
Article

A 24-year-old woman presented to the clinic complaining of her ‘jaw to being to one side’ and didn't like the way the crossbite looked. She had no major issues eating. Medical history revealed that she had well-controlled eczema, had one episode of pityriasis rosea, sickle cell family history and was a haemoglobin C carrier.
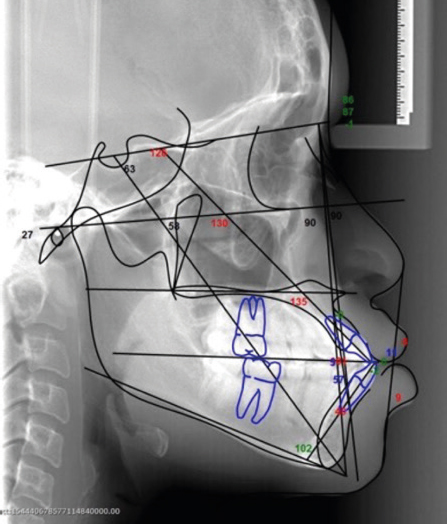
Extra-orally, she presented with a mild Class 3 skeletal pattern with moderate asymmetry. Both the maxilla and mandible were prognathic, but reasonably balanced in terms of ethnic norms. During smiling, the mandibular asymmetry was more visible and a maxillary cant was present (Figure 1).


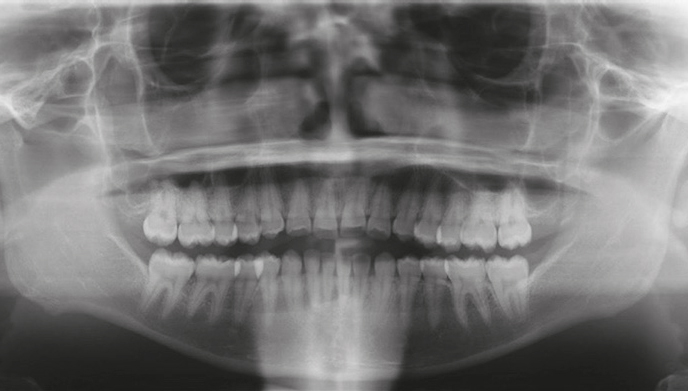
Intra-orally she had 7–7 upper and lower and good periodontal health. She had a Class 3 incisor relationship with a maximum overjet of −4 mm and average overbite. The lower centreline was 4 mm to the right and there was a crossbite without displacement affecting the LR4–LL1 with the UR3–UR1. The molar relationship was ½ Class 3 on the left and ¼ unit Class 3 on the right with the canines ½ Class 3 on the right and Class 1 on the left. There was mild spacing in the upper and lower arches. IOTN was 4m.
How would you address this patient's needs?