Taylor G, McNeill A, Girling A Change in mental health after smoking cessation: systematic review and meta-analysis. BMJ. 2014; 348 https://doi.org/10.1136/bmj.g1151
Chaffee BW, Couch ET, Vora MV, Holliday RS Oral and periodontal implications of tobacco and nicotine products. Periodontol 2000. 2021; 87:241-253 https://doi.org/10.1111/prd.12395
Li Y, Jacox LA, Little SH, Ko CC Orthodontic tooth movement: the biology and clinical implications. Kaohsiung J Med Sci. 2018; 34:207-214 https://doi.org/10.1016/j.kjms.2018.01.007
Bakathir MA, Linjawi AI, Omar SS Effects of nicotine on bone during orthodontic tooth movement in male rats. Histological and immunohistochemical study. Saudi Med J. 2016; 37:1127-1135 https://doi.org/10.15537/smj.2016.10.15159
Sodagar A, Donyavi Z, Arab S, Kharrazifard MJ Effect of nicotine on orthodontic tooth movement in rats. Am J Orthod Dentofacial Orthop. 2011; 139:e261-e265 https://doi.org/10.1016/j.ajodo.2010.08.018
Kirschneck C, Bauer M, Gubernator J Comparative assessment of mouse models for experimental orthodontic tooth movement. Sci Rep. 2020; 10 https://doi.org/10.1038/s41598-020-69030-x
Bakathir MA, Linjawi AI, Omar SS Effects of nicotine on bone during orthodontic tooth movement in male rats. Histological and immunohistochemical study. Saudi Med J. 2016; 37:1127-1135 https://doi.org/10.15537/smj.2016.10.15159
Sundararaj D, Venkatachalapathy S, Tandon A, Pereira A Critical evaluation of incidence and prevalence of white spot lesions during fixed orthodontic appliance treatment: a metaanalysis. J Int Soc Prev Community Dent. 2015; 5:433-439 https://doi.org/10.4103/2231-0762.167719
Naranjo AA, Triviño ML, Jaramillo A Changes in the subgingival microbiota and periodontal parameters before and 3 months after bracket placement. Am J Orthod Dentofacial Orthop. 2006; 130:275.e17-275.e2 https://doi.org/10.1016/j.ajodo.2005.10.022
Klukowska M, Bader A, Erbe C Plaque levels of patients with fixed orthodontic appliances measured by digital plaque image analysis. Am J Orthod Dentofacial Orthop. 2011; 139:e463-e470 https://doi.org/10.1016/j.ajodo.2010.05.019
Shokeen B, Viloria E, Duong E The impact of fixed orthodontic appliances and clear aligners on the oral microbiome and the association with clinical parameters: a longitudinal comparative study. Am J Orthod Dentofacial Orthop. 2022; 161:e475-e485 https://doi.org/10.1016/j.ajodo.2021.10.015
Vemulapalli A, Mandapati SR, Kotha A, Aryal S Association between vaping and untreated caries: a cross-sectional study of National Health and Nutrition Examination Survey 2017–2018 data. J Am Dent Assoc. 2021; 152:720-729 https://doi.org/10.1016/j.adaj.2021.04.014
Rouabhia M, Semlali A Electronic cigarette vapor increases Streptococcus mutans growth, adhesion, biofilm formation, and expression of the biofilm-associated genes. Oral Dis. 2021; 27:639-647 https://doi.org/10.1111/odi.13564
Catala-Valentin A, Bernard JN, Caldwell M E-cigarette aerosol exposure favors the growth and colonization of oral Streptococcus mutans compared to commensal streptococci. Microbiol Spectr. 2022; 10 https://doi.org/10.1128/spectrum.02421-21
Guo X, Hou L, Peng X, Tang F The prevalence of xerostomia among e-cigarette or combustible tobacco users: a systematic review and meta-analysis. Tob Induc Dis. 2023; 21 https://doi.org/10.18332/tid/156676
Fairchild R, Setarehnejad A Erosive potential of commonly available vapes: a cause for concern?. Br Dent J. 2021; 231:487-491 https://doi.org/10.1038/s41415-021-3563-1
Sørensen LT The clinical impact of smoking and smoking cessation: a systematic review and meta-analysis. Arch Surg. 2012; 147:373-383 https://doi.org/10.1001/archsurg.2012.5
