Ando S, Aizawa K, Nakashima T, Sanka Y, Shimbo K, Kiyokawa K. Transmigration process of the impacted mandibular cuspid. J Nihon Univ Sch Dent. 1964; 6:66-71
Tarsitano JJ, Wooten JW, Burditt JT. Transmigration of nonerupted mandibular canines: report of cases. J Am Dent Assoc. 1971; 82:1395-1397
Mupparapu M. Patterns of intra-osseous transmigration and ectopic eruption of mandibular canines: review of literature and report of nine additional cases. Dentomaxillofac Radiol. 2002; 31:(6)355-360
Sumer P, Sumer M, Ozden B, Otan F. Transmigration of mandibular canines: a report of six cases and a review of the literature. J Contemp Dent Pract. 2007; 8:1-9
Kara MI, Ay S, Aktan AM, Sener I, Bereket C, Ezirganlt S, Demirkole M. Analysis of different types of transmigrant mandibular teeth. Med Oral Pathol Oral Cir Bucal. 2011; 16:e335-e340
Aydin U, Yilmaz HH, Yildirim D. Incidence of canine impaction and transmigration in a patient population. Dentomaxillofac Radiol. 2004; 33:164-169
Aktan AM, Kara S, Akgünlü F, Malkoç S. The incidence of canine transmigration and tooth impaction in a Turkish sub population. Eur J Orthod. 2010; 32:575-581
Howard RD. The anomalous mandibular canine. Br J Orthod. 1976; 3:117-119
Javid B. Transmigration of impacted mandibular cuspids. Int J Oral Surg. 1985; 14:547-549
Joshi MR. Transmigrant mandibular canines: a record of 28 cases and a retrospective review of the literature. Angle Orthod. 2001; 71:12-22
Vichi M, Franchi L. The transmigration of the permanent lower canine. Minerva Stomatol. 1991; 40:579-589
Alaejos-Algarra C, Berini-Aytes L, Gay-Escoda C. Transmigration of mandibular canines: report of six cases and review of the literature. Quintessence Int. 1998; 29:395-398
Marks SCJ, Schroeder HE. Tooth eruption: theories and facts. Anat Rec. 1996; 245:374-393
Bruszt P. Neurological anomaly associated with extreme malposition of a mandibular canine. Oral Surg Oral Med Oral Pathol. 1958; 11:89-90
Nodine AM. Aberrant teeth, their history, causes and treatment. Dent Items Interest. 1943; 65:440-451
Thoma KH., 2nd edn. St Louis, Miss: CV Mosby; 1952
Wertz RA. Treatment of transmigrated mandibular canines. Am J Orthod Dentofac Orthop. 1994; 106:419-427
Shapira Y, Mischler WA, Kuftinec MM. The displaced mandibular canine. Am Soc Dent Child J. 1982; 49:362-364
Taguchi Y, Kurol J, Kobayashi H, Noda T. Eruption disturbances of mandibular permanent canines in Japanese children. Int J Paediatr Dent. 2001; 11:98-102
Murthy S, Nagalakshmi V, Nagabhushan Vani C. Impacted transmigrated canine with mural ameloblastoma: an unusual case report with review of literature. J Orofac Sci. 2010; 2:36-39
Mitchel L. Displacement of a mandibular canine following fracture of the mandible. Br Dent J. 1993; 174:417-418
Nixon F, Lowey MN. Failed eruption of the permanent canine following open reduction of a mandibular fracture in a child. Br Dent J. 1990; 168:204-205
González-Sánchez MA, Berini-Aytés L, Gay-Escoda C. Transmigrant impacted mandibular canines. A retrospective study of 15 cases. J Am Dent Assoc. 2007; 138:1450-1455
