Bardach J, Eisbach KJ. The influence of primary unilateral cleft lip repair on facial growth. Cleft Palate J. 1977; 14:88-97
Mars M, Houston WJB. A preliminary study of facial growth and morphology in un-operated male unilateral cleft lip and palate subjects over 13 years of age. Cleft Palate-Craniofac J. 1990; 27:7-10
Sandy J, Williams A, Mildinhall S, Murphy T, Bearn D, Shaw B, Sell D, Devlin B, Murray J. The Clinical Standards Advisory Group (CSAG) Cleft Lip and Palate Study. Br J Orthod. 1998; 25:21-30
Vallino L. Speech, velopharyngeal function, and hearing before and after orthognathic surgery. J Oral Maxillofac Surg. 1990; 48:1274-1281
Guyette T, Polley J, Figueroa A, Smith B. Changes in speech following maxillary distraction osteogenesis. Cleft Palate Craniofac J. 2001; 38:199-205
Kummer A, Strife J, Grau W, Creaghead N, Lee L. The effects of the Le Fort 1 osteotomy with maxillary movement on articulation, resonance and velopharyngeal function. Cleft Palate J. 1989; 26:193-200
Chanchareonsook N, Whitehill T, Samman N. The effect of cranio-maxillofacial osteotomies and distraction osteogenesis on speech and velopharyngeal status: a critical review. Cleft Palate Craniofac J. 2006; 43:477-487
Watzke I, Turvey T, Warren D, Dalston R. Alterations in velopharyngeal function after maxillary advancement. J Oral Maxillofac Surg. 1990; 48:685-689
Okazaki K, Satoh K, Kato M, Iwanami M, Ohokubo F, Kobayashi K. Speech and velopharyngeal function following maxillary advancement in patients with cleft lip and palate. Annals Plastic Surg. 1993; 30:304-311
Janulewicz J, Costello B, Buckley M, Ford M, Close J, Gassner R. The effects of Le Fort 1 osteotomies on velopharyngeal and speech functions in cleft patients. J Oral Maxillofac Surg. 2004; 62:308-314
Cunningham SJ, Hunt NP, Feinmann C. Perceptions of outcome following orthognathic surgery. Br J Oral Maxillofac Surg. 1996; 34:210-213
Cunningham SJ, Feinmann C. Psychological assessment of patients requesting orthognathic surgery and the relevance of body dysmorphic disorder. Br J Orthod. 1998; 42:293-298
Williams RW, Travess HC, Williams AC. Patients' experiences after undergoing orthognathic surgery at NHS hospitals in the south west of England. Br J Oral Maxillofac Surg. 2004; 42:419-431
Modig M, Andersson L, Wardh I. Patients' perception of improvement after orthognathic surgery: pilot study. J Oral Maxillofac Surg. 2006; 44:24-27
Boyne PJ, Sands N. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg. 1972; 30:87-92
Abyholm FE, Bergland O, Semb G. Secondary bone grafting of alveolar clefts. A surgical/orthodontic treatment enabling a non-prosthodontic rehabilitation in cleft lip and palate patients. Scand J Plast Reconstr Surg. 1981; 15:127-140
Jones ML, Sugar AW. The late management of cleft lip and palate problems: a joint orthodontic/surgical approach. J Royal Coll Surg Ed. 1990; 35:376-386
Sugar AW, Honigmann K. Reconstruction of cleft lip and palate osseous defects. In: Greenberg A, Prein J (eds). New York: Springer; 2002
Sugar AW, Samuels R, Jones M, Bocca A, Newton C. Results of a modified cleft versus non-cleft maxillary osteotomy. Int J Oral Maxillofac Surg. 1999; 28
Eales EA, Newton C, Jones ML, Sugar AW. The accuracy of computerised prediction of the soft tissue profile: a study of 25 patients treated by means of the Le Fort I osteotomy. Int J Adult Orthod Orthognath Surg. 1994; 9:141-152
Eales EA, Jones ML, Newton C, Sugar AW. A study of the accuracy of predicted soft tissue changes produced by a computer software package (COG 3.4) in a series of patients treated by the Le Fort 1 osteotomy. Br J Oral Maxillofac Surg. 1995; 33:362-369
Smith AT. The use of orthodontic chain elastic for temporary intermaxillary fixation. Br J Oral Maxillofac Surg. 1993; 31:250-251
Henderson D, Jackson IT. Naso-maxillary hypoplasia: the Le Fort II osteotomy. Br J Oral Surg. 1973; 11:77-93
The orthognathic management of cleft lip and palate skeletal discrepancy: CLP series part 9 Helen Extence Vanessa Hammond Jenny Hunt Adrian Sugar Orthodontic Update 2025 7:1, 15-22.