Kuhlefelt M, Laine P, Suominen AL Smoking as a significant risk factor for infections after orthognathic surgery. J Oral Maxillofac Surg. 2012; 70:1643-1647 https://doi.org/10.1016/j.joms.2011.06.224
Ashour O, Al-Huneidy L, Noordeen H The implications of vaping on surgical wound healing: a systematic review. Surgery. 2023; 173:1452-1462 https://doi.org/10.1016/j.surg.2023.02.017
Thieman T, Westmark D, Sutton A Electronic cigarettes and cutaneous wound healing: a systematic review. J Am Acad Dermatol. 2023; 88:911-912 https://doi.org/10.1016/j.jaad.2022.10.042
Pitzer CR, Aboaziza EA, O'Reilly JM Nicotine and microvascular responses in skeletal muscle from acute exposure to cigarettes and vaping. Int J Mol Sci. 2023; 24 https://doi.org/10.3390/ijms241210208
Jacobi J, Jang JJ, Sundram U Nicotine accelerates angiogenesis and wound healing in genetically diabetic mice. Am J Pathol. 2002; 161:97-104 https://doi.org/10.1016/S0002-9440(10)64161-2
Martin JW, Mousa SS, Shaker O, Mousa SA The multiple faces of nicotine and its implications in tissue and wound repair. Exp Dermatol. 2009; 18:497-505 https://doi.org/10.1111/j.1600-0625.2009.00854.x
Reuther WJ, Brennan PA Is nicotine still the bad guy? Summary of the effects of smoking on patients with head and neck cancer in the postoperative period and the uses of nicotine replacement therapy in these patients. Br J Oral Maxillofac Surg. 2014; 52:102-105 https://doi.org/10.1016/j.bjoms.2013.11.003
Reuther WJ, Hale B, Matharu J Do you mind if I vape? Immediate effects of electronic cigarettes on perfusion in buccal mucosal tissue – a pilot study. Br J Oral Maxillofac Surg. 2016; 54:338-541 https://doi.org/10.1016/j.bjoms.2015.12.001
Silveira ML, Everard CD, Sharma E Tobacco use and incidence of adverse oral health outcomes among US adults in the Population Assessment of Tobacco and Health Study. JAMA Netw Open. 2022; 5 https://doi.org/10.1001/jamanetworkopen.2022.45909
Wadia R, Booth V, Yap HF, Moyes DL A pilot study of the gingival response when smokers switch from smoking to vaping. Br Dent J. 2016; 221:722-726 https://doi.org/10.1038/sj.bdj.2016.914
Karanjkar RR, Preshaw PM, Ellis JS, Holliday R Effect of tobacco and nicotine in causing staining of dental hard tissues and dental materials: a systematic review and metaanalysis. Clin Exp Dent Res. 2023; 9:150-164 https://doi.org/10.1002/cre2.683
Holliday R, Hong B, McColl E Interventions for tobacco cessation delivered by dental professionals. Cochrane Database Syst Rev. 2021; 2:(2) https://doi.org/10.1002/14651858.CD005084.pub4
Banks E, Yazidjoglou A, Brown S Electronic cigarettes and health outcomes: umbrella and systematic review of the global evidence. Med J Aust. 2023; 218:267-275 https://doi.org/10.5694/mja2.51890
Specialist Registrar in Orthodontics (ST2); North Cumbria Integrated Care NHS Foundation Trust/School of Dental Sciences, Faculty of Medical Sciences, Newcastle University.
Academic Clinical Fellow and Dental Core Trainee, School of Dental Sciences, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne Hospitals NHS Foundation Trust.
Senior Lecturer and Honorary Consultant in Restorative Dentistry, School of Dental Sciences, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne Hospitals NHS Foundation Trust
E-cigarettes can be a useful cessation aid for adult smokers. However, the use of e-cigarettes by young people in the UK has been on the rise and is of increasing concern. The implications of e-cigarette use among patients undergoing orthodontic treatment have not yet been reviewed. This narrative review explores the emerging evidence base underpinning the relationship of e-cigarette use on tooth movement, demineralization and surgical outcomes.