Peck S. On the phenomenon of intraosseous migration of nonerupting teeth. Am J Orthod Dentofacial Orthop. 1998; 113:515-517
Baykul T, Heybeli N, Oyar O, Doğru H. Multiple huge osteomas of the mandible causing disfigurement related with Gardner's syndrome: case report. Auris Nasus Larynx. 2003; 30:447-451
Nanci A., 7th edn. St Louis, Missouri: Mosby; 2008
Almonaitiene R, Balciuniene I, Tutkuviene J. Factors influencing permanent teeth eruption. Part one – General factors. Stomatologija. 2010; 12:67-72
Mupparapu M, Auluk A, Setty S, Pai K, Nagpal A. Patterns of intraosseous migration and ectopic eruption of bilaterally transmigrating mandibular canines: radiographic study and proposed classification. Quintessence Int. 2007; 38:821-828
Alba M, Pérez M, Berrocal IL, Dorado CB, Cáliz FF, José M, González M. Transmigrated canines: review and update. J Clin Exp Dent. 2011; 3:e235-e239
Viswanathan S. Horizontal transmigration of mandibular canine with bilateral enostosis between the premolars – A case report. Int J Clin Dent Sci. 2011; 2:84-87
Nagaveni NB, Radhika NB, Umashankar KV, Satish TS. Concomitant occurrence of canine transmigration and symmetrical agenesis of incisors – a case report. Bangladesh J Med Sci. 2011; 10:133-136
Camilleri S, Scerri E. Transmigration of mandibular canines – a review of the literature and a report of five cases. Angle Orthod. 2003; 73:753-762
Peerlings RHJ. Treatment of a horizontally impacted mandibular canine in a girl with a Class II Division 1 malocclusion. Am J Orthod Dentofacial Orthop. 2010; 137:S154-162
Trakyalı G, Çıldır ŞK, Sandallı N. Orthodontic treatment of a transmigrated mandibular canine: a case report. Aust Orthod J. 2010; 26:195-200
Raffat A, Ijaz A. Autotransplantation of transmigrated mandibular canine. J Pak Med Assoc. 2009; 59:53-55
Patel S, Fanshawe T, Bister D, Cobourne MT. Survival and success of maxillary canine autotransplantation: a retrospective investigation. Eur J Orthod. 2011; 33:298-304
Sharma G, Nagpal A. Transmigration of mandibular canine: report of four cases and review of literature. Case Reports Dent. 2011; 1-5
Intra-osseous migration of a non-erupted mandibular canine is a rare phenomenon. The purpose of this article is to report 13 such cases of transmigration. The article reviews various aetiological hypotheses involved in transmigration, outlines diagnostic pathways for a patient presenting with missing permanent canines with or without over-retained deciduous teeth and discusses various treatment options for transmigration.
Clinical Relevance: The article proposes a difficulty assessing for the orthodontic traction of a transmigrated canine which may help the clinician in treatment planning.
Article
Intra-osseous migration of non-erupting teeth is a rare natural condition of horizontal tooth movement within the bone and is termed as transmigration if the tooth crosses the midline.1,2 Management of such impacted and transmigrated teeth includes extraction or orthodontic alignment into the arch. We report 13 cases of transmigrated canines and also discuss a diagnostic sequence, as well as treatment considerations.
