Huber CH Parents of the handicapped child: facilitating acceptance through group counselling. Pers Guid J. 1979; 57:(5)267-269
Urbano MHLondon: Chapman and Hall; 1992
Speltz ML, Endriga MC, Fisher PA, Mason CA Early predictors of attachment in infants with cleft lip and/or palate. Child Develop. 1997; 68:(1)12-25
Maris CL, Endriga MC, Speltz ML, Jones KJ, De Klyen M Are infants with orofacial clefts at risk of insecure mother-child attachments?. Cleft Palate Craniofac J. 2000; 37:(3)257-265
Young JL, O'Riordan M, Goldstein JA, Robin NH What information do parents of newborns with cleft lip, palate, or both want to know?. The Cleft Palate-Craniofac J. 2001; 38:(1)55-58
Habel A, Elhadi N, Sommerlad B, Powell J Delayed detection of cleft palate: an audit of newborn examination. Arch Dis Child. 2006; 91:238-240
Nurses Special Interest Group for Cleft Lip and Palate. (Accessed on 25 Feb 2010)
Glass RP, Wolf LS Feeding management of infants with cleft lip and palate and micrognathia. Infants and Young Children. 1999; 12:(1)70-81
Geddes DT, Kent JC, Mitoulas LR, Hartmann PE Tongue movements and intra-oral vacuum in breastfeeding infants. Early Human Develop. 2008; 84:471-477
Trahms CM, Pipes PL, 6th edn. New York, NY: WCB/McGraw-Hill; 1997
Lazarus D, Hudson D, Fleming A, Goddard E, Fernandes D Are children with clefts underweight for age at the time of primary surgery?. Plastic Reconstr Surg. 1999; 103:1624-1629
Jones WB Weight gain and feeding in the neonate with cleft: a three centre study. Cleft Palate J. 1988; 25:(4)379-384
Bowers E, Rosario F, Linton A, Whitaker P, Pasquariello D, Randell P General body growth in children with clefts of the lip, palate and craniofacial structure. Scand J Reconstr Surg. 1987; 21:7-14
Pandya AN, Boorman JG Failure to thrive in babies with cleft lip and palate. Br J Plast Surg. 2001; 54:471-475
Lee J, Nunn J, Wright C Height and weight achievement in cleft lip and palate. Arch Dis Child. 1997; 76:(1)70-72
Raynor P, Rudolph MCJ Anthropometric indices of failure to thrive. Arch Dis Child. 2000; 82:364-365
Sinclair-Smith C, Dinsdale F, Emery J Evidence, duration and type of illness in children found unexpectedly dead. Arch Dis Child. 1976; 51:424-429
Beaumont D A study into weight gain in infants with cleft lip/palate. Paediatr Nurs. 2008; 20:(6)20-23
The presence of a clinical nurse specialist within the multidisciplinary cleft team has become commonplace across many regions in the UK, with an aim to improve the quality of nursing care in this patient group. The role of the clinical nurse specialist may commence in the antenatal period, progress through birth and infancy, and extend into childhood in concurrence with the surgical procedures. The initial focus is on early feeding advice and management, and the provision of support to facilitate the exploration of feelings and anxieties in relation to the cleft.
Clinical Relevance: This paper enhances knowledge of cleft lip and palate, and an understanding of the Clinical Nurse Specialist's role within a multidisciplinary setting.
Article
The Clinical Standards Advisory Group (CSAG) reported on Cleft Lip and Palate services in England and Wales in 1998.1 In summary, the report showed outcomes at the time that were, at best, average when compared with outcomes in key European Cleft Centres. This subsequently led to a government directive to establish Regional Cleft Lip and Palate Services, with an aim to improve the quality and equity of care to this patient group. By adopting these recommendations, the number of cleft centres reduced to nine, each with a dedicated multidisciplinary team focusing on cleft lip and palate care, and surgeons undertaking a high volume of primary surgical procedures annually.1
During this process, it was acknowledged that new parents had a requirement for information, support and early feeding intervention. Prior to this change, nursing support for families was inconsistent and varied according to geographical location, whereas now it is commonplace for the clinical nurse specialist to be at the core of the multidisciplinary team, making that all important initial contact with parents. This paper explores the role of the clinical nurse specialist from the Leeds site of the Northern and Yorkshire Regional Cleft Lip and Palate Service, although many aspects of our team are now reflected widely across the country.
