A case is described of a 13-year-old boy who presented with infra-occluded primary molars in three quadrants. Creation of space allowed the second premolars in two quadrants to erupt spontaneously. The first premolar in the remaining quadrant did not erupt spontaneously, failing to reach occlusal contact despite orthodontic traction.
CPD/Clinical Relevance: This case demonstrates apparent intermittent ankylosis of a maxillary first premolar.
Article
Graham Oliver
The majority of unerupted teeth that fail to erupt have a physical obstruction; either osteogenic, odontogenic, soft tissue, or there may be a history of trauma. Removal of the obstruction often leads to spontaneous eruption of the affected tooth.1 Other causes for failure of eruption include abnormal tooth germ position, bony deficiency, such as in cleft palate cases, ankylosis and genetic conditions. Genetic conditions that can impede tooth eruption are often associated with syndromes such as Cleido-Cranial Dysplasia (CCD) and Gorlin-Goltz syndrome. The physical mechanism of tooth eruption is unknown but the most popular theories are:
Vascular pressure theory;
Periodontal traction theory;
Root elongation theory;
Bony remodelling theory.
Ankylosis is defined as the fusion of bone and cementum due to a discontinuation of the periodontal ligament. It is more common in the deciduous than the permanent dentition and is most often seen in the buccal segments. The aetiology of tooth ankylosis is essentially unknown but appears to develop due to a disturbance of the periodontal ligament. These disruptions are thought to include endocrine and metabolic disorders, genetic tendency, periapical infections, trauma or previous dental procedures. Treatment of ankylosed teeth often involves extraction, restorative build-up or localized osteotomy.
There are, however, reported cases of failure of eruption with no obvious local or systemic cause. This is often described as Primary Failure of Eruption (PFE). PFE is a rare complication encountered in the developing dentition seen in only about 0.06% of the population.2,3 It is most often reported in the permanent dentition but has also been reported in the primary dentition.4 Characteristic findings of PFE include:5,6
Posterior teeth more commonly affected than anterior teeth;
Affected teeth may show initial signs of eruption then fail to erupt further;
Both primary and permanent dentition can be affected;
Unilateral or bilateral;
Permanent teeth have a tendency to become ankylosed;
Application of orthodontic forces leads to ankylosis rather than normal tooth movement;
Tendency to occur in isolation, with an absence of affected family members.
Making a definitive diagnosis of PFE can therefore be very difficult as many theories as to possible causes and further classifications have been proposed. Earlier diagnostic criteria for PFE included unerupted teeth with:
No evidence of a mechanical, pathological, or systemic cause of obstruction contributing to eruption failure of the affected tooth or teeth (involved teeth that may have erupted initially and then ceased to erupt prior to establishing occlusal contact or may have failed to erupt entirely);
No evidence of successful orthodontic extrusion of the affected tooth or teeth.5
A genetic link was first questioned over 40 years ago when an autosomal dominant inheritance trait was noticed.7 A possible cause for PFE is from a genetic mutation of the PTHR1 (Parathyroid Hormone Receptor 1) gene.8
The clinical problems from PFE can be significant. Most cases of PFE may not be diagnosed up until midorthodontic treatment and will have a significant impact on the treatment plan when ankylosis occurs. Treatment options such as segmental osteotomies may then be required.
Diagnosis and aetiology
A 13-year-old boy was referred to the Orthodontic Department of the John Radcliffe Hospital, Oxford, with retained deciduous molars that appeared to be infra-occluded. The patient had no complaints himself and was medically fit and well.
