Kane G, Cash A, Seehra J. Pre-eruptive coronal resorption of unerupted molar teeth in orthodontic patients. J Orthod. 2019; 46:155-161
Seow WK, Lu PC, McAllan LH. Prevalence of pre-eruptive intracoronal dentin defects from panoramic radiographs. Pediatr Dent. 1999; 21:332-339
Seow WK, Wan A, McAllan LH. The prevalence of pre-eruptive dentin radiolucencies in the permanent dentition. Pediatr Dent. 1999; 21:26-33
Demirtas O, Tarim Ertas E, Dane A Evaluation of pre-eruptive intracoronal resorption on cone-beam computed tomography: a retrospective study. Scanning. 2016; 38:442-447
Seow WK, Hackley D. Pre-eruptive resorption of dentin in the primary and permanent dentitions: case reports and literature review. Pediatr Dent. 1996; 18:67-71
Kjær I, Steiniche K, Kortegaard U Preeruptive intracoronal resorption observed in 13 patients. Am J Orthod Dentofacial Orthop. 2012; 142:129-132
Brooks JK. An unusual case of idiopathic internal root resorption beginning in an unerupted permanent tooth. J Endod. 1986; 12:309-310
Brunet-Llobet L, Lahor-Soler E, Miranda-Rius J. Oral pain due to severe pre-eruptive intracoronal resorption in permanent tooth. Eur J Paediatr Dent. 2014; 15:332-334
Davidovich E, Kreiner B, Peretz B. Treatment of severe pre-eruptive intracoronal resorption of a permanent second molar. Pediatr Dent. 2005; 27:74-77
De Souza NJD, Gopakumar MR, Hegde AM, Kumar J. Pre-eruptive intra coronal lesions revisited: report of two rare cases and their treatment. Int J Contemp Med Res. 2017; 4:25-27
Ignelzi MA, Fields HW, White RP, Bergenholtz G, Booth FA. Intracoronal radiolucencies within unerupted teeth. Case report and review of literature. Oral Surg Oral Med Oral Pathol. 1990; 70:214-20
Klambani M, Lussi A, Ruf S. Radiolucent lesion of an unerupted mandibular molar. Am J Orthod Dentofacial Orthop. 2005; 127:67-71
McNamara CM, Foley T, O'Sullivan VR External resorption presenting as an intracoronal radiolucent lesion in a pre-eruptive tooth. Oral Dis. 1997; 3:199-201
O'Neal KM, Gound TG, Cohen DM. Preeruptive idiopathic coronal resorption: a case report. J Endod. 1997; 23:58-59
Rankow H, Croll TP, Miller AS. Preeruptive idiopathic coronal resorption of permanent teeth in children. J Endod. 1986; 12:36-39
Yamada MKM, Taguchi Y, Watanabe J, Noda T. Preeruptive intracoronal radiolucency caused by resorption: report of a case. Eur J Paediatr Dent. 2012; 2:79-82
Wong L, Khan S. Occult caries or pre-eruptive intracoronal resorption? A chance finding on a radiograph. Pediatr Dent. 2014; 36:429-432
Blackwood HJ. Resorption of enamel and dentine in the unerupted tooth. Oral Surg Oral Med Oral Pathol. 1958; 11:79-85
Seow WK. Pre-eruptive intracoronal resorption as an entity of occult caries. Pediatr Dent. 2000; 22:370-376
Holan G, Eidelman E, Mass E. Pre-eruptive coronal resorption of permanent teeth: report of three cases and their treatments. Pediatr Dent. 1994; 16:373-377
Manmontri C, Mahasantipiya PM, Chompu-Inwai P. Preeruptive intracoronal radiolucencies: detection and nine years monitoring with a series of dental radiographs. Case Rep Dent. 2017; 2017
Manan NM, Mallineni SK, King NM. Case report: idiopathic pre-eruptive coronal resorption of a maxillary permanent canine. Eur Arch Paediatr Dent. 2012; 13:98-101
Dowling PA, Fleming P, Corcoran F. A case report of pre-eruptive coronal resorption in a mandibular canine. Dent Update. 1999; 26:444-445
Azaz B, Shteyer A. Resorption of the crown in impacted maxillary canine. A clinical, radiographic and histologic study. Int J Oral Surg. 1978; 7:167-171
Wood PF, Crozier DS. Radiolucent lesions resembling caries in the dentine of permanent teeth. A report of sixteen cases. Aust Dent J. 1985; 30:169-173
Becker A, Abramovitz I, Chaushu S. Failure of treatment of impacted canines associated with invasive cervical root resorption. Angle Orthod. 2013; 83:870-876 https://doi.org/10.2319/090812-716.1
Heithersay GS. Invasive cervical resorption. Endod Topics. 2004; 7:73-92
Heithersay GS. Invasive cervical resorption following trauma. Aust Endod J. 1999; 25:79-85
Heithersay GS. Clinical, radiologic, and histopathologic features of invasive cervical resorption. Quintessence Int. 1999; 30:27-37
Kindelan SA, Day PF, Kindelan JD Dental trauma: an overview of its influence on the management of orthodontic treatment. Part 1. J Orthod. 2008; 35:68-78
Batista KB, Thiruvenkatachari B, Harrison JE, O'Brien KD. Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children and adolescents. Cochrane Database Syst Rev. 2018; 3
Two case reports are described along with differential diagnoses and management strategies from the literature for teeth discovered with intra-coronal resorption prior to their eruption. Our cases feature impacted maxillary anterior teeth. In both instances, significant coronal resorption presented itself mid-way through fixed appliance treatment, prior to full eruption of the involved teeth. This was detected radiographically and not through patient-reported symptoms. Once sufficiently erupted, root canal therapy was carried out in both cases and orthodontic treatment was successfully completed.
CPD/Clinical Relevance: Orthodontists are often first to identify pathological lesions in unerupted teeth and should be equipped with differential diagnoses in order to manage and refer patients appropriately.
Article
Coronal radiolucencies identified on radiographs of permanent teeth are mostly attributable to demineralization, hypomineralization or hypoplasia.1 Internal resorption, following dental trauma, can also appear as a radiolucency within the crown. A comprehensive history and clinical examination will help to determine the aetiology of the pathology so that the tooth can be managed correctly. But what if the crown of an unerupted tooth is found by chance to be afflicted with a resorptive lesion where the patient is often not able to offer a history? The aetiology, diagnosis and management become more difficult.
