O'Brien K, Wright J, Conboy F, Sanjie Y, Mandall N, Chadwick S Effectiveness of early orthodontic treatment with the Twin-block appliance: a multicenter, randomised, controlled trial. Part 1: Dental and skeletal effects. Am J Orthod Dentofacial Orthop. 2003; 124:234-243
Thiruvenkatachari B, Harrison J, Worthington H, O'Brien K. Early orthodontic treatment for Class II malocclusion reduces the chance of incisal trauma: results of a Cochrane systematic review. Am J Orthod Dentofacial Orthop. 2015; 148:47-59
Jadbinder S, Fleming PS, Newton T, DiBiase AT. Bullying in orthodontic patients and its relationship to malocclusion, self-esteem and oral health-related quality of life. J Orthod. 2011; 138:247-256
Spary DJ, Little RA. The simple Class II and Class III corrector: three case reports. J Orthod. 2015; 42:69-75
Little R, Spary DJ. A novel way of correcting Class II buccal segment occlusions. Ortho Update. 2014; 7:94-98
The early orthodontic management of a severe Class II division 1 malocclusion and its advantages are discussed. Two cases are described, both of which were successfully treated on a non-extraction basis, with a phase of functional appliance therapy followed by fixed appliances.
CPD/Clinical Relevance: The article outlines how, with careful case selection and early treatment, severe overjets can be successfully treated with orthodontics alone.
Article
Shayma Witwit
The treatment of children with severe Class II division 1 malocclusions presents a dilemma to the orthodontist. It is now believed that orthodontic appliances have a clinically significant effect in promoting forward mandibular growth.1 If the malocclusion is so severe that mandibular advancement surgery is a likely outcome, would early orthodontic treatment be putting the child through unnecessary therapy and complicating later treatment by reducing the overjet?
However, early treatment would seem to have some proven benefits such as the reduction of the risk of trauma to the anterior teeth2 and reduction of bullying during the period until the patient was old enough to have surgery.3 Providing teeth have not been extracted, the possibility of increasing the overjet and carrying out mandibular advancement surgery would still be an option.
Two cases are described where a very large overjet (over 15 mm) was successfully reduced without the need for extraction. The treatment involved a functional appliance phase using the simple Class II corrector (Button and Bead appliance), as described by Spary and Little,4 followed by fixed appliances. The conversion to fixed appliances can be a problem if pre-adjusted edgewise appliances, like the Straight-Wire Appliance®, are used. This is because the upper teeth are tipped distally during the functional appliance treatment, so that they will tend to move forwards as the upper teeth are aligned. Using Begg or Tip-Edge® brackets in the upper jaw prevents this proclination and the teeth can be uprighted later when anchorage can be supported by Class II elastics. This technique has been described by Little and Spary.5
Figure 1. (a) Case 1: Pre treatment profile.Figure 1. (b) Case 1: Pre-treatment overjet.Figure 1. (c) Case 1: Button and bead appliance phase.Figure 1. (d) Case 1: Fixed appliance phase.Figure 1. (e) Case 1: Post-treatment profile.Figure 1. (f) Case 1: Post-treatment.
Case JD was aged 11 years 3 months when the appliance was fitted. He had a Class II division 1 malocclusion on a severe skeletal II base with a reduced face height. The overjet was increased to 18 mm and the overbite increased and complete. The molar relationship was Class II on both sides.
The initial treatment was carried out with the ‘simple class II corrector’ (button and bead appliance). After 11 months the buccal segments were Class I and the overjet reduced to 4 mm. The fixed appliance phase of treatment used a lower pre-adjusted edgewise appliance. In the upper arch, Begg brackets were used to minimize forward movement in the early stages of fixed appliance treatment. The total treatment time was 3 years 1 month. Start and near-end of treatment cephalometric data are given in Table 1.