CPD/Clinical Relevance: The use of e-cigarettes has rapidly increased, and it is important to understand the possible implications for orthodontic treatment.
Article
Many health behaviours have the potential to impact on orthodontic treatment for example, dietary factors, oral hygiene habits and tobacco smoking. Electronic cigarettes (e-cigarettes) have been available for over 15 years in the UK, with specific EU regulation since 2014.1 It is estimated that 4.5 million UK adults currently use e-cigarettes2 and e-cigarettes have been the most popular quit aid used by smokers since 2013.3 There is high-certainty evidence that e-cigarettes are effective for smoking cessation and have increased quit rates compared to conventional nicotine replacement therapy.4,5
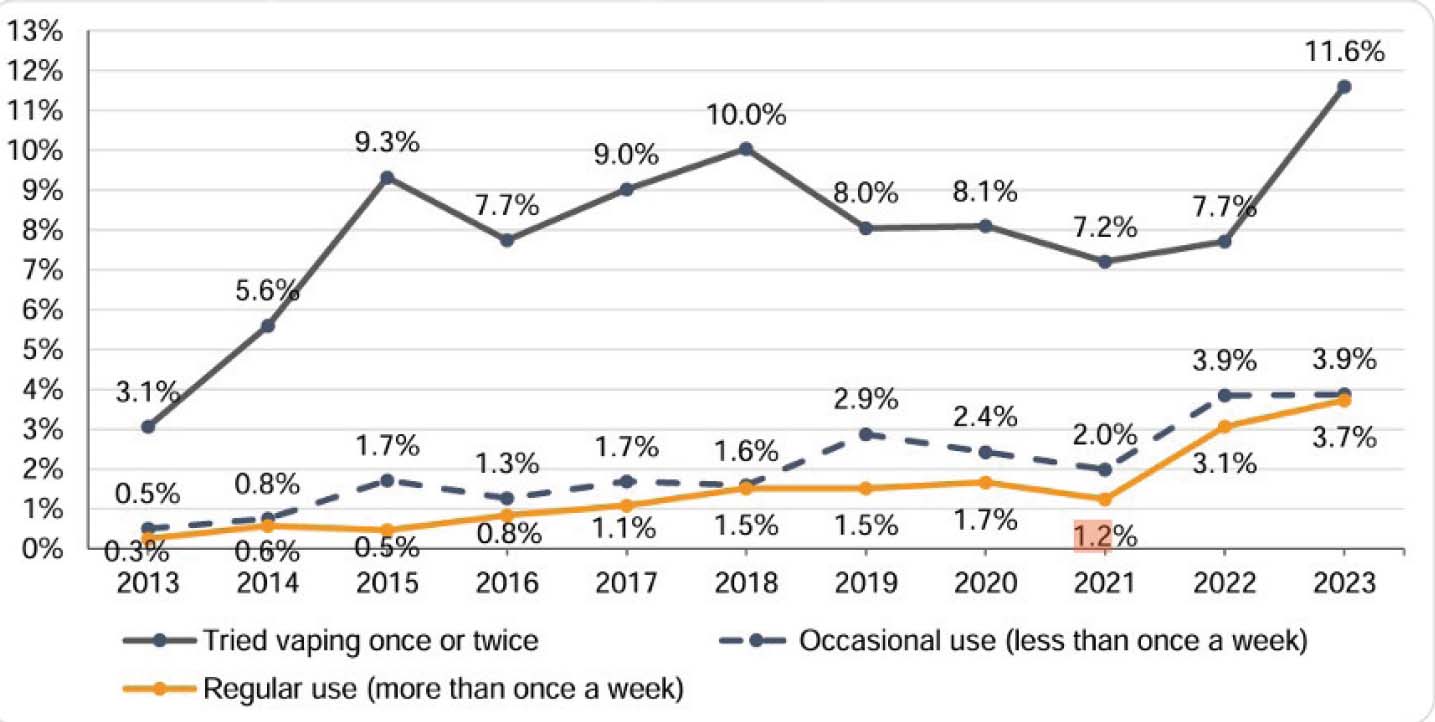
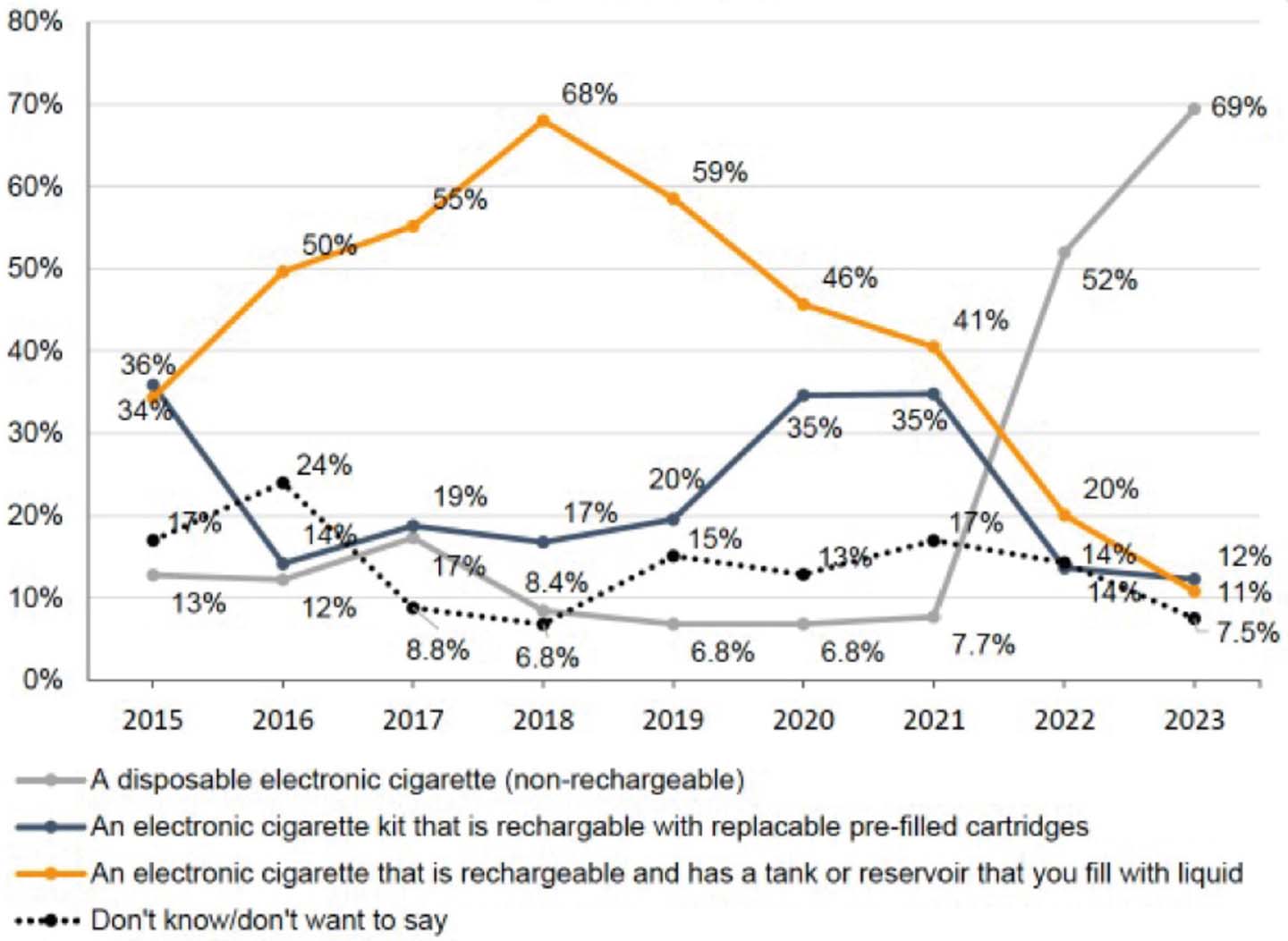
Youth use of e-cigarettes had remained relatively low and stable until 2022, when a sudden increase was seen. Regular usage (more than once a week) in 11–17 year olds has increased from 1.2% in 2021 to 3.7% in 2023 (Figure 1).6 Eighteen percent of 18-year-olds were current e-cigarette users in 2023.3 This increase has largely been put down to the use of disposable products (Figures 2 and 3).6 There has been public health concern about this increase and a government consultation and proposed regulation to ban disposable products and increase flavour and packaging restrictions.