Consultant and Lead Clinical Psychologist, South Wales Regional Cleft Lip and Palate Service, South Wales South West Managed Clinical Network for Cleft Lip and Palate.
A patient with a repaired cleft of lip and/or palate (CLP) may develop dentofacial disproportion, classically a Class III skeletal and inter-arch relationship, due to an underlying maxillary hypoplasia. The definitive correction of the dental and facial aesthetic and functional problems associated with this anomaly requires a multidisciplinary input involving orthodontists, surgeons, speech therapists and psychologists. A successful outcome is dependent on a close working relationship between these disciplines and a planned care pathway that is adapted to patient needs. This paper outlines such a care pathway.
Clinical Relevance: This paper offers the clinician an understanding of a multidisciplinary approach to the orthognathic management of a patient with cleft lip and palate.
Article
All elements of orthodontic management included in the care pathway of a patient with a repaired cleft of lip and/or palate (CLP) should be mindful of the potential for the development of facial disharmony and compromised inter-arch relationships during growth. Such skeletal discrepancies may be completely unrelated to the original congenital defect. However, previous lip or palatal surgery1,2 has been cited as a possible cause of abnormal maxillary growth which requires orthognathic correction.
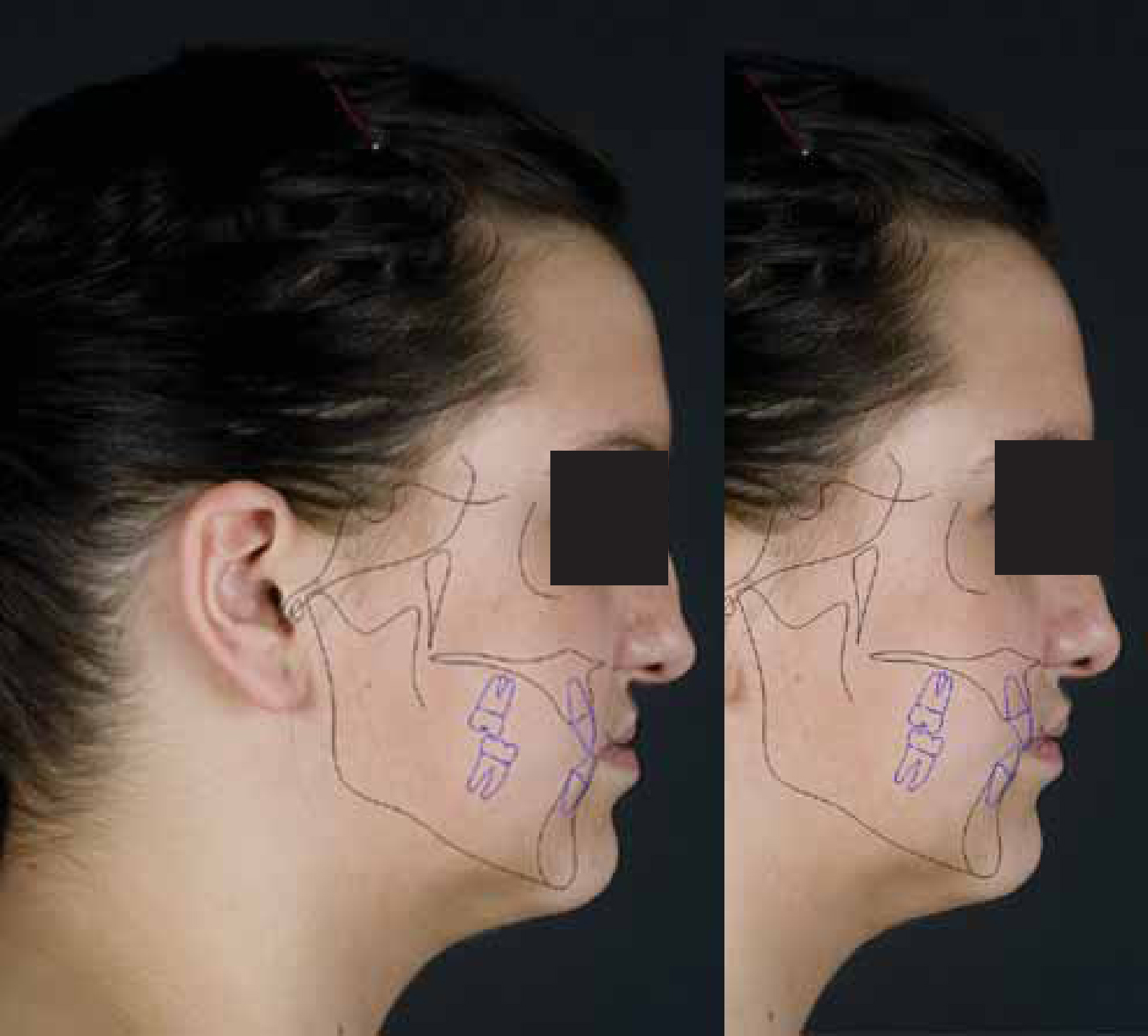
The skeletal relationship, classically associated with CLP, is a Class III discrepancy that is characterized, predominantly, by maxillary antero-posterior deficiency. Although a range of Class II discrepancies may be associated with clefts of lip or palate, this discussion will focus on the management of Class III problems. Where skeletal discrepancies are mild or moderate, the opportunity for orthodontic camouflage exists through maxillary labial segment advancement and mandibular labial segment retraction. Such approaches before adulthood should never involve mandibular tooth loss as growth prediction in CLP cases is notoriously difficult, and unfavourable late facial growth can sometimes present facial and dental relationships that can only be managed orthognathically (Figure 1). It is, therefore, important to consider the potential orthognathic needs of a patient before beginning a definitive orthodontic treatment plan. Where later orthognathic management is possible, early orthodontic interventions should ideally be limited to maxillary arch alignment alone.
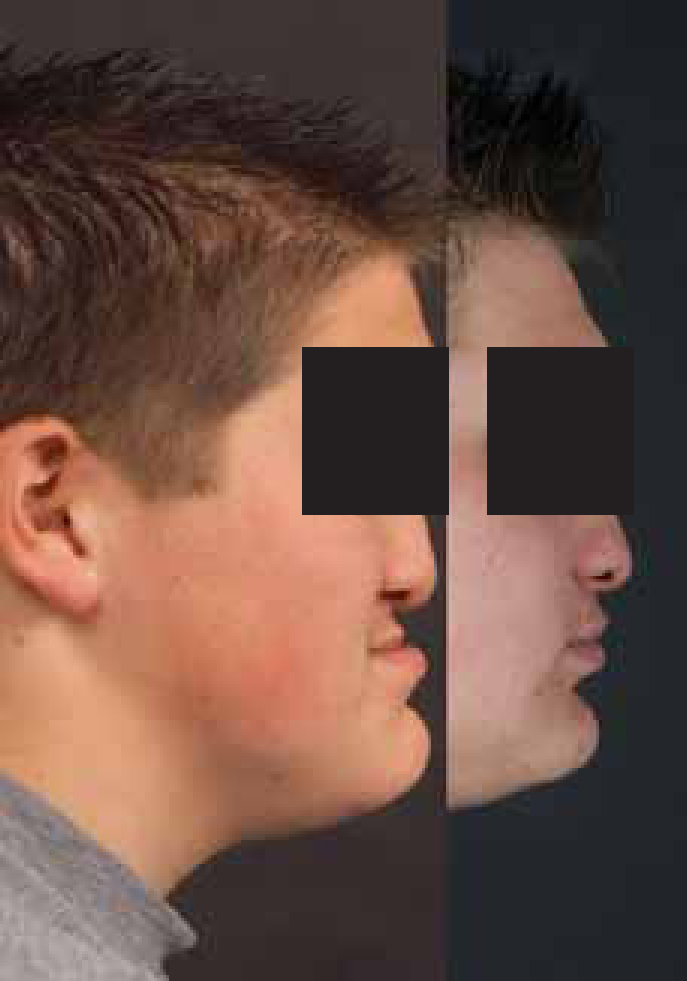
Figure 1. Facial profile at 10, 15 and 18 years showing unfavourable and unpredictable facial growth.