Orthodontic patients are carefully examined for the absence of dento-alveolar pathology and the presence of normal crown and root development prior to commencing treatment. In the two cases described below, the involved unerupted anterior teeth demonstrated normal radiographic development and orthodontic treatment was started. Mid-treatment, coronal radiolucencies were observed on progress radiographs and, at the time, the aetiology was assumed to be idiopathic resorption. Idiopathic coronal resorption of an unerupted tooth has historically often been misdiagnosed as occult caries.1 Many terms have been coined for it in the past, the very first of which was ‘intrafollicular caries’.1,2,3 Now, it is most commonly referred to as ‘pre-eruptive intra-coronal resorption’ (PIR).4,5
Owing to the frequent misdiagnosis of PIR, and the varying radiographic techniques employed in different studies to investigate PIR, its prevalence is difficult to pinpoint. It has been estimated as 0.5% for tooth prevalence and 3% for subject prevalence.6,7 It is rare for more than one tooth to be affected in the same individual.8 There has only been one report of PIR in the deciduous dentition, but this was not a conventional presentation.9 It has been largely suggested that PIR is found only in permanent teeth; perhaps this is simply because fewer dental radiographs are carried out in young patients in the primary dentition. The most commonly affected permanent teeth are molars and premolars.1,2,4,5,6,7,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25 The mandibular second molar appears to be the tooth most affected by pre-eruptive intra-coronal resorption.4,6,10,12,13,16 Most, if not all of the cases of PIR reported in the literature affect young and medically fit patients with no predilection for a particular patient group.5