Figure 1. Regular usage (more than once a week) in 11–17 years of age has increased from 1.2% in 2021 to 3.7% in 2023.3 Ash Smokefree GB Youth surveys: 2014–2023. Unweighted base: all 11–17 year olds (2013 = 1895; 2014 = 1817; 2015 = 1834; 2016 = 1735; 2017 = 2151; 2018 = 1807; 2019 = 1982; 2020 = 2029; 2022 = 2111; 2023 = 2028).Figure 2. Disposable e-cigarette products.Figure 3. Most frequently used e-cigarette by device type, current GB youth (11–17 years of age) users of e-cigarettes, 2015–2023. Ash Smokefree GB Youth surveys: 2014–2023. Unweighted base: all 11–17 year olds (2015 = 41; 2016 = 36; 2017 = 60; 2018 = 59; 2019 = 94; 2020 = 94; 2022 = 172; 2023 = 187).
There is wide consensus that e-cigarette use is significantly less harmful than smoking, but not risk free. For smokers using e-cigarettes as a quit aid, any potential risks from e-cigarette use are likely to be greatly outweighed by stopping tobacco smoking. However, for a young person who is a non-smoker, e-cigarettes will pose health impacts. Additionally young people may be particularly prone to effects given their continued development and the delicate nature of some tissues.7
Several previous papers and resources have explored the potential oral health effects of e-cigarette use.8,9 This article focuses specifically on the potential orthodontic implications of e-cigarette use. This may help guide future research and inform clinical practice.
Orthodontic-specific aspects of interest
E-cigarette use may impact the following areas that are particularly relevant for an orthodontic patient:
Tooth movement;
Caries;
Surgical healing;
Staining.
The following sections review and summarize the evidence base across these areas.
Orthodontic tooth movement
Orthodontic tooth movement (OTM) is a dynamic process dependent on active bone remodelling described by the pressure–tension theory.10 This complex process is regulated by several key factors, including osteoprotegerin, prostaglandins, and cytokines. Importantly, force-induced aseptic inflammation plays a pivotal role in OTM and requires strict control to prevent side effects, which can include alveolar bone loss, root resorption and destruction of periodontal tissues.11
No studies have directly evaluated the impacts of e-cigarette use on tooth movement in either clinical or laboratory studies. However, studies have investigated the relationship of nicotine alone on OTM in animal models (rats and mice). Interestingly several studies found that nicotine was associated with accelerated rates of tooth movement, all finding the most significant differences between the highest strength nicotine group and the control group (no nicotine).12–14 Sodagar et al increased the nicotine dose and identified an increase in mean amounts of tooth movement from 0.4 mm, 0.62 mm and 0.78 mm compared to 0.21 mm in the control group. One study found nicotine exposure significantly increased orthodontically induced inflammatory root resorption (OIIRR)14 and another looked histologically and reported ‘unbalanced resorption–apposition bone remodelling patterns and increased osteoclast cell distribution’.15 Another study found conflicting results, reporting no significant impact of nicotine on tooth movement.16 The authors of this study discussed limitations in the previous studies (showing accelerated tooth movement) that included measurement methods and the timing of nicotine administration.
These studies all used daily subcutaneous injections of nicotine. A single bolus of high-dose nicotine is unlikely to be comparable to the daily nicotine profile seen in either tobacco smokers or e-cigarette users. Hence, there are limitations in how much can be extrapolated from these studies to clinical scenarios. Nevertheless, the animal studies reveal insights into the potential effects of nicotine exposure from e-cigarettes on OTM. Further research, ideally on humans, is required to fully understand the effects on human oral physiology.
