WHO. Infection prevention and control during healthcare when coronavirus disease (COVID-19) is suspected or confirmed: interim guidance. 2020. https://tinyurl.com/4d6z44tm (accessed March 2022)
SDCEP. Mitigation of aerosol generating procedures in dentistry: a rapid review. 2021. https://tinyurl.com/3ymjuva3 (accessed March 2022)
Royal College of Surgeons Faculty of Dental Surgery. Recommendations for paediatric dentistry during the recovery phase of the COVID-19 pandemic. 2020. https://tinyurl.com/yxznufb6 (accessed March 2022)
Royal College of Surgeons Faculty of Dental Surgery. Surgical prioritisation for children and young people requiring dental treatment under general anaesthetic. 2020. https://tinyurl.com/yus3md96 (accessed March 2022)
PHE. COVID19: guidance for maintaining services within health and care settings. Infection prevention control guidance. 2021. https://tinyurl.com/3kxyvmpx (accessed March 2022)
Zaitoun H, Kandiah P, Yesudian G, Rodd H. COVID-19: implications for paediatric dental anaesthetic services. Faculty Dent J. 2020; 11:114-119 https://doi.org/10.1308/rcsfdj.2020.89
BDA. Implementing ‘Was not brought’ in your practice: a tool for safeguarding children who miss appointments. 2019. https://tinyurl.com/2p83rzhk (accessed March 2022)
Campagnaro R, Collet GO, Andrade MP COVID-19 pandemic and pediatric dentistry: fear, eating habits and parent's oral health perceptions. Child Youth Serv Rev. 2020; 118 https://doi.org/10.1016/j.childyouth.2020.105469
RCPCH. BPSU snapshot survey – delayed presentations to dental hospital. 2020. https://tinyurl.com/5xhba8pv (accessed March 2022)
Permanent dentition acute management of traumatic injuries and follow-up care during the COVID-19 pandemic. 2020. https://tinyurl.com/3xbhp2dn (accessed March 2022)
Vergara-Buenaventura A, Chavez-Tuñon M, Castro-Ruiz C. The mental health consequences of coronavirus disease 2019 pandemic in dentistry. Disaster Med Public Health Prep. 2020; 14:e31-e34 https://doi.org/10.1017/dmp.2020.190
Xiong X, Wu Y, Fang X Mental distress in orthodontic patients during the coronavirus disease 2019 pandemic. Am J Orthod Dentofacial Orthop. 2020; 158:824-833.e1 https://doi.org/10.1016/j.ajodo.2020.07.005
Cotrin P, Peloso RM, Oliveira RC Impact of coronavirus pandemic in appointments and anxiety/concerns of patients regarding orthodontic treatment. Orthod Craniofac Res. 2020; 23:455-461 https://doi.org/10.1111/ocr.12395
Sinha PK, Nanda RS, McNeil DW. Perceived orthodontist behaviors that predict patient satisfaction, orthodontist-patient relationship, and patient adherence in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1996; 110:370-377 https://doi.org/10.1016/s0889-5406(96)70037-9
WHO. Telemedicine: opportunities and developments in member states: report on the second global survey on eHealth 2009. 2010. https://tinyurl.com/mr23eh5c (accessed March 2022)
Estai M, Kanagasingam Y, Tennant M, Bunt S. A systematic review of the research evidence for the benefits of teledentistry. J Telemed Telecare. 2018; 24:147-156 https://doi.org/10.1177/1357633X16689433
How COVID-19 has changed our Practice: Adapting to the New Normal Orthodontic Update 2025 15:2, 75-79.
Abstract
The COVID-19 pandemic has led to changes in all aspects of dentistry, from administration adjustments to vast alterations in training and clinical practice. This article highlights the impact the pandemic has had on paediatric dentistry and orthodontics, and to discuss the changes that have been implemented as a result. It is likely that some of these changes will be permanent and recognizing how to adapt our practice will allow us to continue to provide the best possible care to our patients.
CPD/Clinical Relevance: It is in both the patients' and the clinicians' best interests to be fully informed of the effects that the COVID-19 pandemic has had, and how to adapt in order to continue to give the best possible care for our patients.