Case 1: maxillary canine
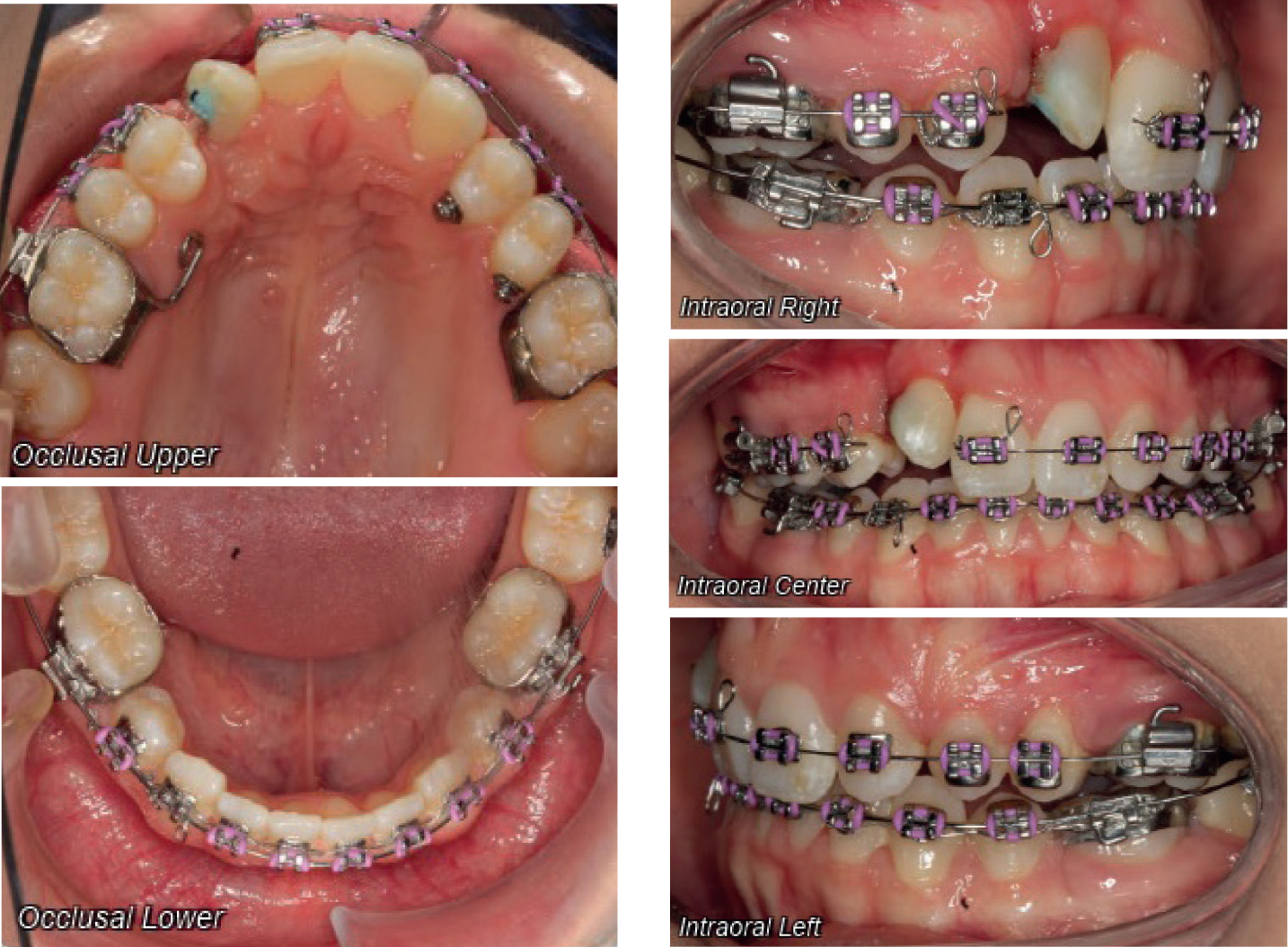
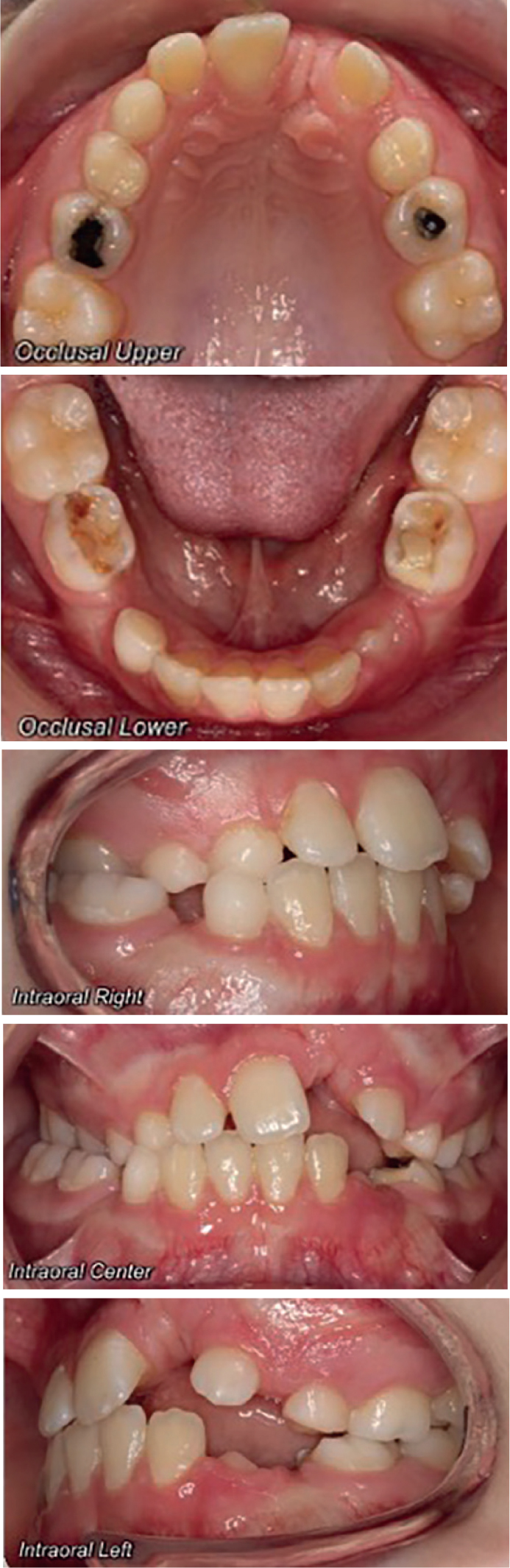
A medically fit and well 17-year-old female was referred to the orthodontic department at Royal Derby Hospital by her general dental practitioner (GDP) for assessment of missing UR2, UL2 and UR3. She presented with a Class III incisor relationship on a mild Class III skeletal base with average vertical dimensions. This was complicated by developmental absence of UR2 and UL2, palatal impaction of UR3, retained URC (between UR1 and UR4) and ULC (between UL3 and UL4). The lower arch was mildly crowded with a retroclined lower labial segment, the upper arch was aligned and at an average inclination. The overjet and overbite were minimal and there was a 3-mm upper centreline shift to the right. Crossbites affected URC and UL5 and molar relationships were ¼ unit II on the right and Class I on the left (Figure 1). The IOTN was 5i.
Radiographic investigation confirmed hypodontia of UR2 and UL2, palatally impacted UR3 in sector V, and shortened roots of URC and ULC (Figure 2). Treatment options included:
Accept the existing malocclusion;
Surgical removal of UR3 and accept the malocclusion;
Expose and bond (E&B) UR3, extract URC and align upper arch only using a transpalatal arch (TPA) and upper fixed appliance. This would involve accepting the upper centreline discrepancy and the need for long-term replacement of ULC when required;
E&B UR3, extract URC, ULC, LR5, LL5 and align using a TPA and upper and lower fixed appliances to correct the centrelines and improve the overjet and overbite.
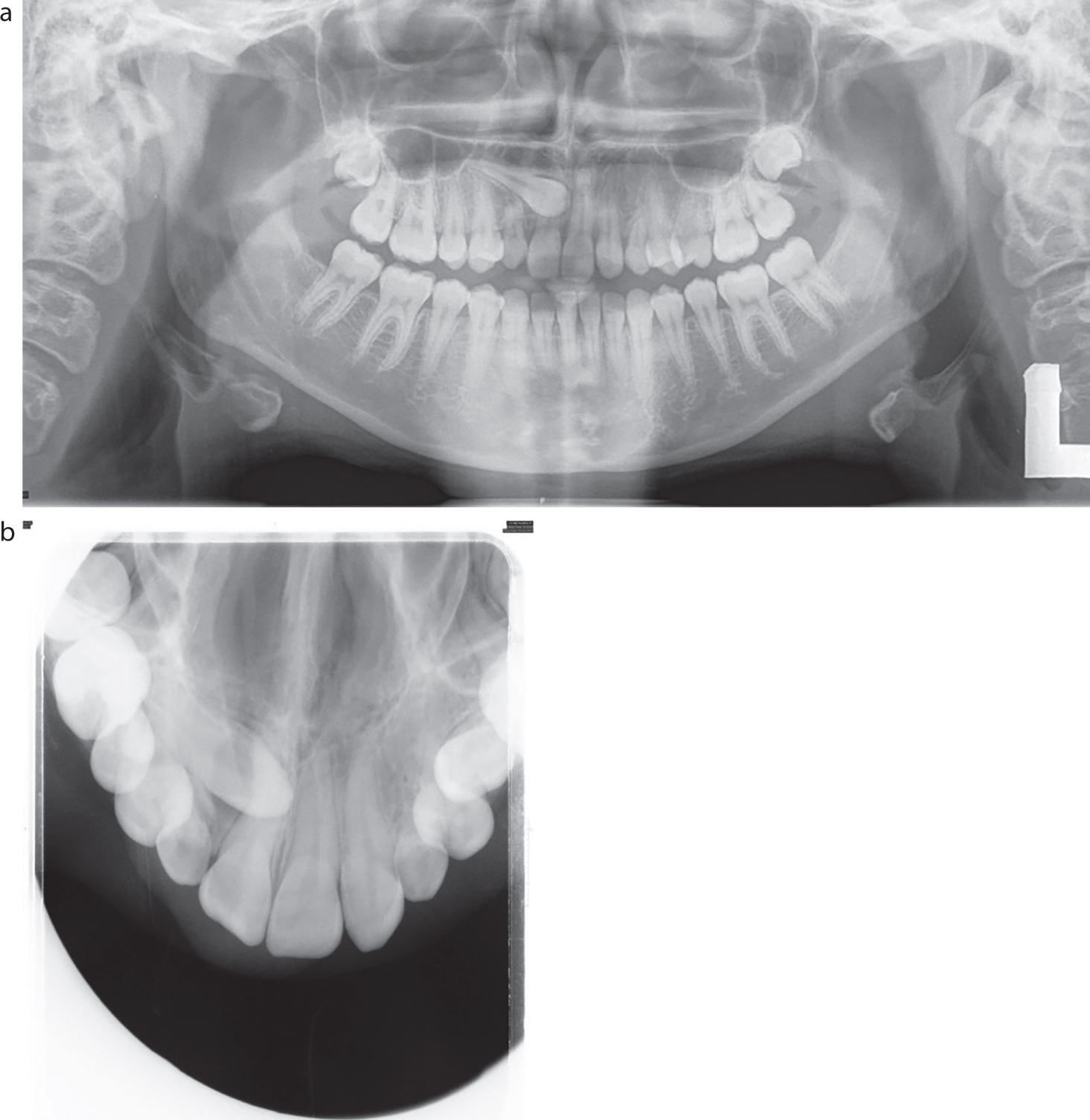
Figure 2.