The use of orthognathic surgery rates as an indicator of the incidence of skeletal III discrepancy in CLP patients is unreliable, relying as it does on surgeon/orthodontist interest and expertise, patient wishes, as well as the cost and availability of surgery. Nevertheless, some objective view is available from the UK NHS Clinical Standards Advisory Group report (1998, HSC 1998/002),3 which looked at all children born in the UK during specific time periods with non-syndromic complete unilateral cleft lip and palate (UCLP). This independent report showed that 80% of the 12-year-old cohort of UCLPs demonstrated Class III incisor relationships suggesting existing, and potentially increasing, Class III skeletal tendencies.
The correction of significant skeletal discrepancy demands a combined orthodontic and surgical approach with input from speech and language therapy, psychology, maxillofacial technology and, sometimes, restorative dentistry. This paper outlines this care pathway.
Early decisions
The objectives of orthodontic care leading to the orthognathic management of a Class III skeletal discrepancy are:
Dental alignment;
The co-ordination of symmetrical arch forms;
The delivery of labial segment inclinations that will facilitate the skeletal movements required to promote optimum facial aesthetics.
The achievement of orthodontic objectives during CLP orthognathic care may be complicated by associated congenital and acquired dental anomalies and the limitations imposed by previous surgery.
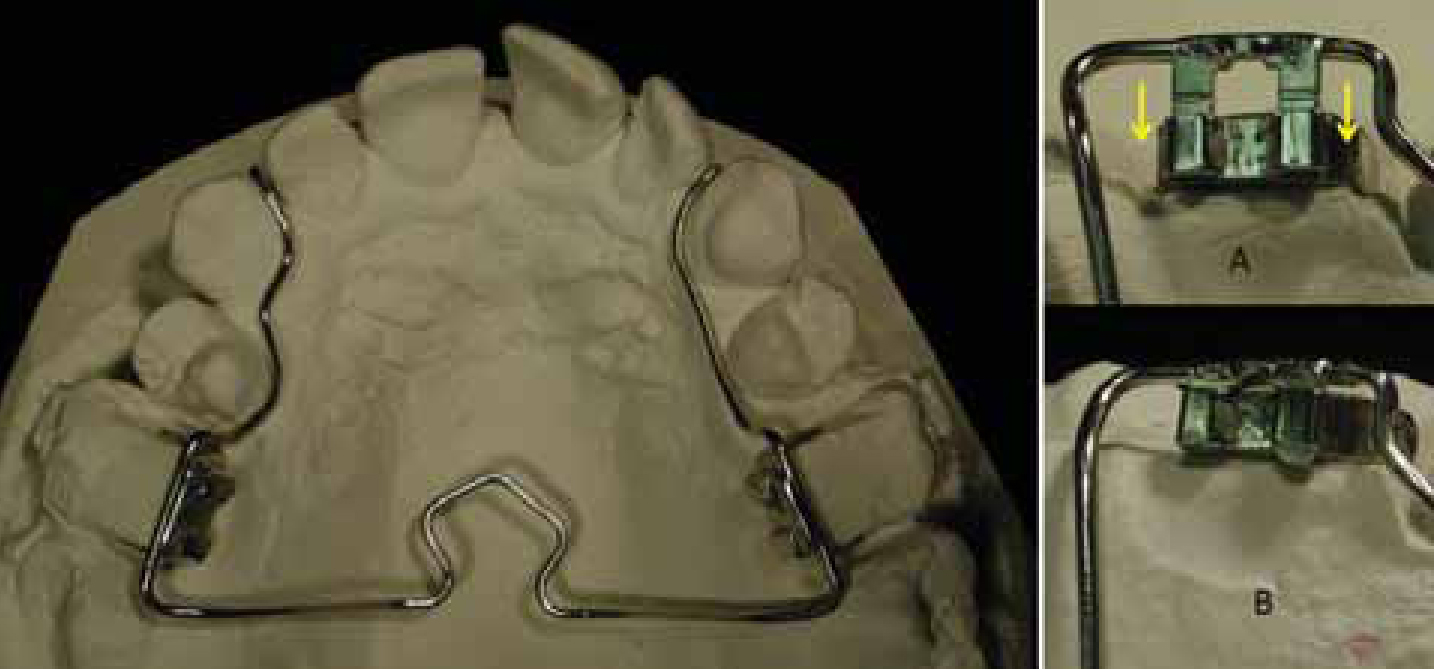
The requirement for maxillary arch expansion should be considered before alveolar bone grafting, not only to address segment collapse and facilitate surgical access, but also with an eye to the degree of expansion that may be required for arch co-ordination as part of a later orthognathic plan. Where this is not done, palatal scarring may limit the expansion that can be achieved and the potential for inducing palatal defects, especially fistulae, may be increased. The retention of arch expansion following the alveolar bone graft is important during the healing phase. This may involve the use of trans-palatal arches (TPA) to maintain transverse buccal segment relationships and, in bilateral cases, labial stabilizing arches (Figure 2) to maintain the position of the pre-maxilla. The placement of trans-palatal and labial stabilizing arches has to be considered at the end of the expansion phase and before ABG surgery. A removable design of TPA and pre-fabricated labial arch (Figure 3) offers the surgeon complete access to the palate if the TPA is removed during the surgery, for example to repair fistulae, and can be replaced in theatre at the end of the procedure as a more efficient means of post-surgical stabilization.
Figure 2. Segment stabilization in BCLP before/after alveolar bone graft.Figure 3. Removable design TPA (Knox J in Sugar AW. AOCMF Surgery reference on congenital deformities, cleft lip and palate. www.aocmf.org, 2012).