Article
The coronavirus disease 2019 (COVID-19) pandemic has caused upheaval to all aspects of everyday social and working life. Although there are successful vaccines, the pandemic is likely to instil long-lasting changes in dentistry. Some of these necessary adaptations are likely to improve the way we work, but others may not, or may be less beneficial for our patients. Whichever way we look at it, the concept of normality within dentistry will be different. Learning to adapt to the new environment will allow us to continue to provide the best possible care for our patients.
This article focuses on the changes observed within the orthodontic and paediatric dental specialties, within a dental hospital setting and highlights the impact on treatment, patient attitudes, clinical practice and training.
Impact on clinical practice
The emergence of the SARS-CoV-2 virus and the resulting COVID 19 pandemic led many governments to curtail the delivery of dental health services. Since June 2020, there has been remobilization of these services, albeit in a different way to what we were used to. All dental care specialties have had to introduce modifications to their standard operating procedures (SOPs), including:
Pre-visit screening for COVID-19 symptoms;
Pre-visit triaging of potential urgent treatments;
Altering appointment times to manage footfall and minimize crowded waiting rooms;
Altering the scope of treatments available;
Introduction of fallow time following aerosol-generating procedures (AGPs);
COVID-19 testing 72 hours prior to general anaesthesia (GA).
Dental professionals may be at risk of acquiring COVID-19 through multiple transmission routes. It has been extensively discussed that aerosol-generating procedures (AGP) carry a higher risk of transmitting COVID-19, although this has not yet currently been proven. An AGP can be defined as any medical or patient-care procedure that results in the production of air-borne particles <5 μm in size.1 Studies looking to identify SARS-CoV-2 in aerosols in clinical environments have used techniques to detect viral RNA, which does not describe infectious particles.2 Results from experimental laboratory studies have proposed that virus transmission via aerosol is possible; however, these experiments have not been undertaken in a clinical setting, where there would be appropriate PPE and disinfection regimens.2Table 1 outlines the AGPs for orthodontics and paediatric dentistry.
Orthodontics
Surface wash and dry with 3 in 1, where air and water are used together
Composite removal with high-speed handpiece
Ceramic removal with high-speed handpiece
Sandblasting (eg of fixed retainer or customized bracket)
Interproximal reduction using high-speed handpiece
Ultrasonic scaling
Paediatric dentistry
Restorations and initial endodontic access
Conventional crowns for primary and permanent dentition
Ultrasonic scaling
Fissure sealants with 3:1, where air and water used together
Surgical extractions
The Scottish Dental Clinical Effectiveness Programme (SDCEP) rapid review into the mitigation of AGPs in dentistry collated evidence from many sources regarding recommended fallow time when undertaking AGPs. Their protocol has been accepted by the office of the UK Chief Dental Officer, with fallow times based on the use of high-flow suction or rubber dam.2 The suggested protocol is as follows (correct at time of writing):
For 1–5 air changes per hour (ACH), or for unknown ACH, the baseline fallow time is 30 minutes;
For 6–9 ACH, a fallow time of 20 minutes is recommended;
For 10 or more ACH, a fallow time of 10 minutes is recommended.
It was also recommended that fallow time may not be considered necessary for family members with successive appointments, if in the same household, and also that fallow time can be commenced from the end of the aerosol production (immediately post-AGP).
These protocols are a guide, and all workplaces should make their SOP with regards to fallow time, based on their ventilation system and treatment adjuncts.
The British Orthodontic Society has produced a very informative document to summarize the findings from both the UK and SCDEP guidelines.3 This document, together with the RCS guidelines4 with recommendations for paediatric dentistry, outlines the methods to minimize aerosol production within both specialties.
Impact on treatments
When the pandemic hit crisis point in March 2020, the General Dental Council (GDC) response was to suspend all non-urgent dental care, including orthodontics and paediatric dentistry. All patients within the dental hospital were contacted via telephone or letter and given advice for the lockdown period.
In orthodontics, patients were advised to discontinue any active treatment adjuncts, such as elastic wear or turning appliance screws. They were counselled on the importance of maintaining an appropriate diet to minimize breakages, and excellent oral hygiene. Many patients will have encountered delays in their orthodontic treatment, not only from the lack of appointments to progress treatment, but also due to the suspension of active treatment mechanics and the likelihood of increased appliance breakages. This was then confounded when clinics restarted. Extra precautions had been put in place to ensure adherence to social distancing measures, such as fewer patients seen, longer treatment times and fallow times after appointments. This reduced capacity, combined with a significant proportion of patients requiring repairs and replacement appliances, led to delay in treatment progression.