The primary role of the nurse focuses on early feeding management, the provision of information, and support throughout the primary surgical procedures. However, the nurse's role overlays and enhances those of other professionals within the team. The use of domiciliary visits encourages openness and discussion, which facilitates a professional relationship with the family, acting as their advocate where necessary. These occasions allow for the exploration of feelings and anxieties in relation to the cleft diagnosis, and with counselling and support many of these concerns can be normalized.
The cleft lip and/or palate can be present in isolation or be combined with other anomalies, for instance, cardiac, renal or limb malformations; or micrognathia, giving rise to varying degrees of airway obstruction. There are numerous syndromes associated with cleft lip and/or palate, some of which can be severe or life limiting syndromes, whereas others may be subtle and therefore not apparent at birth. Managing feeding and monitoring growth and development over the early months of the infant's life can highlight issues unrelated to the cleft, these can then be swiftly referred to the paediatrician for investigation. The nurse engages and communicates with the other clinicians involved in the care of these complex cases, thereby helping to promote a seamless approach across primary and secondary healthcare settings.
Antenatal diagnosis
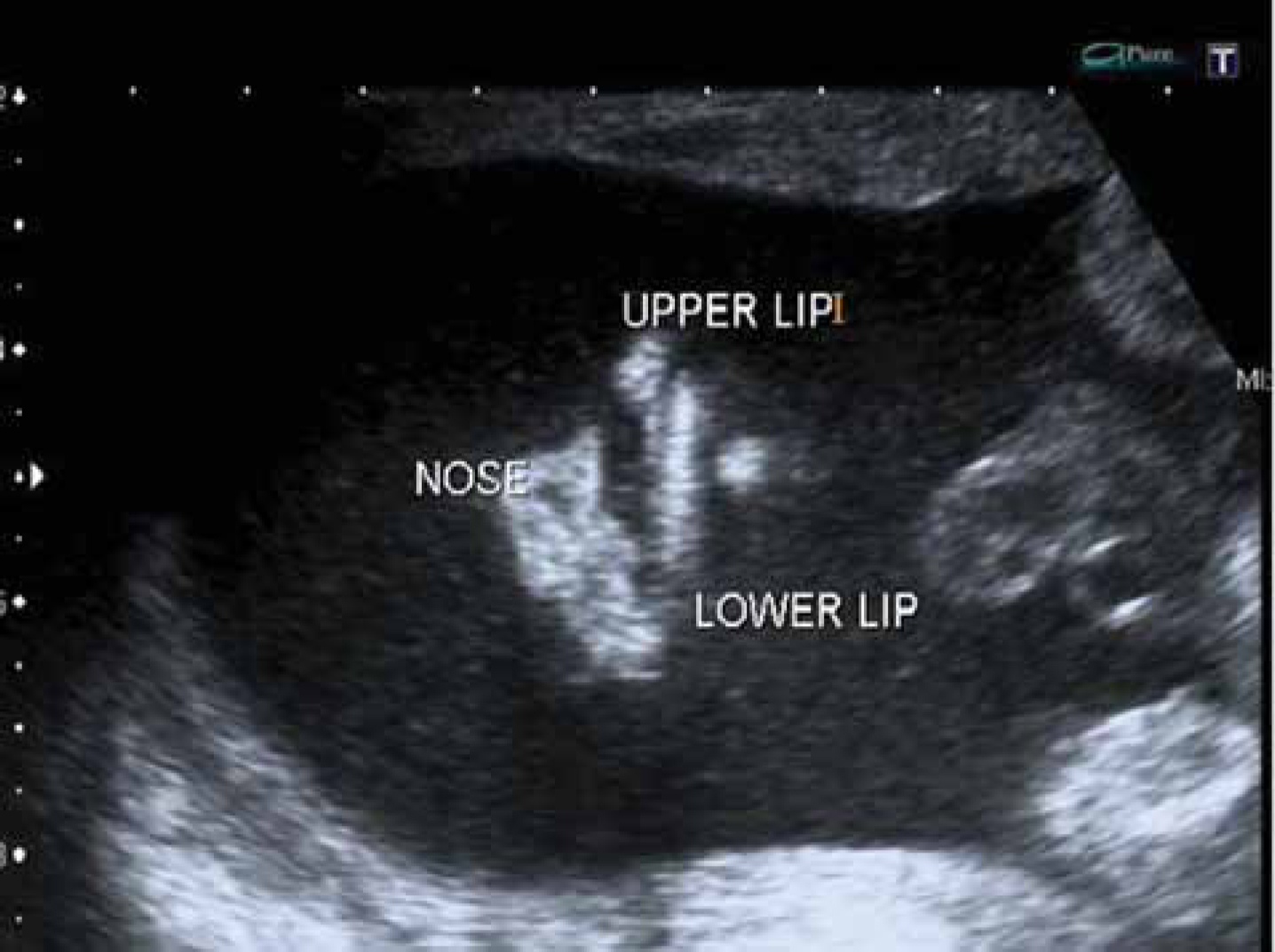
The diagnosis of a facial cleft in an infant may be made at the 20-week anomaly scan, with the findings being imparted immediately to the parents (Figure 1). This clearly can be an emotionally distressing time, and may initiate a mixture of feelings and reactions. At this point, there is a loss of the imagined child and a discrepancy is created between their expectations and reality, leading to a crisis reaction, typically feelings of grief and loss.2 Similarities are recognizable in the responses to bereavement and the reactions and phases parents progress through in accepting a child's anomaly, for instance, shock, denial, anger, equilibrium and reorganization.2,3 These phases describe mutual feelings and emotions of parents in similar situations, and may be present in a number of individuals, although not universal to all. The nurse's role begins at the time of the diagnosis, to offer further information and support so that, through discussion, many parents feel reassured to know these feelings are common to other parents in similar situations.