Case Reports
Case 1
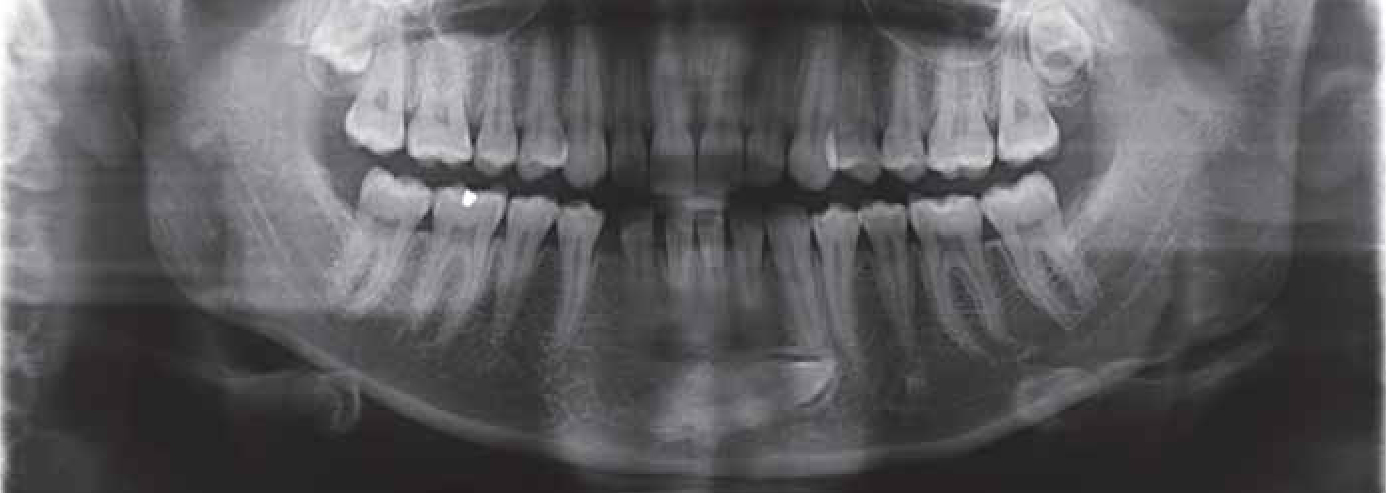
A 13-year-old female patient reported with a complaint of irregularly-placed upper front teeth. Clinical presentation was an increased overjet. A panoramic radiograph revealed transmigrated LR3 below the apices of LL1, 2, 3 (Figure 1).
Figure 1. Panoramic radiograph showing right mandibular canine transmigrated below the apices of the left incisors and canine.
Case 2
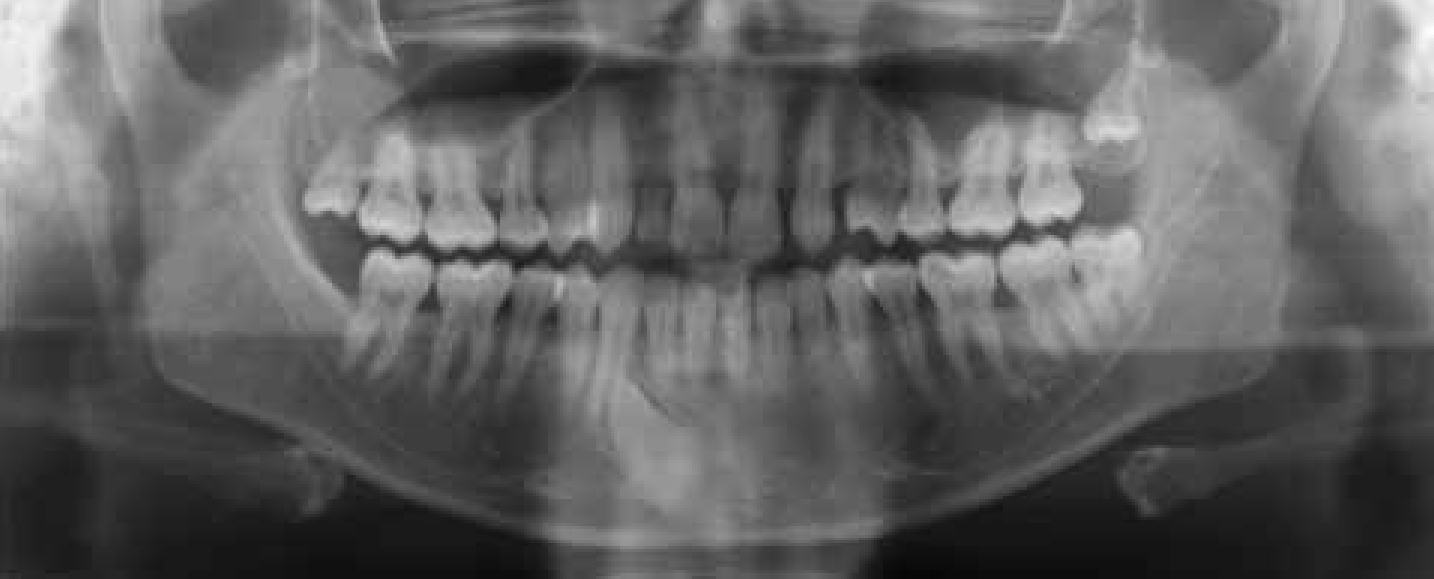
An 18-year-old female patient reported with a complaint of proclined upper anterior teeth. Clinical presentation was an increased overjet. A panoramic radiograph revealed transmigrated LL3 below the apices of LR3, 2, 1; retained LLC and missing LL2 were noticed (Figure 2).