As orthodontists, we must recognize this and take steps within our clinical work to ensure that patients can continue to progress with treatment even with increased recall times. Such measures may include:
Bonding with self-etch primers instead of traditional etch and bond, to reduce the need for an AGP and associated fallow time. Research has shown no significant difference in success when bonding with self-etching primers, compared to separate etch and bond;5
Ensuring NiTi wires are cinched back to prevent sharp ends and disengagement from terminal molar tubes;
Calibrate open-coil lengths when space opening, to avoid excessive space, root convergence or proclination of anterior teeth;
Avoid excessive posterior bite blocks when using them to prevent premature contact of brackets. This will prevent excessive alterations to the occlusal plane if appointments are missed;
Ensure appropriate orthodontic extraction timing; in particular ensure that sufficient anchorage is established before requesting extractions;
Consider retaining final treatment models and using these for remaking retainers for patients who may lose/break theirs. These are then likely to be securely posted to the patient and prevent the need for extra appointments.
Akin to orthodontics, COVID-19 has had a significant impact on the provision of paediatric dental care, access to GA provision and clinical capacity. In March 2020, all patients were contacted via letter and telephone to provide prevention guidance and advice, analgesics and, if indicated, antibiotics were provided.2 For those children requiring urgent dental care, provision was provided under local and GA. With limited PPE and open-plan clinics in most paediatric dental departments, services have been pushed to further develop AGP-free minimally invasive caries management. These included:
Clinical photographs sent by parents for pre-screening assessment;
Patient information to support dental anxiety because of new PPE clothing, and social stories;
Silver diamine fluoride use for arresting caries and dentine hypersensitivity for molar–incisor hypomineralization (MIH). The BSPD has produced patient and clinician information to support practices in this treatment modality, which can be found on their website (www.bspd.co.uk/Professionals/Resources);
Hall crown technique;
Where biological technique contraindicated the above methods, an extraction may be indicated as the treatment of choice over invasive treatment in the primary dentition;
Initial caries temporization for up to 6 months in the permanent dentition;
Use of crown forms to minimize clinical treatment time for enamel dentine fractures following dental trauma;
Use of self-etching adhesive when placement of splints following trauma, with removal of splint using wire cutters and orthodontic bracket remover pliers;
Reducing fallow time by use of the dry dam, which is well tolerated by children;
Use of inhalation sedation in urgent cases to support the reduced GA access;
Digital health technology and resources to support self-care and prevention.
Prioritizing urgent dental care
The pandemic has brought emergency dental care to the forefront. With limited access to services clinical urgency took priority from the traditional referral to treat time. Patients were reprioritized based on the conditions described in Table 2.4
Conditions taken into consideration for re-prioritization of paediatric urgent care
Priority to children with medical comorbidities with increased risk of complications as a result of dental infections and poor oral health:Diabetes, cardiac conditions, epilepsy or inherited metabolic disorder
Patients at increased risk of self-harm
Trauma in primary dentition: child is symptomatic and unable to occlude
Uncooperative for dental treatment under local anaesthetic with:Acute dental infection with no resolution with antibioticsIntractable pain or discomfortFacial swelling as a result of dental diseaseCompromised swallow or risk of aspiration of tooth
‘Red-Flag’ conditions that may complicate/exacerbate dental management should they present as an emergency:Haematological conditions, eg haemophilia, Von Willebrand'sIncreased risk of infection: immunocompromised, diabetic, chemotherapy, steroids, immunosuppressantsIncreased risk of infective endocarditis