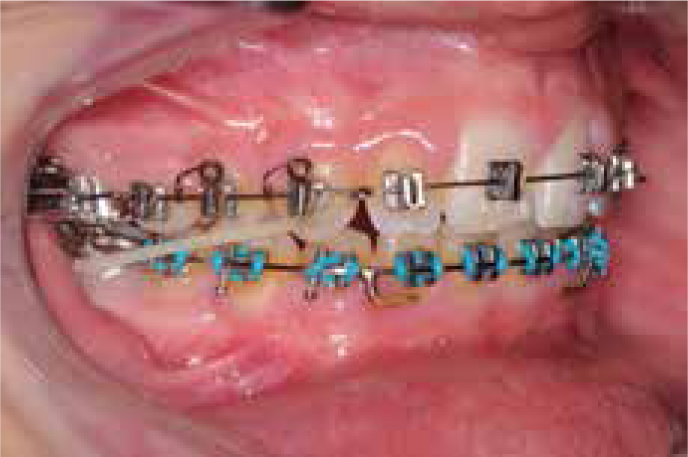
Figure 2. (a) Case 2: Pre-treatment profile.Figure 2. (b) Case 2: Pre-treatment overjet.Figure 2. (c) Case 2: Button and bead appliance phase.Figure 2. (d) Case 2: Fixed appliance phase.Figure 2. (e) Case 2: Post-treatment profile.Figure 2. (f) Case 2: Post-treatment.
Case AB was age 13 years 11 months when the appliance was fitted. He had a severe Class II division 1 malocclusion on a severe skeletal II base with a slightly reduced face height. The overjet was increased to 16 mm and the overbite was increased and complete; the molar relationship was Class II on both sides. The upper left canine was still unerupted. The simple Class II corrector was worn for 8 months until the buccal segments were corrected to a Class I relationship, the canine erupted and the fixed appliance phase of treatment could begin. A pre-adjusted edgewise appliance was used in the lower arch and Begg brackets in the upper arch. The total treatment time was 1 year and 7 months. Start and near-end of treatment cephalometric data are given in Table 2.
Start
Near-End
Norms
SD
SNA
84°
81°
81°
3.7°
SNB
76°
77°
78°
3.7°
ANB
8°
4°
3°
2.4°
Upper incisors
122°
115°
109°
5.4°
Lower incisors
90°
106°
93°
5.5°
Overjet
16 mm
2 mm
2 mm
Overbite
12 mm
2 mm
2 mm
Li to APo
-3 mm
+3 mm
1 mm
2 mm
FMPA
19°
20°
27°
4.9°
MMPA
25°
25°
27°
4.9°
Discussion
Proffit refers to the treatment of severe Class II division I malocclusions by orthodontics only as ‘camouflage treatment’.6 The inference is that this treatment is inferior to surgical correction. However, surgical correction is only possible after growth has completed. Early treatment has some advantages:
It reduces the risk of trauma to the anterior teeth;
It can have a significant psychological benefit at a vulnerable time;
It can reduce bullying at school;
In addition, there is no doubt that some patients are happy with the improvements in occlusion and facial profile that can be achieved with orthodontics only, especially if subsequent growth is favourable.
Because this treatment does not involve the extraction of teeth, except in cases of severe crowding, the option of surgical treatment at the completion of growth remains a possibility. At this stage, lower first premolars can be removed and the fixed appliances placed to increase the overjet to the correct value to allow mandibular advancement surgery.
Notes on the simple Class II corrector (Button and bead appliance)
This appliance consists of separate upper and lower splints made of vacuum pressure-formed material with a bead on the disto-palatal cusps of the upper first molars. The bead bites behind the occlusal table on the lower splint which postures the mandible forwards. A second splint with the bead on the mesio-palatal cusp can be used after 6 weeks to over-correct the buccal segments.
The buttons, or other attachments, are placed on the upper lateral incisors and lower first molars, allowing Class II inter-maxillary elastics to be used throughout the treatment. This ensures that the appliance remains active during sleeping and speech when other functional appliances are inactive. A help sheet for this appliance is available on the internet.7