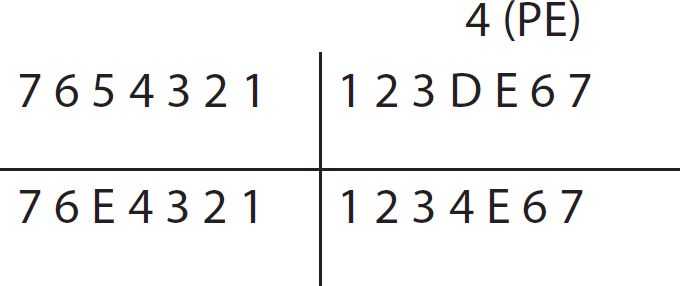
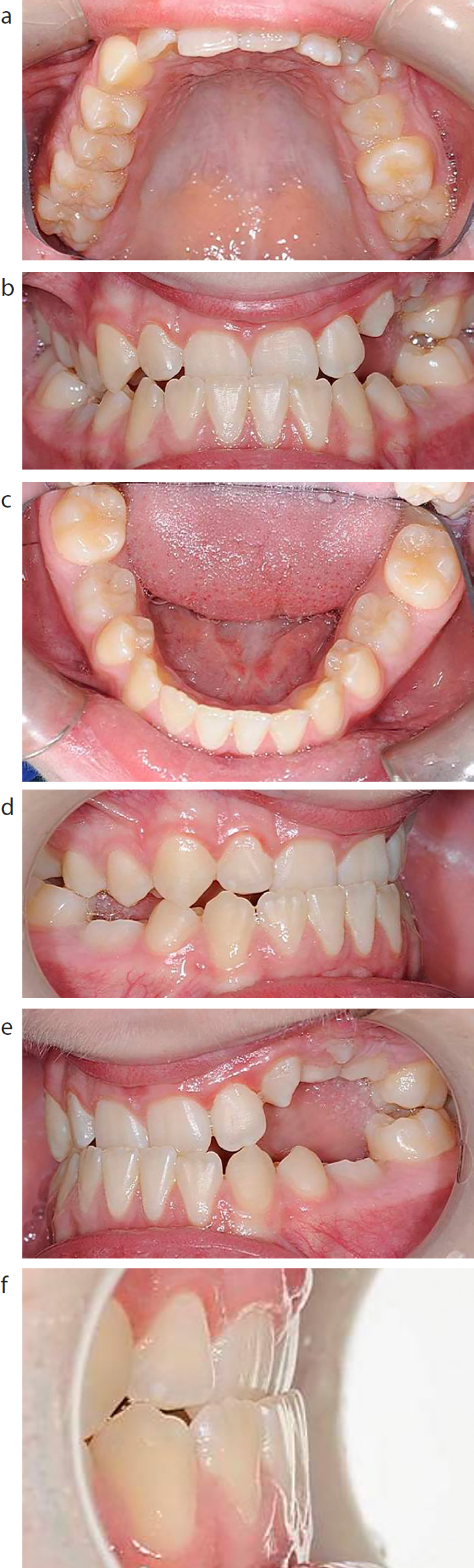
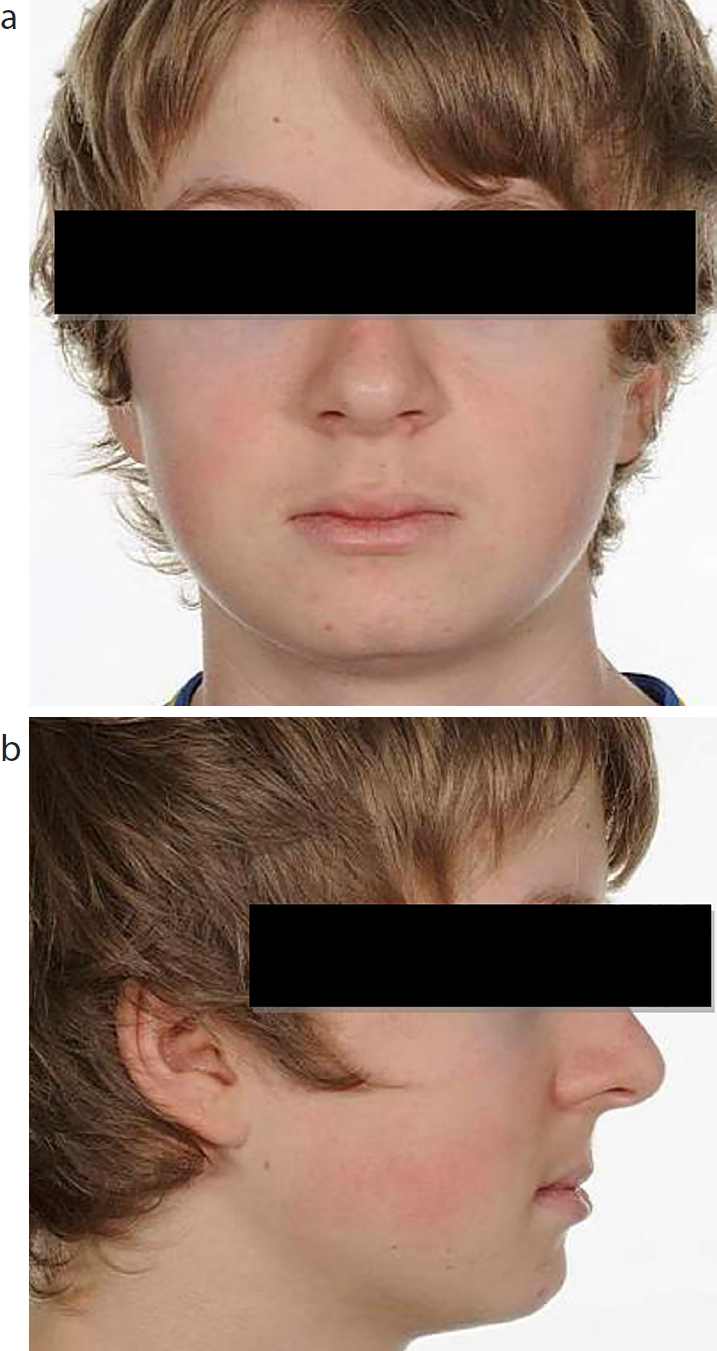
On examination, the patient presented with a mild skeletal III discrepancy due to maxillary hypoplasia, a low Frankfort-mandibular plane angle and reduced lower face height. There was no obvious facial asymmetry. Lips were competent with a normal nasolabial angle. The teeth present are shown in Figure 1. There was poor plaque control in the upper labial segment, however, no caries was clinically evident. The lower arch was well aligned with infra-occluded primary second molars. The upper arch showed mild crowding with first and second left primary molars infra-occluded and delayed eruption of the permanent canine (compared with its antimere). There was a Class III incisor relationship with a 0 mm overjet in retruded contact position, associated with an anterior displacement into a reverse overjet with a normal overbite in intercuspal position (ICP). A buccal crossbite was evident, as seen in Figure 2. The centrelines were coincident with one another and the midline of the face. An orthopantomogram confirmed the presences of both mandibular and maxillary left second premolars. The mandibular second premolars were mildly disto-angually impacted. The mesial roots of both mandibular deciduous molars showed limited resorption. Third molars were developing in all quadrants. No other dental pathology was noted (Figures 3 and 4).
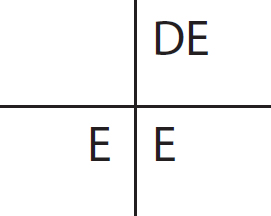
Figure 1. Teeth present at initial assessment.Figure 2.
(a–f) Pre-treatment views.Figure 3.
(a, b) Pre-treatment extra-oral views.Figure 4.
(a, b) Pre-treatment orthopantomogram and lateral cephalogram taken at appointment for fitting of trans-palatal arch.
Problem list
Poor plaque control;
Infra-occluded LRE, ULDE and LLE;
Edge-to-edge bite with anterior displacement;
Buccal crossbite.
The aims of treatment were to:
Improve oral hygiene;
Establish the unerupted premolars into occlusion;
Eliminate the anterior displacement;
Level and align the arches;
Correct buccal crossbite;
Achieve an ideal overjet and overbite.
Treatment plan