Although dental GA services have been re-established for medically compromised paediatric dental care, the pandemic has resulted in the cessation of five elective dental GA services per week with Ad-Hoc lists provided infrequently at the time of publication. To overcome this all patients were validated on the GA waiting list, and reprioritized based on their clinical urgency.5 However, when surgical lists are provided there is also a reduction in patient number from previous eight children per theatre session to four or five children due changes in infection control procedures, in line with Public Health England guidance.6 This provides significant concern on an already extensive waiting list for children, especially those with additional needs, with potential long-term impact on children's overall wellbeing and dental health.7
Many children who are on the GA pathway are recognized as being in a vulnerable cohort, where English may not be a family's first language, are from more deprived backgrounds and there is an increased risk of safeguarding concerns. For those patients who do not respond to contact, the ‘Was Not Brought’ policy was implemented to support families.8 It is important to note that families may often be anxious to attend the hospital setting for dental treatment,9 and delayed presentation has been noted across all paediatric specialities by the Royal College of Paediatric and Child Health.10
Management of dental trauma
Throughout the pandemic, trauma has been a common referral for urgent care. The BSPD has produced a consensus guideline on the management of dental trauma and streamlined dental visits in line with evidence-based guidance.11 Prior to the initial visit, parents are encouraged to provide clinical photographs, enabling assessment of the clinical urgency of the initial appointment. Communication has been improved with accident and emergencies attendees to sign-post and refer patients who require specialist-led care due to reduction in routine GDP access. To minimize treatment visits endodontic management of MTA root-ended closure in the immature apex can be provided in a single visit, or dressing with Cavit (Manufacturer, location) to reduce a further AGP appointment and enable the continuation of treatment to be provided on the open plan clinic.
Impact on dental referrals
Paediatric department referrals significantly declined as a result of the cessation/reduction of GDP/community dental access. This resulted in direct contact to the hospital by parents, GPs, schools, and social workers with individual concerns and referrals for children. Within the department the current referral rate is estimated to be at 60% of pre-pandemic levels, and there are concerns within the profession that important time-dependent referrals will be missed. These include referrals for the management of the developing dentition, with conditions such as MIH and extraction of poor prognosis first permanent molars, ectopic canines, delayed eruption, infraocclusion of primary molars, to name a few.
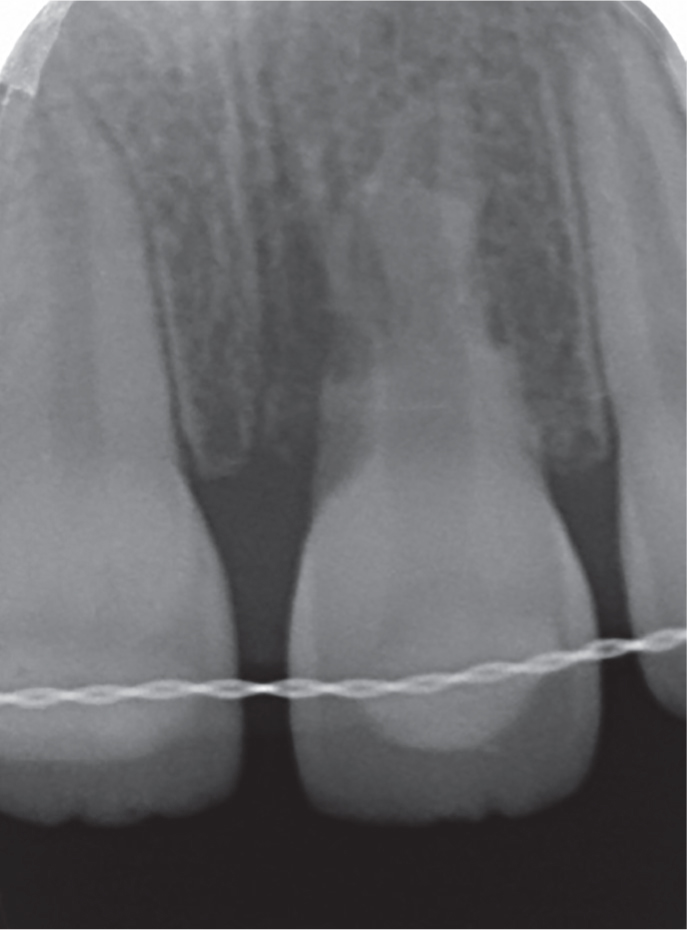
The decline in referrals has also resulted in delayed presentation of acute trauma – with a decline in patients accessing urgent treatment in primary care, and onwards referral for those cases requiring specialist care. The delay in presentation can have detrimental outcomes (Figures 1 and 2). This is the case of a 13-year-old boy who sustained an avulsion injury to UL1 during the first COVID-19 lockdown, and subsequently had the tooth re-implanted and splinted in A&E. The patient was referred to the dental hospital 1-year post trauma. The rigid splint was still in situ, and the UL1 had not received any active root treatment. As a result, the mature permanent tooth presented with significant inflammatory and replacement resorption (Figure 2). Cases such as this result in the breaking of bad news to an understandably shocked family, regarding a tooth of hopeless prognosis. Practitioners are advised to use guidelines published by the BSPD and International Dental Trauma Association in the management of dental trauma.11
Figure 1. Clinical photograph showing a 13-year-old boy with a rigid splint in situ following re-implantation of avulsed UL1. The splint had been in situ for 12 months and no further adjunctive treatment had been undertaken.Figure 2. Peri-apical radiograph showing significant internal and external inflammatory root resorption of the UL1 root.