Figure 1. Antenatal: frontal view of nose and lips on ultrasound scan shows a left unilateral complete cleft lip and alveolus.
In the Yorkshire area, our protocol is for the local antenatal scanning units to refer to the cleft service following detection of a facial cleft. At this point the clinical nurse specialist makes contact with the mother within 24 hours to offer immediate support and information, and follows this with a domiciliary visit. The early detection of the cleft gives parents time to assimilate the information and prepare other family members. Many report, after the birth, that they were pleased they knew about diagnosis before the delivery, enabling them to adjust their thoughts, so they could begin caring for their infant immediately. Previous concerns that infants with a cleft lip and palate had an increased risk of insecure parental attachment have been challenged. It would appear that, despite an initial negative reaction, parents are able to adjust their thoughts and feelings, to develop acceptance of their infant with a facial cleft.4,5
During the antenatal period, care is taken to judge parental reactions and regulate the extent of information required on each occasion. The nurse discusses the possibility of palatal involvement, shows relevant pre- and post-operative photographs, and formulates a feeding plan with the parents and midwife. The plan takes into account the cleft type of the infant, and the bottle or breast-feeding preferences of the mother, and is placed into the maternity records. This gives midwifery personnel information to assist with initial feeding requirements of the infant prior to the arrival of the clinical nurse specialist after the delivery.
Postnatal care
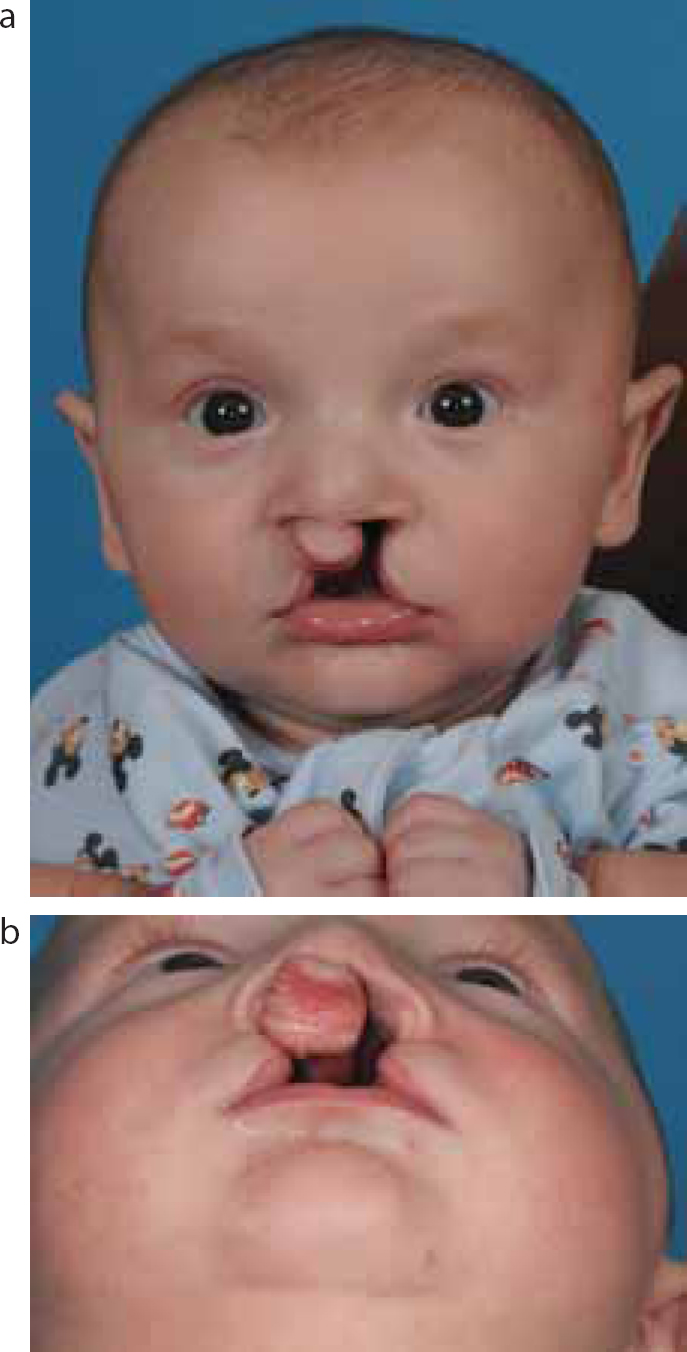
Not all facial clefts are detected in the antenatal period, along with isolated cleft palate, the diagnosis may not be made until after birth (Figure 2). At this point, parents have a requirement for information that is accurate and delivered sensitively. Many lose faith in healthcare professionals if conflicting or out-of-date information is provided then subsequently altered. For the infant with a cleft lip and/or palate, feeding poses an immediate concern for health professionals and parents, however, with the correct information, parents can begin the process of providing and caring for their infants.6
Figure 2.
(a, b) Infant with a bilateral complete cleft lip and palate. (Consent has been obtained to use these photographs.)
In cases of isolated cleft of the palate, the diagnosis may be overlooked on the initial birth examinations. A delay in diagnosis can lead to difficulties in feeding, a crying or unsettled infant, inadequate calorific intake and, eventually, failure to thrive, depending on the time interval before the cleft palate is detected. There have been reports of delays in diagnosis ranging from days or weeks, even to several years. Out of 344 cases of isolated cleft palate, 12% were diagnosed beyond 8 days.7 Parents are frequently and justifiably angry at this lapse, many reporting feelings of frustration in their inability to feed their infant, some have even sought legal redress. Therefore, it is recommended when examination of the palate takes place after birth, that the palate is viewed along its complete length, using a good light source, with the tongue depressed, and an assistant holding the infant in position.7