Caries and demineralization
Patients undergoing orthodontic treatment with fixed appliances are at an increased risk of developing caries and white spot lesions. One meta-analysis reported an incidence of new carious lesions during orthodontic treatment as 45.8% with a prevalence of 68.4%.17 It should be noted that caries and decalcification occurrence can vary depending on individual risk factors, and the impact of socio-economic status and area deprivation cannot be underestimated.18 Multiple studies have demonstrated an increase in plaque accumulation associated with fixed orthodontic appliances; however, most are limited by small sample sizes.19–21 With recent data suggesting that the proportion of young people experimenting with vaping has grown by 50% year on year, it is important to consider the association between e-cigarettes, caries and erosion among this cohort of patients.6
An association has been suggested between e-cigarette use and caries. The strongest evidence to date comes from a cross-sectional study of self-reported data. Individuals who used e-cigarettes were more likely to have untreated caries (odds ratio 1.69; 95% CI 1.24–2.29) than those who had never smoked or used e-cigarettes.22 However, as discussed by the study authors, because of the cross-sectional design, causality could not be established. Also, although they controlled for some demographic factors, they were not able to adjust for other important factors, such as diet.
Much of the available data is therefore limited to in vitro studies. It has been suggested that e-cigarette aerosols promote a significantly higher adhesive force between the enamel surface and Streptococcus mutans, a facultatively anaerobic bacterium implicated in the dental caries process. The e-liquids used in this study were produced by the research group, rather than using commercially available products.23 Separate laboratory-based studies highlighted enhanced biofilm formation and attachment of S mutans, but suppressed the growth of early colonizers, S sanguinis and S gordonii.24,25 Given that all the aforementioned bacteria are implicated in the ecological plaque hypothesis, the findings are contradictory about the impact on caries development.
Saliva has an important protective effect on the oral cavity. Individuals who experience reduced quality or quantity of saliva are at risk from increased caries and tooth surface loss rates.26 A common reported side effect of e-cigarette use is oral dryness, which could be related to the hygroscopic nature of several of the carrier agents in the e-liquids (propylene glycol and vegetable glycerine).27
This could be a potential mechanism for an increased caries rate.
When considering the erosive potential, an analysis of 45 e-cigarette liquids (e-liquids) available online in the UK found that several products had a pH below 5.5, with the authors concluding potential erosive effects.28 The results from this laboratory-based study, however, should be treated with caution because the buffering effect of saliva, the complexities of the oral microbiome nor the titratability of the acid. were not taken into account How readily acids disassociate is of more consequence than a low pH in isolation. Most importantly, it should be noted that the study highlighted only the erosive potential of products that did not contain nicotine. The nicotinecontaining samples (which are more representative of the products used by the general population) had an alkaline pH.
In summary, the body of evidence indicates a noteworthy association between e-cigarette use and an increased risk of caries. However, these findings are not without limitations, including methodological constraints and the reliance on self-reported data. Further research is essential to determine the extent of the relationship between e-cigarette use and caries and erosion risk with special consideration for those undergoing orthodontic treatment.
E-cigarettes and surgery
Traditional tobacco smoking is a wellestablished risk factor for adverse outcomes following surgery, including increased surgical site infections.28 Similarly, orthognathic surgery patients who smoke are more likely to experience these infections.29 Many harmful components of tobacco smoke, such as carbon monoxide and hydrogen cyanide, are likely to be responsible for these negative effects. E-cigarettes, on the other hand, either lack these components entirely, or contain them at significantly lower levels. Therefore, it is hypothesized that e-cigarette use may be associated with fewer adverse post-operative outcomes compared to tobacco smoking.
As with other areas explored in this review, there is a paucity of direct clinical evidence on the impact of e-cigarettes on surgical outcomes. Existing research is primarily limited to case reports: animal and human studies using surrogate physiological markers for cutaneous wound healing and cell-line laboratory studies.30,31 These studies raise concerns about potential negative effects of e-cigarettes on inflammation, oxidative stress, endothelial dysfunction, blood flow/oxygenation and platelet function.