(a) Baseline OPG and (b) USO. Root development complete UR3.
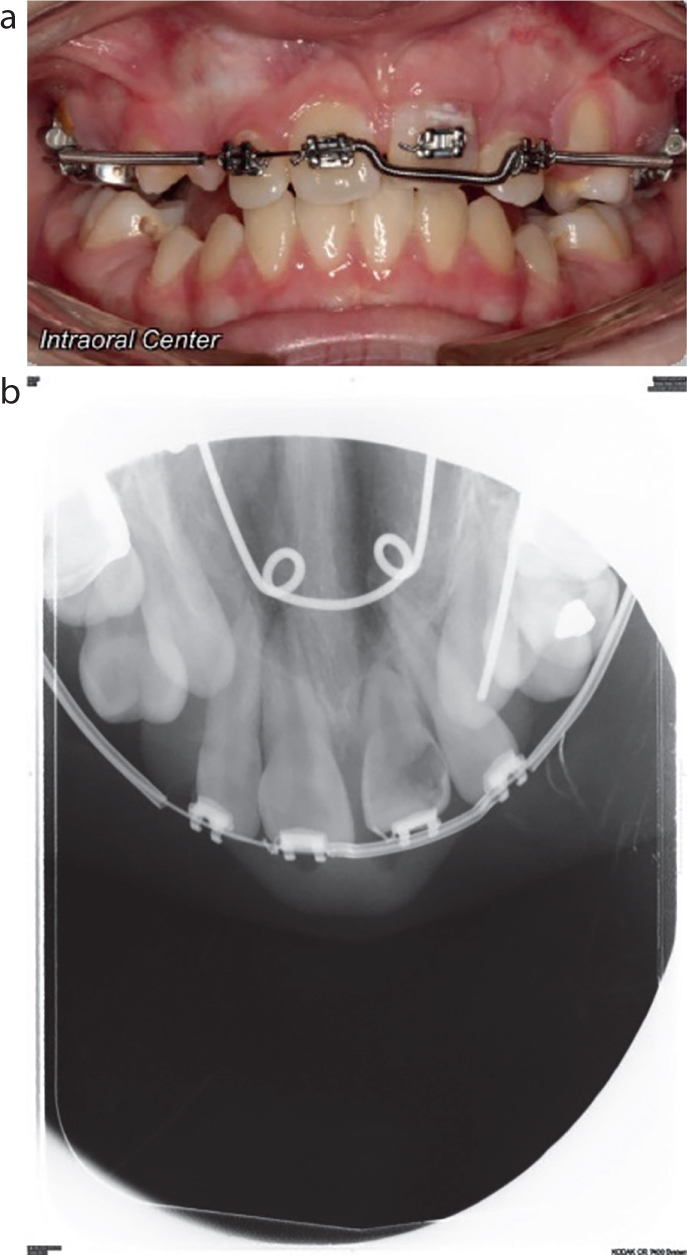
The patient wanted comprehensive orthodontic treatment (option 4) and a closed exposure of UR3 was carried out. Alignment of UR3 was slow, with partial eruption after 2 years of traction. An OPG revealed an unexpected finding: a well-defined coronal radiolucency in the UR3 occupying 50% of the crown width. A supplemental peri-apical radiograph of UR3 confirmed a radiolucency approaching the pulp chamber and widening of the periodontal ligament (Figure 3). Clinically, a cavity could not be detected at this point. The surrounding gingivae was normal and healthy. The patient also reported no symptoms from UR3.
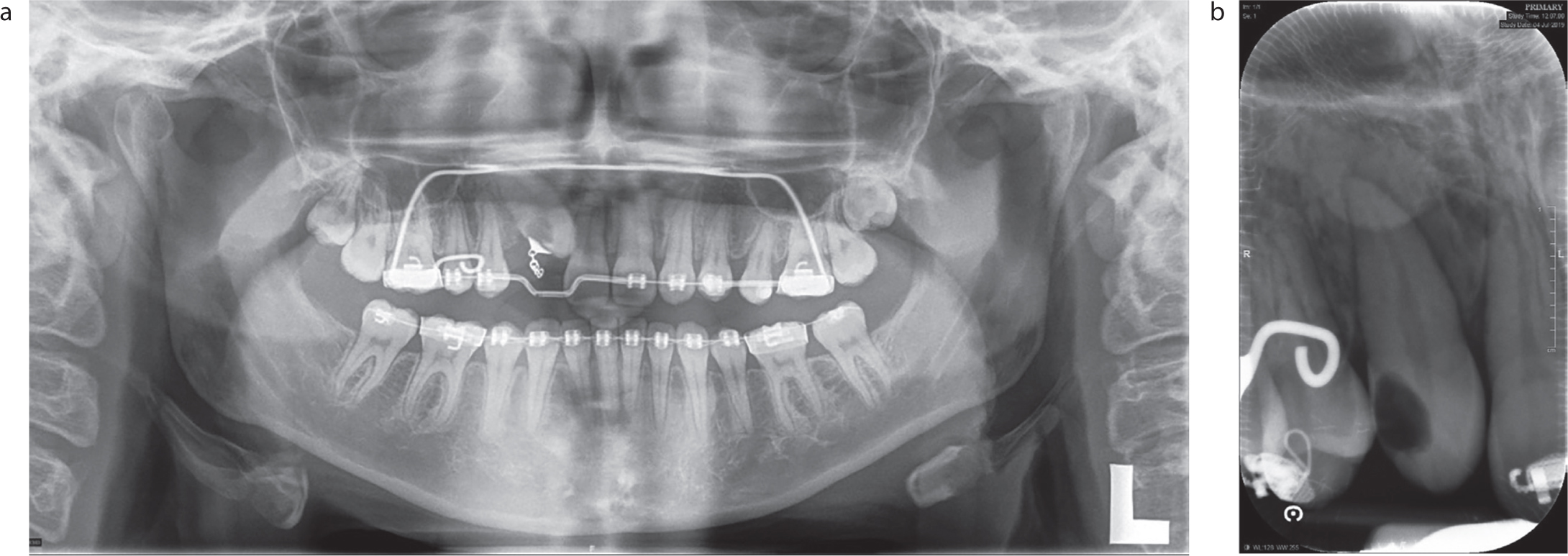
Figure 3. Mid-treatment (a) OPG and (b) peri-apical of UR3.