Figure 2. Panoramic radiograph showing the left mandibular canine transmigrated below the apices of the right incisors and canine.
Case 3
A 27-year-old male patient reported complaining of pain and swelling in the lower jaw. Panoramic radiographs revealed a large radiolucency extending from lower LL8 to LR7. Biopsy confirmed it as unicystic ameloblastoma. LL3 had pathologically transmigrated to the right side with only the root crossing the midline (Figure 3).
Figure 3. Panoramic radiographs showing the pathologically transmigrated lower left canine, to right side, with only the root crossing the midline.
Case 4
A 30-year-old male patient reported complaining of space between the upper front teeth. Panoramic radiograph revealed transmigrated LL3 below the apices of LR3, 2, 1, retained LLC and missing UL2 (Figure 4).
Figure 4. Panoramic radiograph showing the transmigrated left mandibular canine erupting mesial to the right canine.
Case 5
A 15-year-old female patient reported complaining of proclined upper front teeth. Panoramic radiographs revealed transmigrated LL3 below the apices of LR2, 1; retained LLC and impacted UR3 and UL3 were observed (Figure 5).
Figure 5. Panoramic radiograph showing the left mandibular canine transmigrated below the apices of the right incisors.
Case 6
A 25-year-old female patient reported complaining of proclined upper anterior teeth. Panoramic radiographs revealed transmigrated LL3 below the apices of LR3, 2, 1, retained LLC and impacted UL3 (Figure 6).
Figure 6. Panoramic radiograph showing the left mandibular canine transmigrated below the apices of the right incisors and canine.
Case 7
A 29-year-old male patient reported for the prosthodontic replacement of missing upper and lower front teeth. Panoramic radiographs revealed transmigrated LL3 in the edentulous area of LR2 and 1 (Figure 7).
Figure 7. Panoramic radiograph showing the left mandibular canine transmigrated into the edentulous area of the right incisors.
Case 8
A 15-year-old male patient reported for the prosthodontic replacement of upper front teeth. Panoramic radiographs revealed transmigrated LL3 oriented vertically below the apices of LR2, 1; over-retained LLC and LRC, and impacted LR3 UR3 and UL3 were observed (Figure 8).
Figure 8. Panoramic radiograph showing the transmigrated left mandibular canine oriented vertically below the apices of the right central incisor.
Case 9
A 13-year-old female patient reported with the complaint of forward-placed upper front teeth. Panoramic radiographs revealed transmigrated LL3 below the apices of LR2, 1 and retained LLC (Figure 9).
Figure 9. Panoramic radiograph showing the left mandibular canine transmigrated below the apices of the right incisors.
Case 10
A 29-year-old male patient reported with the complaint of space between the lower front teeth. Panoramic radiographs revealed transmigrated LR3 below the apices of LL1, 2, 3 and missing LL2 (Figure 10).
Figure 10. Panoramic radiograph showing the right mandibular canine transmigrated below the apices of the left incisors and canine.
Case 11
A 23-year-old female patient reported complaining of irregularly placed upper and lower front teeth. Panoramic radiographs revealed transmigrated LR3 below the apices of LL1, 2, 3, retained LRC and impacted UR3 and UL3 (Figure 11).
Figure 11. Panoramic radiograph showing the right mandibular canine transmigrated below the apices of the left incisors and canine.
Case 12
A 24-year-old male patient reported complaining of irregularly placed upper front teeth. Panoramic radiographs revealed transmigrated LR3 below the apices of LL1 and 2 (Figure 12).
Figure 12. Panoramic radiograph showing the right mandibular canine transmigrated below the apices of the left incisors.
Case 13
A 20-year-old female patient reported with the complaint of crowding in the upper front teeth. A panoramic radiograph revealed bilateral transmigrated canines situated horizontally below the LR2 and 1; LL1, 2 and retained LRC and LLC were observed (Figure 13).