Dental anomalies such as dilacerations, enamel hypoplasia, ectopic tooth development, congenital or acquired hypodontia, supernumerary teeth, microdontia and tooth transposition may influence orthodontic management through the introduction of tooth size or arch length discrepancies. If these anomalies are managed early in the care pathway, consideration must be given to the effect of that intervention on arch symmetry and labial segment inclination. For example, where a maxillary lateral incisor is congenitally absent, the decision to replace the unit prosthetically may enhance an orthodontic camouflage treatment plan, whereas a decision to close the space will influence arch symmetry, if considered in isolation, or retrocline the maxillary incisors, if accompanied by loss of a unit and space closure in the opposing quadrant to promote dental symmetry.
And so a number of decisions and interventions made early in the CLP care pathway will have an impact on the later orthognathic management of an individual. These include:
The achievement of good maxillary arch expansion before alveolar bone grafting;
The delivery of a good and robust alveolar bone graft;
Careful management of arch crowding and spacing.
Orthognathic planning
For some patients, the development of significant Class III skeletal and inter-arch relationships is evident at an early age, allowing long term planning. For others (Figure 1), the requirement for an orthognathic intervention presents much later.
Orthognathic planning must always follow a structured diagnostic process with consideration given to the patient's presenting complaint (the presence of a significant Class III skeletal discrepancy must not automatically initiate an orthognathic treatment plan). Within this process there should be a complete evaluation of the patient's facial appearance, speech, psychological status and ability to sustain and support a combined orthodontic and surgical procedure.
Speech considerations
Surgical maxillary advancement may have an effect on articulation and velopharyngeal function. It is generally recognized that articulation often improves following maxillary advancement, in particular anterior errors such as s, z, sh, ch and j, due to a more favourable jaw and labial segment relationship which promotes improved labio-lingual and lingual-dental relationships.4,5,6
However, when surgical maxillary advancement is planned, the impact on velopharyngeal function must be taken into consideration. Most patients have sufficient compensatory reserve to ensure adequate velopharyngeal closure following maxillary advancement. However, a patient with a cleft palate may have a reduced ability to compensate as a result of scarring, short soft palate or an increased nasopharyngeal depth. Where maxillary advancement alters the velopharyngeal sphincter beyond its ability to compensate, velopharyngeal dysfunction may result with associated speech characteristics of hypernasal resonance, nasal emission, nasal turbulence and weak pressure consonants.