The Chief Dental Officer has published new guidelines for dental practitioners on the recall priorities for paediatric patients.12 The document highlights those who are the highest priority of recall, which includes those who are medically compromised, looked after or on a child protection plan, children under 2 years old, and those who have not had a face-to-face examination in over 12 months.
Impact on patients' mental health
Many patients will have encountered problems with their orthodontic appliances during the lockdown period and active treatment suspension, during which they could not seek face-to-face help from their specialist clinician. Patients were directed towards the extensive information available on the British Orthodontic Society (BOS) website. They were also given details of a telephone triage service with the dental hospital for anything that could not be self-managed. Once clinics were back up and running, patients were seen with extra protective measures, such as increased PPE and reduced family members allowed into the clinic. The extended period without being seen, together with the heightened precautions upon restarting clinics and the general level of global anxiety, can profoundly affect a patient's mental health and their attitude towards treatment.
The consensus among clinicians within both departments is that, during the lockdown, patients' oral hygiene has become suboptimal, with loss of routine in the home environment. Upon returning to clinic they are now keener to accept compromised orthodontic treatment results and have the appliances removed as soon as possible. This is in addition to the patient's and parent's own anxiety in attending the hospital setting during the COVID-19 pandemic.13
Multiple studies looking at patients' mental attitudes have been published with data collected during the COVID-19 pandemic. The results from these studies show that the patient's primary concern with orthodontic treatment was the implication of missed appointments on total treatment time, with around 64% of patients acknowledging that the pandemic would have a negative impact on the course of their treatment.14 The studies also suggest that female patients are more likely to have mental distress than male patients.14 There was no correlation between patient age and levels of anxiety.15
Patient communication has been paramount during the pandemic to help relieve anxiety towards treatment. Most orthodontic appliances can be left in place for many months without significant adverse effects to the dentition, provided there are no breakages or untoward incidences. However, most patients are used to seeing their clinician more frequently and are unlikely to be aware of this fact. It is not a new notion that good communication between a clinician and a patient is a good predictor for success of treatment.16 Xiong et al14 found that patients who received lockdown information direct from their doctor, showed less anxiety compared with patients who had generic communication. This reminds us that a good patient–doctor relationship is paramount, and can lead to increased patient reassurance, satisfaction and communication.
Virtual healthcare and COVID-19
The World Health Organization defines telemedicine as ‘a use of telecommunications and virtual technologies to provide healthcare outside of traditional healthcare facilities’.17 It was originally developed to help facilitate healthcare in remote areas; however, as technology has advanced, telecommunication has grown, with this especially true in these unprecedented times.
The COVID-19 pandemic not only denied us the ability to see non-urgent patients, but on service remobilization, it led us to reduced chair time and reduced patient capacity. Telemedicine, or ‘teledentistry’, allows us to reach patients remotely, thus maintaining the reduced capacity but ensuring our patients are not left unsupervised.
The idea of ‘telemedicine’ is not a new concept in the dental field. A systematic review in 201818 reviewed the benefits of teledentistry, including access and supervision within orthodontics. The review found that virtual communication could be a useful way of engaging patients and clinicians alike and allows for easy access to information. The review also found that teledentistry has a positive economic impact on the dental profession.