Figure 13. Panoramic radiograph showing the bilateral transmigrated canines situated horizontally below the apices of the lower incisors.
Discussion
Transmigration of mandibular canines is a rare phenomenon with as few as 200 reported cases to date.3,4 According to various authors, the incidence of transmigration of canine ranges from 0.075% to 0.34%.5,6,7 Transmigration of other teeth, like mandibular lateral incisors and second premolars, have also been reported with extremely low incidence rates (0.0017% for lateral incisor and 0.0026% for second premolar5). Though these two teeth are most commonly affected, developmentally the reason for the difference in the incidence of transmigration is as yet unknown.
The aetiology of transmigration is unknown; many authors have suggested various phenomenona8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25 (Table 1). Eight of the 13 cases reported here had retained deciduous canines; these could be retained because of the absence of the resorptive forces from the succeeding tooth (ie the impacted and transmigrated permanent canine). In two cases, missing incisor teeth were observed. In only one case, the transmigration was pathological in nature and was associated with a cyst.
Etiologic factor
Hypothesis from literature
Developmental
Angulation of canine to midsagittal plane between 30 and 45° (Howard)8
Clinical signs that suggest the presence of genetic control like bilateral occurrence, hypodontia and palatally displaced canines are associated with transmigration (Peck)24
Intra-osseous tooth movement is regulated by the dental follicle, enamel organ and surrounding alveolar tissues; various putative molecules implicated in the tooth eruption signalling cascade, for example BMP-2, EGF, CSF-1, IL-1α, NFκB, Runx-2, etc have been identified. Formation of the tooth eruption pathway is a localized, genetically programmed event. Suggested eruption genes and their products are localized primarily in either the dental follicle or stellate reticulum.26,27 Any disturbance in this signalling cascade might lead to a deflected path of migration, indicating a strong genetic role in transmigration.
Transmigration of mandibular canines is generally a unilateral phenomenon, although bilateral cases have been reported.28 In 2002, Mupparapu proposed a classification for transmigrated mandibular canines according to their migratory pattern and position in the jaw and classified these teeth into five groups.3 Type 1 is the most common type among the cases reported in the literature (47.5%).3 Cases 1, 2, 5-7 and 9-12 of our reported cases are of this category. (Case 4 is of Type 3 category and Case 8 is of Type 5). The current classification does not accommodate cases with only root transmigration, as seen in Case 3. Hence, it necessitates further modification in the existing classification to include such cases (Table 2).
Type 1
Canine positioned mesio-angularly across the midline within the jaw bone, labia or lingual to anterior teeth, and the crown portion of the tooth crossing the midline.
Type 2
Canine horizontally impacted near the inferior border of the mandible below the apices of the incisors.
Type 3
Canine erupting either mesial or distal to the opposite canine.
Type 4
Canine horizontally impacted near the inferior border of the mandible below the apices of either premolars or molars on the opposite side.
Type 5
Canine positioned vertically in the midline (the long axis of the tooth crossing the midline) irrespective of eruption status.
Type 6
Canine with only root crossing the midline.
Unilateral transmigration is commonly associated with left side canines.29 In cases 2-9, left-side canines are transmigrated, and in cases 1, 10-12, right-side canines are involved. Our case series also confirms such a pattern of involvement.
The distance travelled by the canine ranges from the midline to the third molar on the opposite side. Type 4 of Mupparapu's classification is the farthest distance migrated, accounting for 9.9% of all transmigrations.3 Howard expected older patients would show greater distance of travel because of longer time available for migration.8 However, a review of Type 4 reported cases shows that the majority of them are detected at an early age between 6 and 31years;3,10,23 Alba et al also reported higher prevalence in the age group 0-20 years.29 Hence the distance of migration may not be age dependent but it may be due to abnormal displacement of the dental lamina, as proposed by Nodine,15 or could be of genetic aetiology.