Extraction under local anaesthesia of:
Trans-palatal arch maxillary first molars;
Upper and lower fixed appliances;
Indefinite retention.
Treatment
Initially, the patient was referred to his dentist for extraction of the remaining deciduous dentition. A trans-palatal arch was cemented to the maxillary permanent first molars to maintain space for the premolars.
Six months later the LR5 erupted spontaneously; however, no change was seen in relation to the UL45 and LL5 (Figure 5). Subsequently, at the following appointment, it transpired that palatal to the erupting UL4 was a retained root from the ULD. This was referred for removal in the Oral and Maxillofacial Surgery Department. A lower fixed appliance was then bonded. As both the UL4 and UL5 showed little signs of movement, active push coil was placed between the UL3 and UL6. At the following appointment, the UL5 had erupted sufficiently to enable bonding and alignment. Over the following four appointments, utilizing vertical traction with intermaxillary elastics, the UL4 had not moved. Therefore, a second referral was made for a surgical opinion. On examination with a periapical film, no lamina dura were noted around the UL4 (Figure 6). After removal of the ULD root by the Oral and Maxillofacial Surgery Department, and further creation of space, the UL4 still failed to show any signs of movement over the following six months. A further opinion was gained and a sectional osteotomy was treatment planned. However, within two appointments of continued push coil between UL3 and UL5 to create space for the sectional osteotomy using the UL4 as anchorage to prevent centreline shift, the UL4 spontaneously erupted further (Figure 7). The osteotomy was therefore no longer required. After rebonding, the premolars were aligned further. However, a 2 mm open bite still remained after 6 months of finalization with vertical and Class III intermaxillary elastics, with no further improvement. On discussion with the patient, a satisfactory result had been achieved so that the patient was debonded and fitted with vacuum-formed retainers (patient preference) (Figures 8 and 9). In all treatment lasted over 3 years.