There have been a number of studies investigating the effects of maxillary advancement on speech. Chanchareonsook et al7 reviewed the available literature and reported that 12 of the 39 studies reviewed concluded that maxillary advancement did not have a detrimental effect on velopharyngeal function, whereas 15 studies demonstrated a deterioration.6,8,9
When patients with cleft palate are being considered for maxillary advancement, the Specialist Speech and Language Therapist should evaluate speech pre-operatively and counsel the patients and other team members regarding the possibility of resonance deterioration following the procedure. Patients who have articulation errors associated with a Class III malocclusion can be advised that these errors are likely to improve spontaneously following the correction of the malocclusion without the need for therapy. Patients should also be counselled about the risks of changes in resonance due to altered velopharyngeal function.
Some units throughout the UK perform nasendoscopy, videofluoroscopy and nasometry, in addition to a perceptual speech assessment, in an attempt to predict velopharyngeal function post advancement. It has been suggested by some authors10 that patients with borderline hypernasality pre-advancement may be more at risk of developing velopharyngeal dysfunction post advancement.
Psychological assessment pre-treatment and surgery
There has been a growing recognition of the need for pre-treatment and pre-surgery psychological assessment for cleft patients considering orthognathic surgery. The assessment should involve screening in a number of areas, preparation and psychological intervention when required. The Special Interest Group (SIG) of psychologists working in cleft services have recently developed a national protocol for the psychology input in the care of cleft patients undergoing orthognathic surgery which aims to ensure that the psychological needs of patients are met, as well as providing a framework which allows for the collection of prospective data.
At the pre-treatment stage, the assessment looks at the decision-making process, including a patient's motivations for opting for surgery and his/her expectations. Patients who have unrealistic expectations of surgery have been found to report greater dissatisfaction with the outcome of surgery.11 Expectations of surgery in terms of impact on appearance, as well as impact on other factors, including confidence, mood and self-esteem, need to be assessed. It is also important to assess the views of other significant people in the patient's life in relation to the potential treatment and surgery. Social and family support is a key factor in terms of satisfaction with outcome and adjustment.12 The pre-treatment stage is an appropriate point to begin to discuss adjustment to changes in appearance, including coping with and preparing for the reactions, comments and questions of other people.
Assessment should also include discussion of the process of treatment and surgery. The quality of information provided, in relation to the process of treatment and surgery, is known to be a predictor of outcome and satisfaction,13,14 and psychological assessment can include checking a patient's understanding and knowledge about pre-surgical treatment, surgery and information about the post-operative effect of the surgery. The psychologist can then work collaboratively with the patient to agree the best route to supplement this knowledge, through discussion, liaison, advocacy and empowerment. Discussion should also include specific issues in relation to surgery and hospital treatment, including any specific fears or phobias, such as needle phobia, and coping strategies. Intervention, including direct work with the patient, as well as liaison with members of the MDT and ward staff, may be required.
A final area of assessment is formally to assess psychological factors, including mood and anxiety. This mental health screen may contribute to the identification of other significant disorders, such as body dysmorphic disorder (BDD) or major depression, which would require further assessment and treatment by appropriate mental health services. Indeed, such findings may be a contra-indication to surgery.
The psychological assessment can then feed back into the discussions with the patient and the MDT in terms of planning treatment. Further psychological intervention can be offered if required, either prior to or alongside treatment, by other members of the MDT as appropriate.
Choice of surgical approach and consent
The informed consent process must include a description of all risks inherent in an orthognathic treatment plan. For a CLP patient, additional information needs to be provided on the likely effect the procedure may have on speech, the requirement for bone grafting and the use of any distraction devices. To help a patient visualize treatment objectives, video photographic imaging may be a useful tool to demonstrate proposed profile changes (Figure 4).
Figure 4. 2D videosimulation.
The Class III skeletal defect associated with CLP may be gross and due entirely to a maxillary deficiency which should, ideally, be corrected entirely by maxillary advancement. In some centres, maxillary advancement is limited to around 10 mm, with any of the residual discrepancy managed through a mandibular setback. This inevitably results in a degree of compromise that can, with careful planning and technique, be avoided.