An apically repositioned flap of UR3, followed by light extrusive forces, allow better visual assessment of the tooth. A cavitated lesion with softened dentine on the disto-palatal aspect of UR3 was observed (Figure 4). The tooth was dressed and sealed temporarily in the orthodontic clinic and the patient referred back to the GDP for root canal treatment. Six months later, in the absence of clinical or radiographic signs of pathology, continued alignment of UR3 was resumed. Figure 5 shows the occlusion after debond.
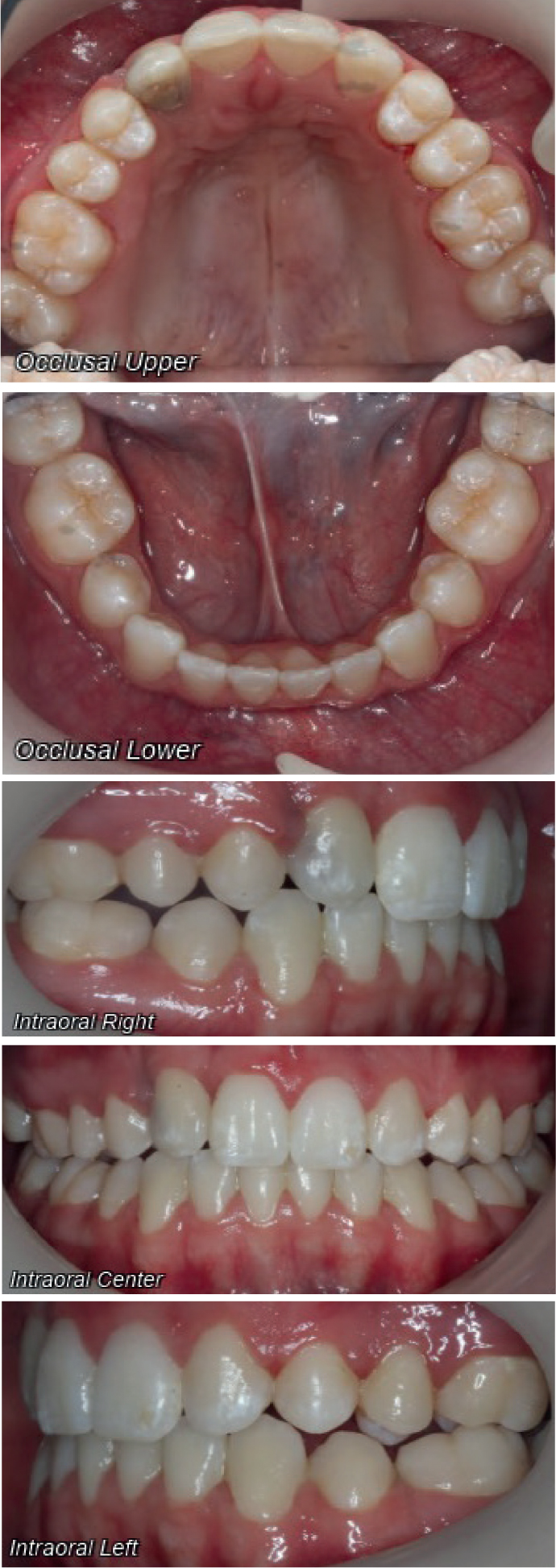
Figure 4. Clinical appearance of UR3 once erupted and temporarily dressed.Figure 5. The occlusion after debond.
Case 2: maxillary incisor
A medically fit and well girl aged 10 years and 4 months was referred to the orthodontic department by her GDP for assessment of missing UL1. There was a vague history of trauma to both primary central incisors aged 4, but both deciduous central incisors had been removed shortly after the event.
She presented with a Class I incisor relationship on a Class I skeletal base with reduced vertical proportions and mandibular asymmetry of the chin point to the right side. She presented in the early mixed dentition. The lower arch was well aligned and the lower labial segment at an average inclination. The upper arch showed potential moderate crowding with proclined incisors, an unerupted UL1 and buccally palpable unerupted canines. Overjet was 2 mm on UR1 and the overbite was reduced and complete to tooth. The upper centreline was to the left of the facial midline by 4 mm and the lower to the right by 3 mm. Initial contact on URC had a resulting forward slide to the right into ICP resulting in crossbite of URCDE6. Molar relationships were ½ unit II on the right and Class I on the left (Figure 6). IOTN was 5i.
Radiographs confirmed a full complement of teeth, including the unerupted UL1 and vertical bone loss in this region. Vertical height assessment showed the UL1 crown tip was situated halfway up the UL2 root. Most importantly, the UL1 showed a normal appearance of the crown and root (Figure 7) and was deemed feasible to align.
Figure 7. Baseline (a) OPG and (b) USO. Root development complete UL1.
The first stage of active treatment included removal of all remaining deciduous teeth and an apically repositioned flap with attachment of a gold chain to the labial surface of UL1 under general anaesthesia. A few weeks later, the second stage was the placement of a quadhelix and a 2x4 sectional fixed appliance on the UR21 UL2. Once a sufficient amount of the UL1 crown was visible, the tooth was bonded and gently extruded with powerchain to allow subsequent piggyback mechanics. Within 2 months of applying traction to UL1, the emerging clinical crown revealed a worrying appearance: the disto-gingival corner of the labial crown was diffusely pink with an overlying white opacity (Figure 8). No enamel cavitation was noted to suggest that this was a typical carious process. Upon further questioning, the patient admitted recent pain from UL1. An upper standard occlusal (USO) showed a distal radiolucency extending on to the pulp chamber, which again at the time was initially believed to be PIR.