Once the cleft has been identified, a referral is made to the service, where our protocol is for the nurse to visit the newborn within 24 hours. This protocol is part of a set of nationally agreed nursing standards for the care of infants with a cleft.8 These standards aim to improve the quality and equity of nursing care across the country, and focus around prompt provision of information specific to the cleft type, feeding assessment and parental feeding preferences. Our aim is to keep the post-natal care as standard as possible, keeping the mother and baby together on the postnatal ward, whilst being sensitive to those mothers who wish for some privacy away from other parents whilst they adapt to their new infant.
Parents and families may seek additional information from other sources, commonly the Internet or friends. The Cleft Lip and Palate Association (CLAPA) is routinely recommended to families as an excellent British resource. An introduction to a parent support group may be positive for some individuals, as a place to meet other parents whose children have undergone surgery and share experiences. The nurse may co-ordinate this process, although caution is needed when matching families to one another, to ensure similarity of cleft types, coping strategies and ages of children.
Infant feeding
In order to feed adequately, all infants have to co-ordinate sucking, swallowing and breathing. The sucking action draws the milk into the mouth by means of two pressure gradients. The first is positive pressure; this is where compression on the teat or nipple causes ejection of milk on to the tongue. The second is by negative pressure or suction, which arises when the oral cavity is sealed off from the nasal cavity by means of the soft palate, which enlarges slightly, thus drawing milk into the tongue.9 At the breast, suction is required to latch on and maintain the nipple in the infant's mouth, where both types of pressure play a part in milk flow.10 The tongue channels milk along a central groove towards the pharynx, the soft palate is raised, closing off the nasal cavity, and a swallow is triggered. Breathing is suspended during swallowing, as the airway is protected by the closure to the vocal folds and epiglottis.
Once the mechanism of normal feeding is understood, it is clear to see how an infant with a cleft has difficulty accomplishing this. The oral cleft impacts on the infant's ability to achieve the level of suction required for successful oral feeding. A cleft in the lip allows air to enter the mouth, breaking the seal around the teat. When there is a cleft of the palate, the nasal and oral cavities are shared, therefore the infant is unable to create a vacuum, despite displaying the correct tongue and jaw movements. This can result in prolonged feed times, tiring the infant before the feed is completed.10 Growth in infancy is primarily a nutritionally driven process, with biological and psychosocial factors having an additional effect.11 Therefore, if an infant is unable to achieve adequate nutritional intake, growth will be adversely affected.