Clinical experience would tell us that, within orthodontics, the long-term application of virtual consultation would be limited to: emergency triaging, validation consultation, an interim review of removable appliances (functional appliances or aligner therapy); and retainer review. Multi-bracket systems are not optimal for virtual clinics due to the hands-on nature of the treatment.
Within this dental hospital, telecommunication has been primarily used to triage orthodontic and paediatric emergencies and for the use of some multidisciplinary team (MDT) clinics. Orthodontic emergencies are managed on a step-wise approach. First the patient has an oral consultation with a specifically trained nurse. The nurse manages the patient as appropriate over the phone and directs patients to the extensive ‘self-help’ information available on the British Orthodontic Society website. If the problem cannot be managed in this way then the patient will be asked to send photos via a secure email route. A qualified orthodontic specialist then review these, and the patient will be contacted with further advice, or will be offered a face-to-face appointment. For paediatric patients, new patient assessments for those who are medically compromised, or for those with additional needs, have been undertaken virtually, to minimize hospital attendance and the length of hospital appointments, and in some cases, enabling direct listing for urgent dental care. The virtual appointment allows a streamlined clinical appointment when attending, and also enables clinicians to provide pre-appointment information, such as that found on the British Society of Paediatric Dentistry website,19 to prepare patients.
For use within MDT clinics, virtual communication is primarily for the treatment planning or review stage. The patient will have already attended for initial examination and full records for treatment planning, including study models, photos and radiographs, will be available. These records are reviewed by the MDT and discussed with the patient virtually using the ‘Attend Anywhere’ system. This works well because the appointments are primarily discussion sessions and only occasionally require the patient to be chairside. Review clinics may be for reviewing patients who are over 1-year post-treatment – as may be the case for post-surgical completed orthognathic cases. Again, if anything untoward arises in these situations, the patient will be offered a face-to-face review.
Overall, the use of teledentistry is a rapidly evolving field with many potential benefits to clinical practice. However, we need to be careful not to compromise patient treatment or the patient–doctor relationship. The COVID-19 pandemic has undeniably placed extra strains on our services.
Impact on dental training
Now that clinics and treatments have been re-established, the impact on training has been reduced. However the struggle is not over. Many dental hospitals use open-plan polyclinics for training, which allow multiple trainees to be supervised collectively. Undertaking AGPs in these areas poses an obvious concern and therefore leads to a reduction in the available space for clinical activity. Nationally, dental trainees were redeployed to assist on medical wards during the COVID-19 waves. Despite these challenges, dental schools and deaneries have worked hard to ensure that trainees have been able to progress as planned, with many Royal Collage Examinations undertaken virtually.
The effect the pandemic has had on orthodontic and paediatric dental specialty training is yet to be fully realized. Some exams planned for March 2020 had to be cancelled and trainees were required to extend their training posts. The knock-on effect of this meant that the starts of other training posts had to be delayed and, therefore, there were fewer positions available for annual STR applications. Although specialists in orthodontics outnumber those in paediatric dentistry by almost 6:1, work-force provision is a significant concern if there is a prolonged impact on national recruitment.22 Alongside this, trainees currently undertaking their training have had a reduction in clinics and theatre opportunities because elective treatments were cancelled completely due to the pressures of COVID-19 on the NHS system, such as orthognathic surgery, and significant reduction in GA provision for paediatric dental care. Trainees who were deemed clinically vulnerable were also affected owing to the shielding impacting their clinical development during training. This impact on trainee progress has led to the new ‘no blame’ outcome 10 being developed for the ARCP process, which recognizes a trainee's need to extend training as a result of the COVID-19 pandemic.
Conclusion
We do not yet know the full financial, clinical and ethical impacts the COVID-19 pandemic will leave in its wake. It is likely that some of the adaptations that have been necessary in our clinical practice will be long-standing, s and will be carried forward for many years to come. The introduction of a viable vaccination and mass-testing has led to restrictions being eased. The COVID-19 pandemic certainly had an impact on access to dental care, and there is likely to be a long-term impact on children's oral health. This requires longitudinal evaluation and continued need to highlight the importance of prioritizing children for recall in primary care. What is clear is that the pandemic has forced us to re-evaluate the way we work, and has shown that we have the ability to adapt to a ‘new normal’ to continue to provide the best possible care for our patients.