The vasoactive and wound healing effects of nicotine are complex and warrant further investigation. Traditionally nicotine is considered a vasoconstrictor owing to its sympathomimetic properties.32 However, a recent study has questioned the role of nicotine in this process, although still reporting a similar vasoconstrictive effect of e-cigarette use.33 Conversely, other studies suggest nicotine may reduce inflammation,34 accelerate wound healing (in diabetic mice), and promote wound angiogenesis.35,36 The potential benefits of topical nicotine application for wound healing were even explored by oral and maxillofacial surgeons through a series of publications,37 including a small pilot clinical trial with 10 participants. This found a statistically significant, initial increase in buccal mucosa tissue perfusion among e-cigarette users with nicotine compared to without.38 Some clinical studies have shown an association between e-cigarette use and gingival bleeding.39 However, interpreting these findings is challenging because users often quit tobacco smoking concurrently, which is known to increase gingival bleeding, making it difficult to isolate the specific impact of e-cigarette use.39,40 Further clinical research is necessary to determine the precise role of nicotine in wound healing.
Given the high volume of surgeries performed worldwide, and the widespread use of e-cigarettes for over a decade, the lack of robust clinical studies reporting adverse surgical outcomes in this population is surprising, and perhaps telling in its own right – if there were major impacts of e-cigarette use on surgical outcomes, we would perhaps expect to see a strong signal to indicate this in the evidence base. For elective procedures, such as orthognathic surgery, where the consequences of complications are high, it remains prudent to minimize all modifiable risk factors. Ideally, patients should abstain from both smoking and vaping before undergoing surgery.
Staining
Tobacco smoking is well known to cause staining of the dental hard tissues.41 In the context of orthodontics, this has relevance to restorative materials, in particular resin composites. A recent, comprehensive systematic review examined the evidence for staining caused by novel nicotine products, including e-cigarettes. The review found low-quality evidence suggesting that e-cigarettes may cause staining, but to a lesser degree than cigarette smoke.40
Discussion
We have reviewed the evidence for adverse oral health impacts of e-cigarette use across four clinical areas of relevance to orthodontics. There are several common themes across the areas: the evidence base is generally weaker quality and not conclusive, the indication is that the oral health effects are relatively minimal, but further research is needed. In our opinion, possible increased caries risk is one of the areas with the strongest data to date, and one to watch as the evidence develops.
Cigarette smoking is not an absolute contraindication for orthodontic treatment, but carries increased risks and patients should be provided with evidence-based cessation interventions.42,43 E-cigarettes are the most common quit aid being used by smokers (in England)44 and are recommended by the NHS and NICE as options smokers could consider.45,46 Robust evidence shows e-cigarettes are more effective than conventional treatments, such as nicotine replacement therapy.4 Hence, adult orthodontic patients who are current or former smokers, may be using e-cigarettes as part of a current or recent quit attempt. The advice for dual users (i.e. those smoking and vaping) is that they should quit smoking completely. For vapers, the current NHS advice is that they should aim to quit vaping as well, but not to rush this process, and only do it when they are sure they will not go back to smoking.46
Given the typical young patient population in orthodontics, and current trends in tobacco cigarette and e-cigarette use, a common scenario we face clinically is a young person who has never smoked, but who is using an e-cigarette. In this situation, we should engage in a non-judgemental conversation with the patient, presenting the current uncertainties surrounding e-cigarettes' oral health impacts based on available research. While e-cigarette use is not an absolute contraindication for orthodontic treatment, in the authors' opinion, it is likely to carry a slightly increased risk of complications, particularly when considering surgical options. There is a range of concerns for young people using e-cigarettes: unnecessary addiction (disruption to education); unnecessary costs; environmental impact; and general health impacts, such as lung damage or causing harm to the developing brain.47,48 For a young person seeking orthodontic treatment, the interaction with an orthodontist could be a powerful motivator to quit vaping.
Conclusion
Tobacco smoking is a well-documented risk factor for various adverse oral health outcomes. Emerging evidence suggests that e-cigarette use might also have detrimental effects on oral health during orthodontic treatment, although likely to be to a lesser extent than tobacco smoking. However, the current evidence in this area is limited and of weak quality. Further well-designed studies are crucial to definitively understand the impact of e-cigarettes on oral health in orthodontic patients. This is particularly important for young people who may have never smoked tobacco before, but use e-cigarettes. In the interim, it is advisable for healthcare professionals to encourage and support orthodontic patients, especially young people, to reduce or ideally eliminate their e-cigarette use altogether.