Figure 8. Mid-treatment (a) photograph of UL1 and (b) USO.
On that visit, the patient was informed of the pathology and the archwire was removed from the fixed appliance. A specialist restorative opinion was sought from University Hospitals of Leicester where root canal treatment was carried out. During root treatment, the UL1 demonstrated eggshell thin labial enamel and on exposure of the pulp chamber, a snail track lesion was found extending down onto the root. This was sealed uneventfully following the root filling.
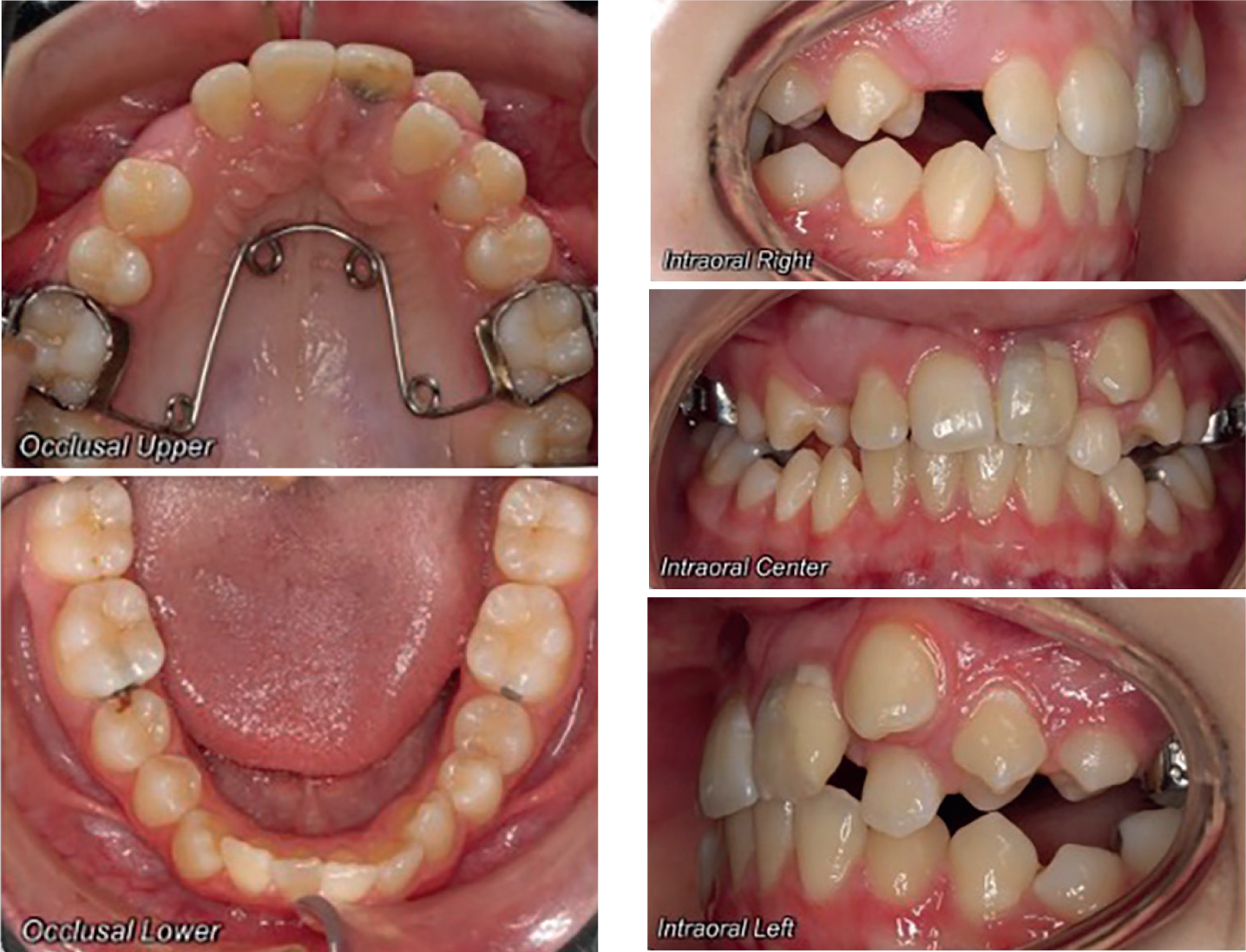
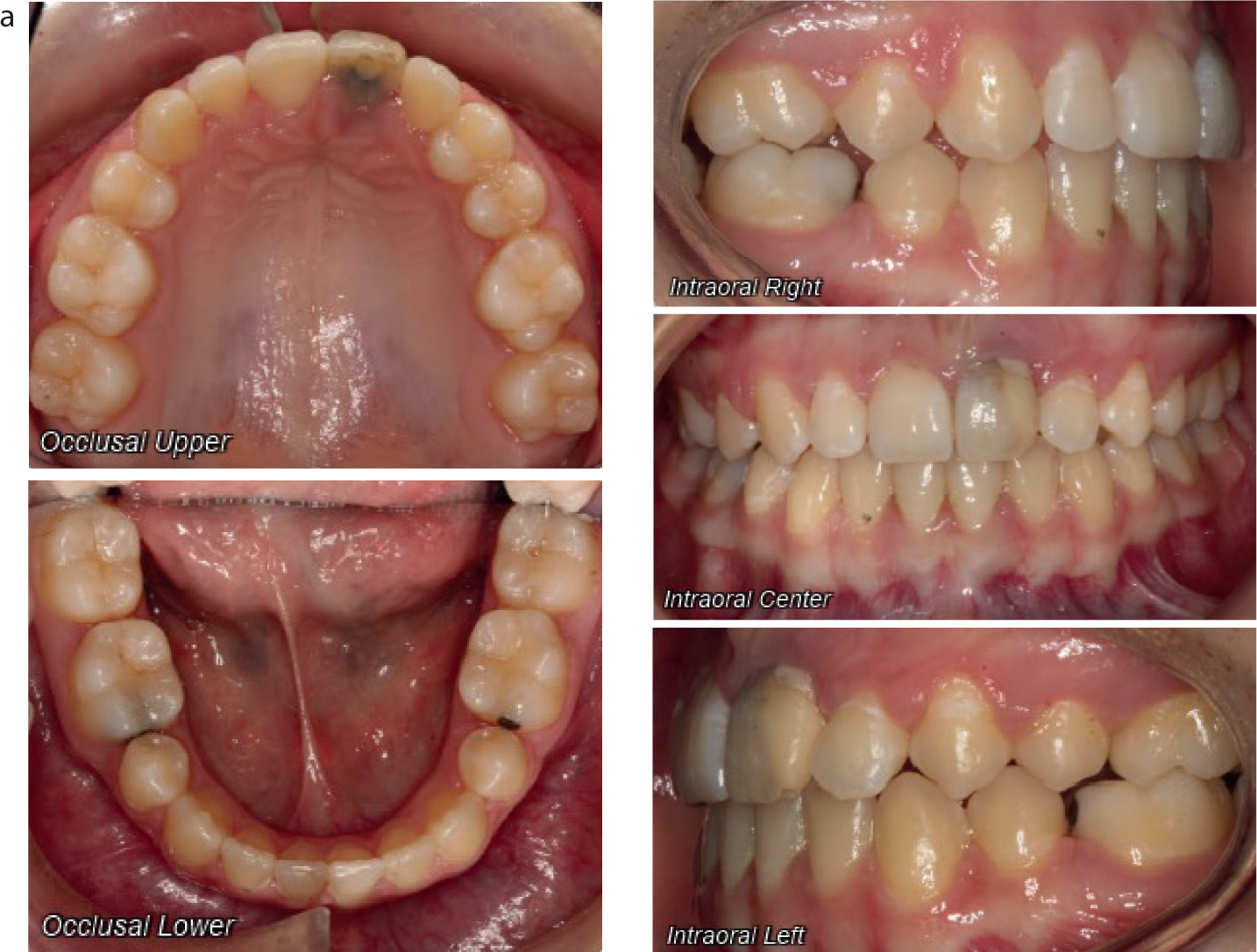
The patient returned to the orthodontic department 9 months later, aged 12 years and 6 months, in the permanent dentition with a fully erupted UL1. Pertinent features of her malocclusion included: a buccally excluded UL3 and severe crowding in the upper arch, mild crowding in the lower arch, Class I incisor and molar relationships bilaterally and a reduced overbite (Figure 9). An extraction pattern of LR5, LL5, UR5 and UL3 was agreed and fixed appliance treatment was re-commenced. The patient has been de-bonded and would like to improve the colour of the darkened UL1 (Figure 10).
Figure 9. The occlusion following RCT UL1.Figure 10. Post-debond photographs.
Discussion
Case 1 and pre-eruptive intra-coronal resorption
An unerupted tooth that is not directly exposed to the oral cavity is not at risk of the usual pathological processes that result in surface demineralization. In the presence of both a caries-favouring oral environment and a non-cleansable periodontal pocket associated with an unerupted tooth, it could be argued that demineralization could take place. However, the development of primary caries in an unerupted tooth has yet to be proven.15,18 This makes it feature quite low down on the differential diagnosis list for Case 1 (Table 1). The insidious nature of PIR reported in the literature is highly reflective of the clinical and radiographic presentation of the UR3 in Case 1. Even though PIR has largely been reported in unerupted molars and premolars, a few reports highlight that the condition does not spare impacted canines.10,19,26,27,28 Furthermore, PIR has been associated with anomalies in the dentition, such as hypodontia. In this case, the patient presented with an impacted UR3 and developmentally absent maxillary laterals.29
Differential diagnosis
Reasoning
Likelihood
PIR
Incidental radiographic finding resembling caries close to the pulp, no suspicion of cariogenic micro-organism activity, clinically asymptomatic
High
Primary caries
Low caries risk/experience in the remainder of the dentitionComplete coverage of the crown by healthy soft tissueNo periodontal pocket to allow bacterial ingress
Low
Turner's tooth
The preceding URC was sound, no root fragments were retained following its extraction
Low
Iatrogenic
SurgicalDirect damage from the bur on a surgical hand piece during bone removal intra-operatively – not in keeping with radiographic appearance of radiolucencyOrthodonticExcessive orthodontic force can cause root resorption, but not much evidence to link it to intra-coronal resorption Inappropriate extrusion mechanics were not used
Low
Invasive cervical root resorption
Secondary to impaction/trauma of the surgical exposure/subsequent orthodontic tractionRoot unaffected, resorption was limited to the dentinal crown
Low
During dental development, the reduced enamel epithelium covers the crown of an unerupted tooth and protects it. It also separates it from the adjacent dental follicle, which contains vascular mesodermal tissue. This epithelial layer protects the enamel of an unerupted tooth from invasion by the nearby vascular channels within the connective tissue. Blackwood suggested that a breach in the reduced enamel epithelium followed by subsequent abnormal contact of the enamel with connective tissue leads to disruption in normal crown development and is believed to be the pathogenesis behind PIR.9,18,22
An alternative pathogenesis for PIR was described by Seow: an ectopically positioned tooth may experience heightened localized pressure against the surface of the crown, precipitating resorption to ensue. This is thought to be mediated by resorption-inducing cells entering the dentine via enamel fissures or the cemento-enamel junction.6,7,8,23 Azaz and Shteyer speculated damage at the level of the enamel and not the cemento-enamel junction as the starting point for resorption in impacted canines.28 This is possible if the protective epithelium overlying the enamel of an unerupted tooth is destroyed, possibly by a local factor which then induces an inflammatory process.19