Successful CLP maxillary advancement requires that the maxilla is always in one solid piece at the time of osteotomy. This is achieved by a policy of alveolar cleft bone grafting shortly before the eruption of the permanent maxillary canine tooth on the cleft side(s).15,16 When an alveolar cleft bone graft has not been successfully carried out previously, a late or tertiary bone graft is performed to achieve the same, or similar, end.17
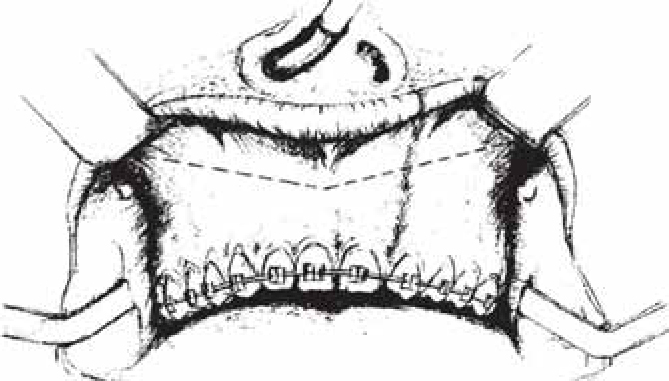
A modified surgical incision (Figure 5), which starts 5 mm anterior to and 5 mm superior to the parotid duct on one side and finishes in an identical position on the opposite side, by providing improved blood supply to the osteotomized maxilla, aids maxillary mobilization and advancement. This, combined with robust fixation and bone grafting, has offered safe and reliable results with excellent stability.18 This study demonstrated better stability in 24 consecutively treated modified cleft osteotomy cases than in non-cleft maxillary advancement19 or in cleft cases managed by internal distraction osteogenesis.
Figure 5. Modified Le Fort 1 incision.
Orthodontic preparation
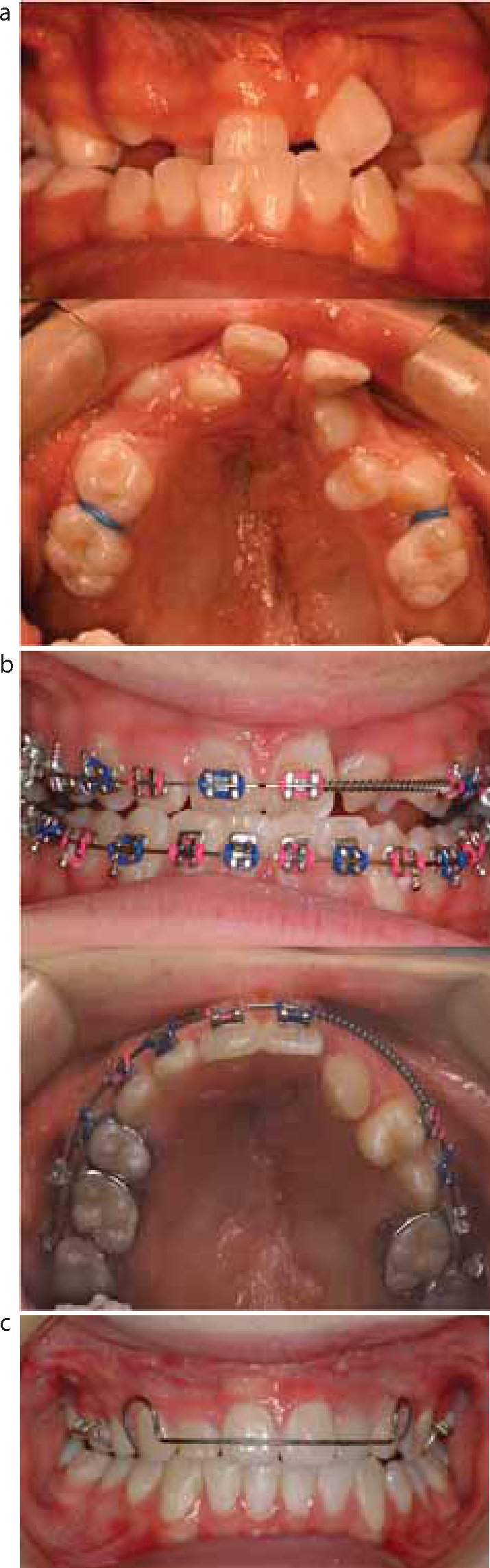
Orthodontic preparation must deliver ideal arch alignment, sufficient maxillary arch expansion to deliver good transverse buccal segment relationships after maxillary advancement, and a good relationship between dental and skeletal midlines (Figure 6). At the same time, labial segment inclinations must be prescribed that will facilitate the skeletal movements required to promote optimum facial aesthetics.