Bilateral transmigration occurs in only 9% of all transmigrations.7 In 2007, Mupparapu et al proposed a new classification for bilaterally transmigrated mandibular canines into five groups with sub-types.28 A total of 19 cases of bilateral transmigration have been reported in the literature28 and a new case of Type 2 sub-type A has been added with this report (Case 13).
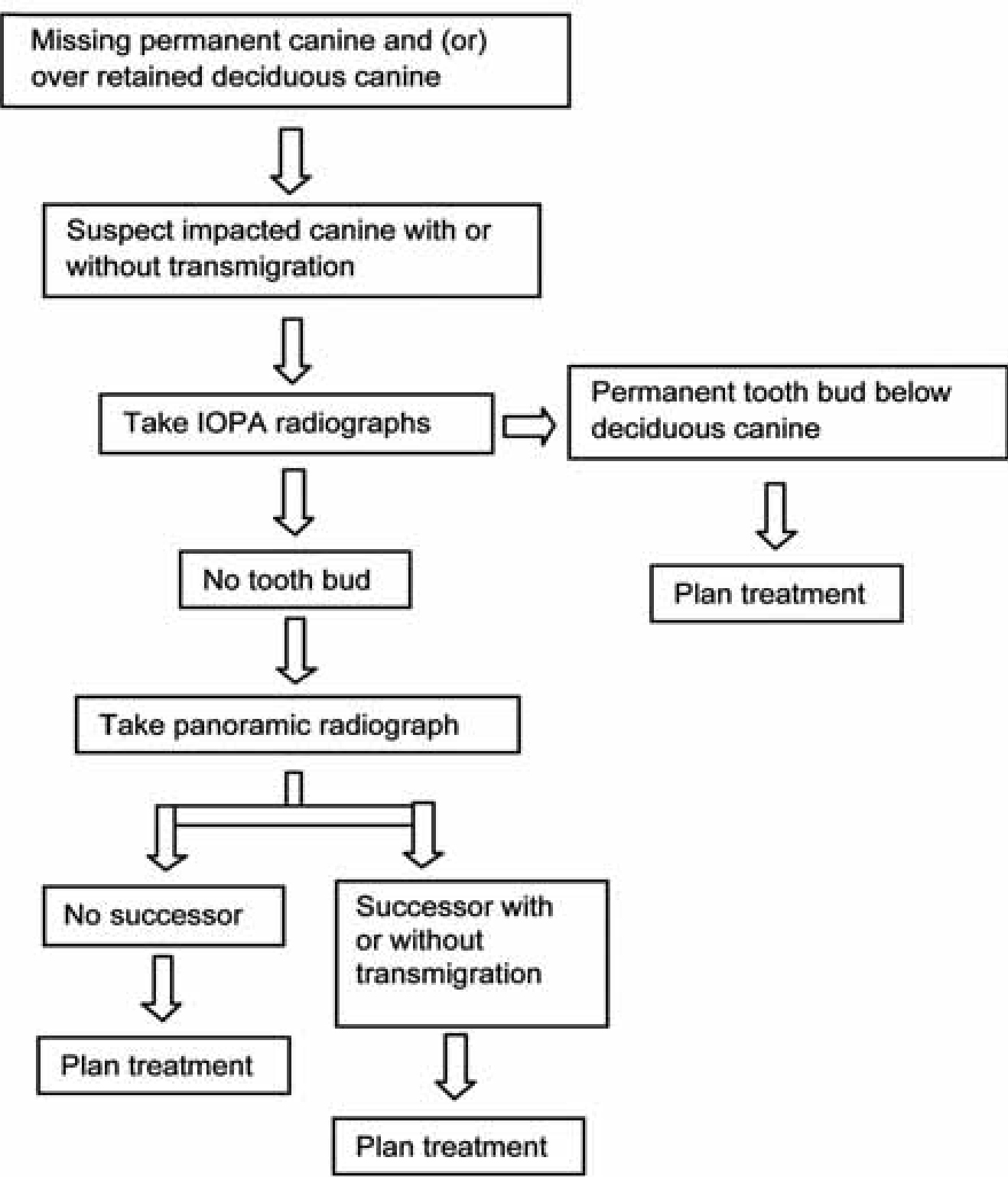
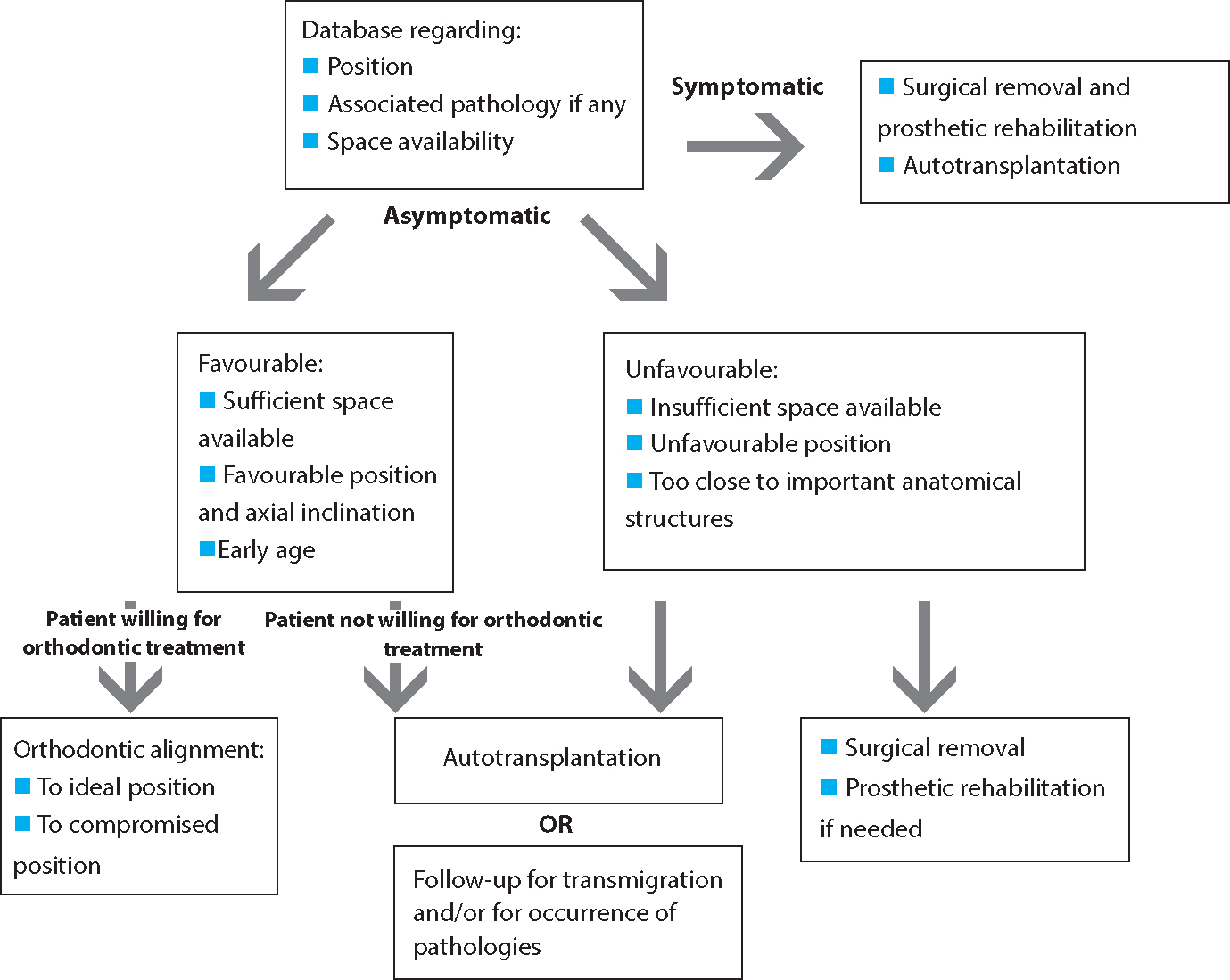
The majority of transmigrated canines are not associated with any pathology. However, cystic pathologies (17.2%), odontomas (3.3%), supernumerary teeth (1.9%),3,10,29 enostosis,30 Gardner's syndrome,25 mural ameloblastoma20 and bilateral agenesis of lower incisors31 have been reported in association with mandibular canine transmigration. In four of our cases (Cases 5, 6, 8 and 10) other canines are impacted. Several treatment options are available for transmigrated canines, which include orthodontic intervention, autotransplantation, surgical removal and periodic observation.6,9,17,18,23,32 From the data published regarding management of transmigrated canines, it is possible to outline pathways of care (Figures 14 and 15).
