
Article

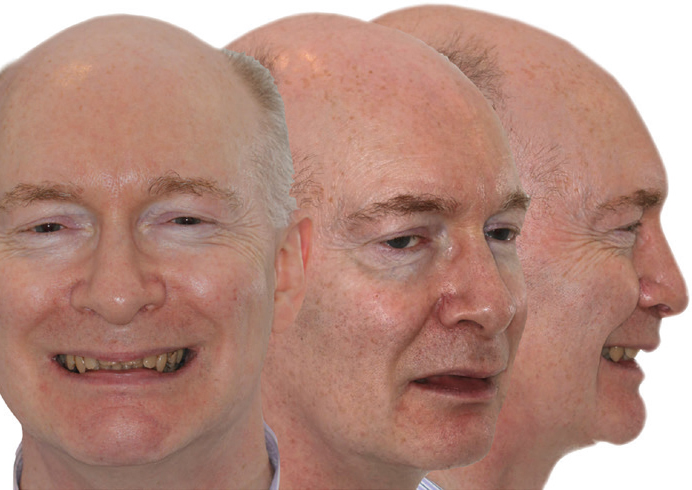
A 53-year-old man with a Class II division 1 incisor relationship on a mild Class II skeletal base with a reduced mandibular planes angle (Figure 1) presented. He had an overjet of 7 mm and an overbite of 6 mm with a spaced, proclined upper labial segment, a mildly crowded lower labial segment, and an extremely narrow lower arch. Bilaterally, he demonstrated a scissors bite on the premolars (Figure 2).

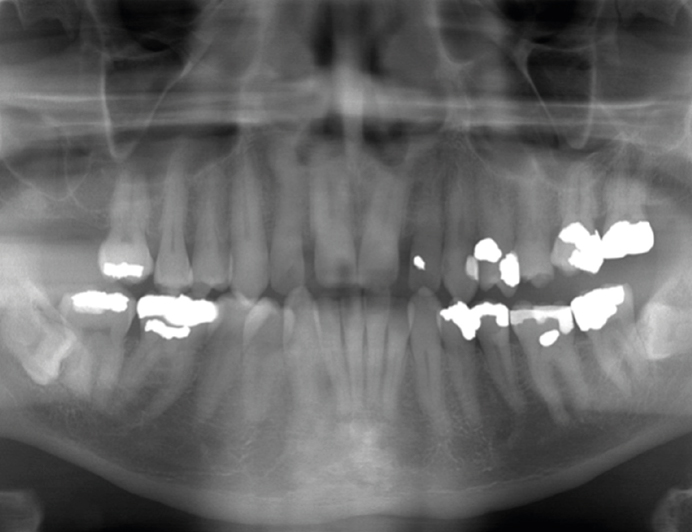
The panoramic radiograph revealed a very heavily filled, but reasonably healthy dentition, with reasonable bone levels for a man in his mid 50s. He had horizontally impacted low wisdom teeth that were asymptomatic (Figure 3).
He was very keen to achieve correction of his bite and if possible, he would like an improvement in the anterior aesthetics.
How would you address this patient's needs?