Historically, infants with a cleft lip and/or palate have presented with poor growth and failure to thrive, thought to be associated with early feeding difficulties.12,13,14 Failure to thrive rates have been reported to be up to 49% for infants with a non-syndromic cleft presentation, and up to 100% for those with Pierre Robin Sequence.15,16 Severely compromised growth can have a detrimental affect on health, with an increased risk of lasting growth deficits, developmental delay,17 and cot death.18 Within our region, where regular nursing input and feeding management has been undertaken since 2002, the outlook appears to be improving. A recent review of weight gain in infants appears to show a significant reduction in failure to thrive rates compared with previously reported studies.19
Prior to the initiation of feeding, an assessment of the infant's oral skills should be undertaken. This involves consideration of the following:
Maternal and obstetric history;
Oral examination of the infant;
Cleft type and other anatomical anomalies, such as micrognathia;
Tongue position;
Presence or absence of oral reflexes; and
Ability to co-ordinate suckling.
Where it is safe to proceed with oral feeding, the nurse advises on the most appropriate method of feeding, taking into account the infant's skills and the maternal preference.
Feeding methods
In general, infants with an isolated cleft lip, with an intact palate, may feed successfully using standard feeding methods. These infants can be effective breast-feeders, with the breast tissue moulding into the alveolar defect, thus achieving a seal and successful latching. Those mothers who choose to bottle-feed may use a standard bottle and an easily compressible latex teat. However, the nurse should monitor progress with this method, as some infants are unable to form a seal with the upper alveolar ridge against the teat, resulting in loss of suction. This would present with the infant being slow to feed, taking inadequate milk volume and lead to poor weight gain. An adjustment in the type of teat utilized may be all that is required to overcome this issue.
Where the cleft involves the palate, most infants require assistance in obtaining sufficient volumes of milk. For those wishing to breast-feed, the infant may be put to the breast for comfort and suckling, but will be unable to stabilize the nipple for compression or generate a sufficient vacuum to aid milk flow from the breast.10 Supplemental milk is given to the infant after each breast-feed using a soft squeezable bottle and latex teat. The milk can be expressed breast milk or formula, whichever is the mother's preference. Many cleft units have a supply of electric breast pumps that can be offered on free loan, along with an initial supply of feeding bottles.
The parents are shown by the nurse how to ‘assist feed’, by gently squeezing the soft bottle in time with the infant's suckling rhythm, being directed to regulate the flow and observe the infant for cues of distress. If milk flow is too fast and the infant's cues are overridden, there is a potential for aspiration. It is standard practice to feed the infant in a semi-upright position, which should reduce nasal regurgitation of milk. In addition, regular ‘winding’ of the infant can alleviate bloating, as air is swallowed during feeding.9 Most parents respond positively to advice offered and become practised at this technique within a few days.
The older child
During these periods of contact, the treatment pathway and details of surgical procedures are explored, so the family has information to enable them to care for their child in the pre- and post-operative period. The nurse aims to encourage compliance with treatment protocols, thereby promoting wound healing, whilst ensuring a smooth progression through the hospital stay and continuing care in the community. Discussion generally centres around the practical aspects of a hospital admission, and on post-operative management. However, the nurse can highlight any issues of concern that may arise around surgery, hopefully alleviating the usual anxieties around anaesthetics or pain relief.
As the child matures, further surgical interventions may be required, such as surgery to improve speech, or alveolar bone grafts. The nurse adapts pre- and post-operative information for the child and family specific to each procedure. If, during this process, significant issues are brought to light, particularly around needle or hospital anxiety, then referral to the team psychologist may be more appropriate.
Conclusion
The presence of a clinical nurse specialist as a principal member of the multidisciplinary cleft team has now been emulated in many regions across the UK, as a process to improve the quality of nursing care in this patient group.8 As a highly skilled practitioner, the nurse is the designated team member who makes initial contact to offer care and support to expectant or new parents. The role of the clinical nurse specialist may commence in the antenatal period, progress through birth and infancy, and extend into childhood in concurrence with the surgical procedures. The initial focus is on early feeding advice and management, and the provision of support to facilitate the exploration of feelings and anxieties in relation to the cleft. This care is provided to all, regardless of geographical location from our regional centre, thereby ensuring equity of provision.