Figure 14. Diagnostic outline for cases presenting with a missing permanent canine and (or) over-retained deciduous canine.Figure 15. Treatment options for a transmigrated canine.
When the mandibular arch is crowded and requires therapeutic tooth extraction to correct incisor crowding, the surgical removal of transmigrated teeth can be considered. However, the symptomless unerupted teeth can be left in place.33 Transmigrated teeth associated with pathologies, like cysts, tumours and fractures, are often surgically removed, along with associated pathologies.7 Autotransplantation can also be considered if the tooth can be removed intact, even if associated with pathology. Improvement in the position of the canine after surgical removal of associated odontoma has been reported.29
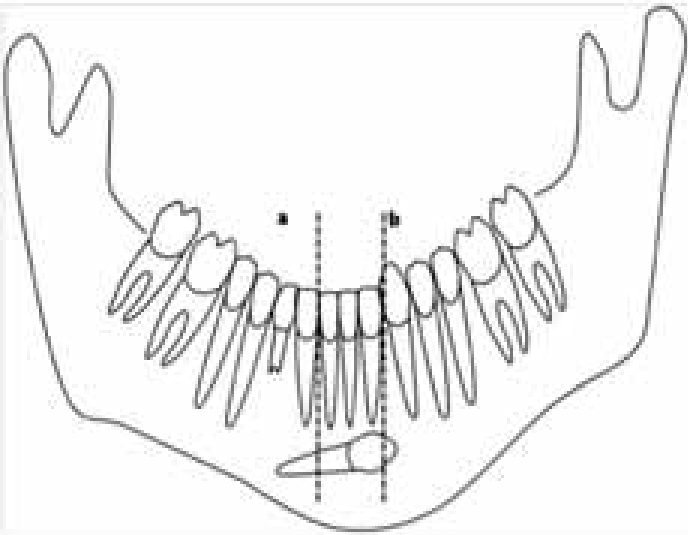
Orthodontic treatment appears to be the ideal treatment option for transmigrated teeth. The majority of the successfully treated cases mentioned in the literature are of Type 1 variety.17,33,34 Orthodontic alignment of a labially impacted transmigrated canine can be undertaken to its original position if the crown of the transmigrated canine has not migrated past the opposite lateral incisor, or if the apex has not migrated past the adjacent lateral incisor apex17 (Figure 16). Trakyalı reported the alignment of a transmigrated canine to a compromised position.34
Figure 16. Favourability assessment of a transmigrated canine. Lines a and b are drawn parallel to the long axis of the incisors. The root apex should not cross line a and (or) the crown should not cross line b.
Autotransplantation of a transmigrated canine may be indicated in selected circumstances where incisors are well aligned and sufficient space is available for the canine in those patients who are unwilling to undergo orthodontic treatment.8,32,35 However, the procedure is technique sensitive and success rate depends on apex development and is higher in teeth with an open apex. The patient must be informed regarding failure and risk associated with such procedure. Average survival rate of autotransplantation reported is about 14.5 years (1.4–27.8).36
Asymptomatic transmigrated canines can be left in place; however, a series of successive radiographs should be taken periodically to check on any progressive worsening in position, pathologic changes, neurologic symptoms and pressure resorption tendencies to adjacent teeth. Surgical intervention is suggested if any such changes are noticed.37
Conclusion
In conclusion, clinical observation of a retained deciduous canine or a missing permanent canine warrants further radiographic investigation to rule out possible transmigration of an impacted permanent canine. Early detection of transmigration may help in a better prognosis for orthodontic alignment. The current system of classification does not include teeth with root migration. We are suggesting a modification of Mupparapu's classification for unilateral transmigration by including transmigration of only root as Type 6.