Similar to our management in Case 1, once a coronal radiolucency lesion has been identified in an unerupted tooth, many authors have advocated surgical exposure of the affected tooth with a view to gaining faster visual access, limiting the pathological process and conserving the tooth.6,10,18,23,26 However, after a certain point, PIR is not a fast progressing lesion, unlike dental caries.22 Interestingly, many papers evidence a lack of progression into the pulpal chamber. Despite extensive coronal resorption seen in PIR of unerupted teeth, pulpal infection does not occur at a histological level.6,7,9,16,21,22
Cases in which poor-prognosis teeth have been extracted and examined under a microscope, unanimously describe a normal layer of dentine between the pulp and the resorptive lesion, with absence of pulpal inflammation and minimal secondary dentine deposition.9,15,16,17, 19, 20,22,25 The histological picture of PIR is strikingly different to that of dental caries: spindle-shaped fibroblasts, multi-nucleated giant cells and vascular connective tissue occupy the resorptive lesion. The epithelium, in areas of its deficiency, is often found to be replaced by multinucleated osteocytes thought to be responsible for the resorption.9,17,20,22 Cross-contamination with oral microflora clouds the true presentation of a PIR lesion at a cellular level.16
In contrast to extracted teeth due to PIR, many papers have shown that affected teeth are not all destined for removal and can be retained with early interception and appropriate restorative procedures.2,4,20,25 Pulpal regenerative techniques have been employed where possible,5,10,13,14,15,18,20,22 with some reports of very conservative management. This includes treating relatively large molar PIR lesions as fissure caries, sealing occlusal surfaces and monitoring closely long term,25 while another example includes direct pulp capping,2 and indirect pulp capping and restoration.4 Indeed, many cases from the paediatric literature place emphasis on careful curettage and pulpotomy, with successful short-term follow ups reported in scenarios where the pulp is believed not to have been directly affected.4 The most common restorative treatment modality appears to be either a calcium hydroxide lining or zinc-oxide eugenol base cement followed by a definitive restoration.2,4,9,13,20
In our case, the UR3 underwent root canal treatment by the GDP, a reasonable treatment approach towards suspected pulpal involvement in a permanent tooth in a patient who was an adult at that point. Historically, prompt endodontic treatment was advocated because lesions were usually discovered or made accessible once the radiographic coronal radiolucencies had become significantly large.11,27 However, after a certain stage, progression can be minimal or arrest altogether.22 More recent reports have shown clinicians preferring to monitor PIR lesions for several years by adopting a protocol of delayed restorative treatment given the newly identified, slowly progressive nature.4,25 Nonetheless, pulp regeneration is critical in teeth with immature apex formation because normal root development is desired. It can be argued that a tooth affected by PIR that achieves normal continued root development is more desirable than attempting to sustain pulp vitality in an affected tooth, particularly in the presence of hypodontia or premature loss of other teeth. Early and urgent referral by the orthodontist to a paediatric or restorative department will allow maximal chance of obtaining apexification; however, the literature seems to show that PIR-involved teeth continue to show normal and full root development.2 It is worth noting that the canine and incisor described in our cases both showed completed root apexification before appearance of the coronal lesion, and referral to the GDP was deemed appropriate in Case 1.
Case 2 and invasive cervical root resorption
Both cases in this report involved impacted teeth, but it is suspected that the aetiology in Case 2 is different given the history of dental trauma. The involved tooth in Case 2 was beginning to cause intermittent pain unlike Case 1 in which the impacted UR3 remained asymptomatic despite demonstrating a larger radiolucency closer to the pulp. This suggests the pathogenic process was different in each. It could be that the UL1 had erupted more, and symptoms may have occurred as the pulpal tissue was exposed to the oral environment.