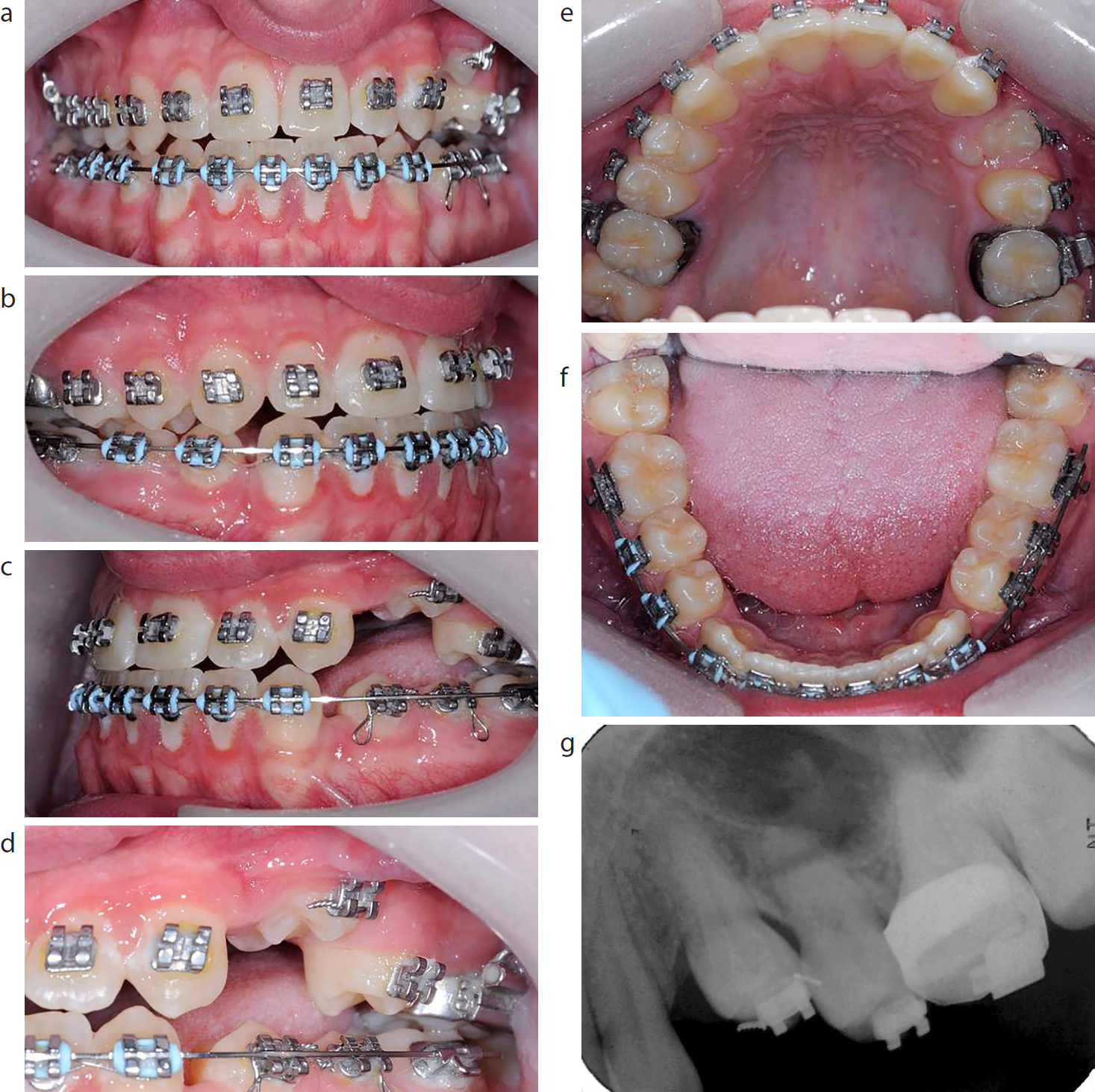
Figure 5. Six months into treatment.Figure 6.
