, knowing that lower incisor proclination is inevitable, a choice should be made as to which approach is the most efficient and effective in correcting Class II with the CMA. The approach presented in this article allows for management of both the vertical and sagittal components simultaneously, thus reducing overall treatment duration. It must be noted that active Class II correction commenced at the first visit in both cases (i.e. with an initial alignment NiTi archwire in the lower arch). This may have contributed to the lower incisor proclination and increase in the lower arch length. A consideration should be given to not commencing active Class II correction with a CMA until a more stiff and larger lower archwire is in place (e.g. 0.019”x0.025” SS). However, although this would control the lower incisor inclination, it may increase overall treatment duration.
More importantly, a pre-adjusted edgewise appliance (0.022”x0.028” slot) with an MBT prescription was used to allow for complex tooth movements, ensuring adequate torque to the upper incisors (+17°, +10° palatal root torque to central and lateral incisors, respectively), which would help to improve their inclination and the interincisal angle. Class II intermaxillary elastic wear could affect the inclination of the upper incisors; however, the extra palatal root torque may have counteracted this. The additional lingual crown torque in the lower incisors (-6°) may have helped to control the lower incisor inclination.
The use of an MBT bracket on the upper canines with less mesial tip is preferable. MBT brackets have +8° mesial tip compared to the +11 of Andrews and +13 of Roth brackets. The reduced mesial tip helps to reinforce the anchorage on the canines, allowing for root uprighting, while maintaining the Class I canine relationship and preventing mesial tipping and relapse. This canine anchorage is further enhanced during the transition phase from The CMA to fixed appliances with light Class II elastics worn on a part-time basis.
Molar tubes with less mesial tip are used to prevent relapse of the molar relationship. In this case, an MBT prescription was used (0° tip) in preference to other prescriptions, for example Andrews (+5° mesial tip).
Conclusion
The concurrent use of the CMA and lower fixed appliances is an effective and efficient way to treat Class II malocclusion. The overall treatment duration in both patients was 12 months. Active Class II correction was completed after 6 months of treatment. The dental changes in both cases were mostly a result of significant lower molar mesialization and extrusion, upper molar distalization and lower incisor proclination. Very minimal changes to the upper incisor inclination were seen in both cases. Proclination of the lower incisors remains a side effect irrespective of the anchorage method used to control the lower incisors. Careful transitioning from the CMA to full fixed appliances is crucial to progress the case predictably and prevent relapse.