Table 2 considers possible diagnoses for Case 2, for which invasive cervical root resorption (ICRR) seems most likely. Hiethersay and Becker et al have described this form of external root resorption as rare, insidious and aggressive.30,31 Orthodontics, closely followed by trauma were the most likely predisposing factors in the onset of ICRR.31,32 It begins as a focal resorptive point in the cervical area under the epithelial attachment and spreads inwards to dentine both coronally and apically.32,33 Heithersay also described a pink discolouration at the gingival margin is a tell-tell sign of ICRR.33
Differential diagnosis
Reasoning
Likelihood
ICRR
Secondary to previous dental trauma in the primary dentition aged 4 yearsPink discolouration of clinical crownThe radiographic coronal radiolucency extended onto the root when examined clinically
High
PIR
Secondary to previous dental trauma or secondary to impaction
High
Primary caries
Low caries risk/experience in the remainder of the dentitionComplete coverage of the crown by healthy soft tissueNo periodontal pocket to allow bacterial ingress detected
Low
Turner's tooth
Secondary to possible peri-apical inflammation from the traumatized deciduous maxillary incisor, but no record of this
Low
Iatrogenic
OrthodonticExcessive orthodontic force can cause root resorption, but not much evidence to link it to intra-coronal resorptionInappropriate extrusion mechanics were not used
Low
Typically, it does not traverse into the pulp quickly and allows the tooth to remain asymptomatic while significant dentinal destruction takes place.30 Symptoms arise only in the presence of pulpal or periodontal involvement, as seen in the female patient in Case 2.33 The pathogenesis has been described as damage to the cementum at the cemento-enamel junction with subsequent exposure of the underlying dentine. Osteoclastic cells are signalled towards the dentine and initiate resorption.30 A classification system (class I–IV) based on severity of the lesion has been described to provide a clinical guide for practitioners, serve as a research tool and to help assign either non-surgical or surgical treatment accordingly.31 ICRR is relatively uncommon, but is often mistaken as a form of internal root resorption when in reality it takes place external to the root surface.10,31
It is difficult to pinpoint whether the trauma directly affected the development of the UL1 and resulted in coronal resorption, or whether it was the subsequent physical impaction of the UL1 that led to coronal resorption of the crown. The Children's Dental Health Survey 2013, revealed that 12% of 12-year olds in the UK had experienced traumatic damage to their maxillary permanent incisors by that age, reducing to a lower incidence of 10% in 15-year olds.34 The likelihood of dental trauma in young people is often correlated with skeletal sagittal discrepancies, that is children with a retrognathic mandible, a class II skeletal pattern and proclined maxillary incisors.35,36 Less commonly considered than the position of the teeth in the antero-posterior plane as a risk factor in dental trauma is the impact of a discrepancy in vertical face height.
A reduced vertical dimension may have been an important contributory factor for the prognosis of the UL1 following the trauma in Case 2. A relatively short height of the maxilla would imply that the developing UL1 was lying in relatively closer proximity to the root of the traumatized deciduous incisors within the anterior maxilla at the time of the trauma aged 4 years. Theoretically, there may have been greater chance of the developing permanent central incisor being adversely affected to a greater extent than compared to a patient with average or increased vertical dimensions.
Conclusion
Unerupted teeth with lesions resembling PIR or ICRR are often discovered as an incidental finding on OPG, USO or bitewing radiographs by orthodontists. There seems to be a predilection for impacted teeth.
Lesions can remain asymptomatic despite extensive coronal destruction. Therefore, orthodontists should carefully monitor those teeth to which orthodontic traction is applied.
Not all unerupted affected teeth require immediate intervention with surgical exposure once lesions have been identified. Treatment strategies should be formed on a case-by-case basis depending on the extent of the radiographic lesion and clinical symptoms.