(a–g) Eighteen months into treatment.Figure 7.
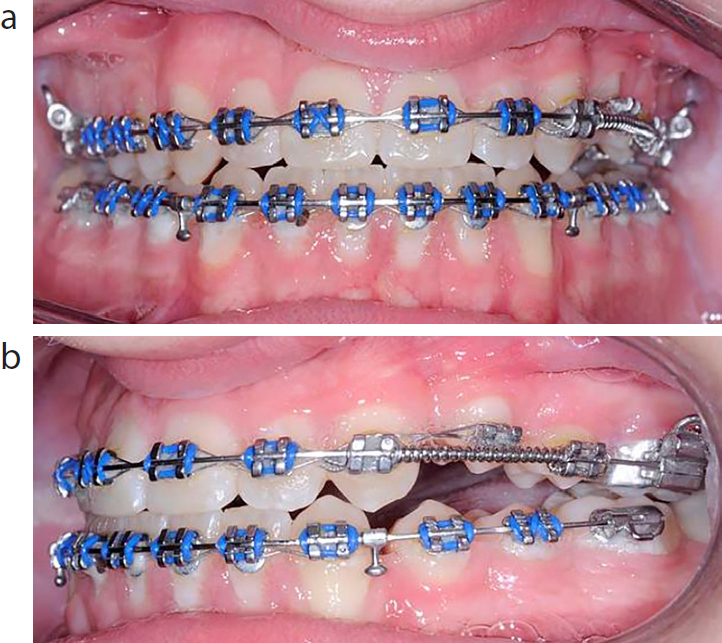
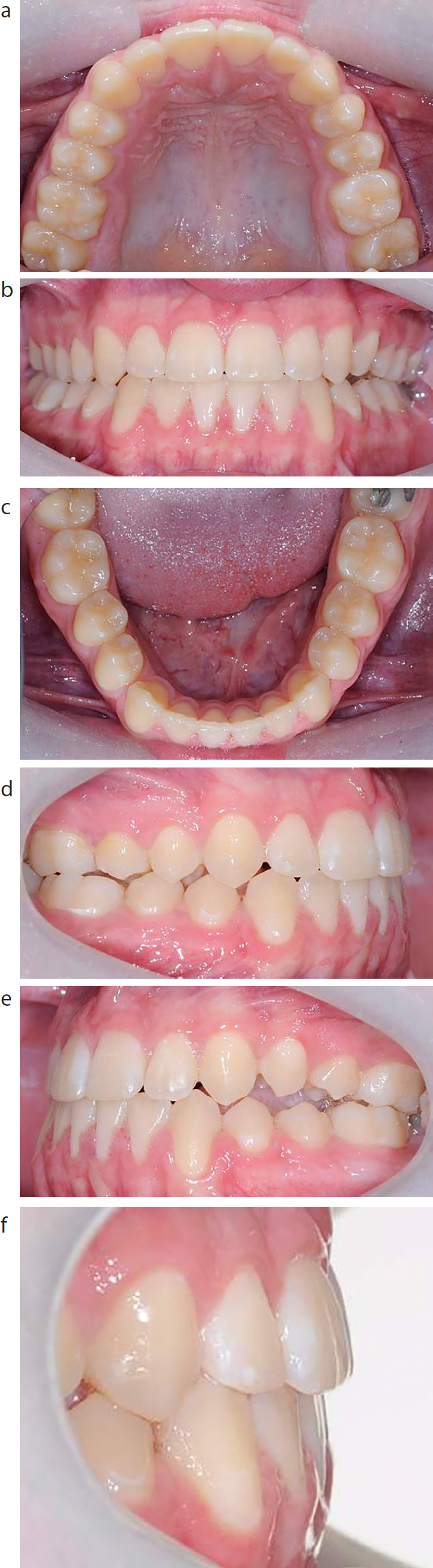
(a, b) Thirty months into treatment showing spontaneous movement of the UL4.Figure 8
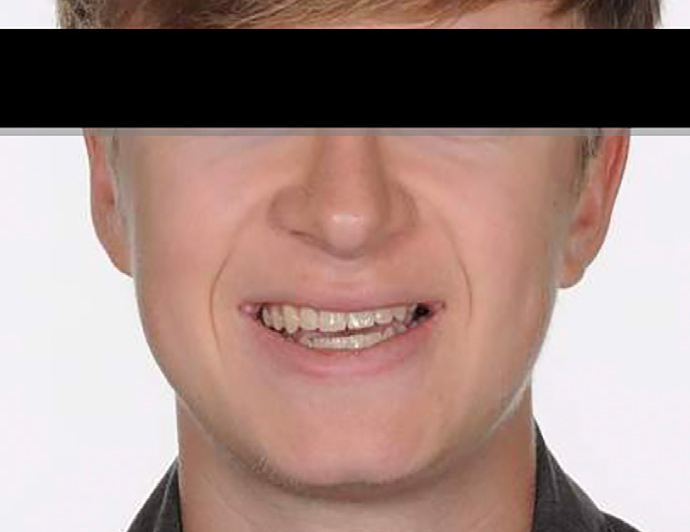
(a–f) Post-treatment intra-oral views.Figure 9. Post-treatment extra-oral view.
Outcome and follow-up
The patient's Peer Assessment Rating has changed from an initial 31 to 5, resulting in a greatly improved (84%) change. However, a small lateral open bite remained, and the levelling of the occlusion in the maxillary left quadrant shows that it is incomplete.
Discussion
This case highlights the difficulties of managing unerupted teeth. Whilst the incisor crossbite correction took place early in treatment, the vertical movement of the UL4 was intermittent and a slow process, resulting in 34 months of active treatment. It is fortunate that the patient maintained a good standard of oral hygiene and enthusiasm during his treatment with fixed appliances. It was a reasonable decision to discontinue treatment in view of the correction of the incisor relationship, the reduction of the lateral open bite to minimal levels and the duration of treatment. Initially, a diagnosis of a primary failure of eruption was considered.
Primary failure of eruption
Despite initial concerns of an impaction against a retained ULD root, there was failure to align the UL4 and achieve occlusal contact. A diagnosis of PFE is plausible as there was failure to align the tooth, even with adequate space, application of orthodontic forces and no obvious physical impaction. After application of orthodontic forces there appeared to be no periodontal ligament space and no lamina dura, indicating possible ankylosis. This case doesn't fall into a typical PFE case as the dentition posterior to the affected unit erupted normally.
Ankylosis
A diagnosis of ankylosis may appear most likely due to the radiographic findings of loss of periodontal ligament space and lamina dura, as well as failure to complete the levelling of the premolar. However, the apparent spontaneous movement later would disprove this. Ankylosis of the dentition has also been reported as a post-orthodontic finding associated with PFE. The post-treatment views appear to show an occlusal cant which was not observed pre-orthodontics. The only history relating to a possible cause of ankylosis was the extraction of infra-occluded ULDE. Ultimately the aetiology of the erratic behaviour of the UL4 eruption is unknown.
Conclusion
This case highlights the challenges and unpredictable nature of managing unerupted permanent teeth. Fortunately, a reasonable outcome was achieved and a reflection from the patient's perspective is shown below.
Patient perspective
‘My teeth used to be at an angle, not all my second teeth had come through and my upper teeth did not come in front of my lower teeth. My dentist referred me to orthodontics and I had a meeting with the consultant who X-rayed my teeth and it made it even more obvious there was a whole set of problems. I then met with Miss Nevard to plan what to do. The straightening process worked with braces and bands but I was a bit worried that surgery might have been needed as one of my second teeth would not move down. Several members of the orthodontic team debated what to do. Very surprisingly a tiny tooth fragment was stopping the other tooth moving and when that was removed they thought there was a remote chance it might solve the problem. Amazingly it did and that was good as it meant I didn't need an operation. The whole saga of my teeth has been going on for years and it was really good late last year to have my braces removed. My teeth are now straight, all through and I can bite properly and they look normal when I smile. Although I have had loads of visits over the years it has not been an issue as every time I went everyone was very friendly and a small amount of progress had occurred between visits. I am really please my dentist referred me to orthodontics at the John Radcliffe as it has meant that by the time I leave school my teeth will all be sorted out, look good and not give me any problems.’