Figure 6. Space management dilemma. (a) Missing UL2, 5 (transposed UL4,3) with centerline displaced to left and Class III incisors. (b) Loss of UR4 to facilitate centerline correction but increasing Class III incisor relationship. (c) Orthognathic correction of Class III inter-arch relationships.
Labial segment inclinations and arch symmetry will be determined largely through the management of arch crowding and spacing. Incisor inclinations can be modified further through inter-arch mechanics, third-order archwire bends or bracket prescriptions, or mechanics supported by Temporary Anchorage Devices. However, aiming for cephalometric normative values for incisor inclinations, and Class I incisor relationships after surgery, will not always deliver optimal facial results. There is sometimes a limit to the degree of incisor inclination change possible and a slightly Class II inter-arch relationship following surgery will sometimes offer additional lip support and improved facial aesthetics (Figure 7).
Figure 7. Prescription of increased overjet to improve upper lip support during CLP maxillary advancement.
Pre-operative planning
The planning of orthognathic surgery in CLP patients usually starts following an initial consultation with an individual member of the cleft team. The optimum time to discuss the orthognathic treatment plan is around the age of 15 years. However, in a well structured CLP protocol, the possible need for an orthognathic approach may have been raised with the child and his/her parents at an earlier time. Despite this, there will always be older patients who will return, either because their deformity has become worse, or because they have changed their minds and decided that they want to progress with such surgical care. Even older patients, from earlier generations of cleft care, will sometimes return to the team with concerns of which skeletal discrepancy is part of the problem.
During planning, the identification of a patient's own concerns and motives for treatment must be identified. In the younger group, these must be considered over and above the concerns and wishes of the parents. Discussion about the changes that can be achieved and their desirability should take place initially and primarily with the cleft surgeon and the cleft orthodontist. It is helpful to provide printed leaflets about orthognathic treatment and to encourage the patient to make a written note of any questions he/she may have and about concerns.
This initial consultation should also be followed by a speech assessment in which the potential risk to, and benefit of, surgery to speech can be considered and, if possible, evaluated. A psychological evaluation, in which a patient's concerns can be identified and an assessment of his/her ability to cope with the proposed procedure, should follow.
These consultations should lead to a joint consultation with all members of the team in which the patient has the opportunity to ask questions and consider his/her wishes. Patients should never be coerced into such a decision as, to a large extent, orthognathic treatment is not age dependent and can be delayed for years.
No planning of orthognathic surgery should take place without a full record of the patient's medical history and a documented clinical assessment of the patient facially and the recording of certain critical measurements (eg dental midlines related to the facial midline, upper incisor exposure, inter-alar distance, etc). 2D computerized planning (Figure 4), based on digitized lateral cephalograms and both hard- and soft-tissue prediction, has become a routine in orthognathic surgery and is equally valuable for orthognathic surgery in CLP patients. There are some small differences in soft-tissue changes, especially of the upper lip in CLP cases, but in general the predictions are reasonably reliable and helpful.20,21 This type of planning can also produce a 2D lateral facial image, with a prediction of the changes achievable, which can often be helpful to patients. 3D surface scanning (for example using stereophotogrammetry) is also a useful and non-invasive way of monitoring the 3D changes achieved.22
Such plans then need to be transferred to dental models mounted on an anatomical articulator so that the planned surgery can be executed on them. Precise measurements can be recorded for the aid of the surgeon at operation and, from the model movements, surgical splints (wafers/stents) can be constructed so that the jaws can be precisely located at operation in the antero-posterior and transverse dimensions. Vertical changes are largely determined by the clinical measurement of incisor exposure and are in the hands of the surgeon, who must ensure that he uses a point of reference for any changes (eg a screw inserted at the beginning of surgery in the glabella and from which the maxillary height can be measured).
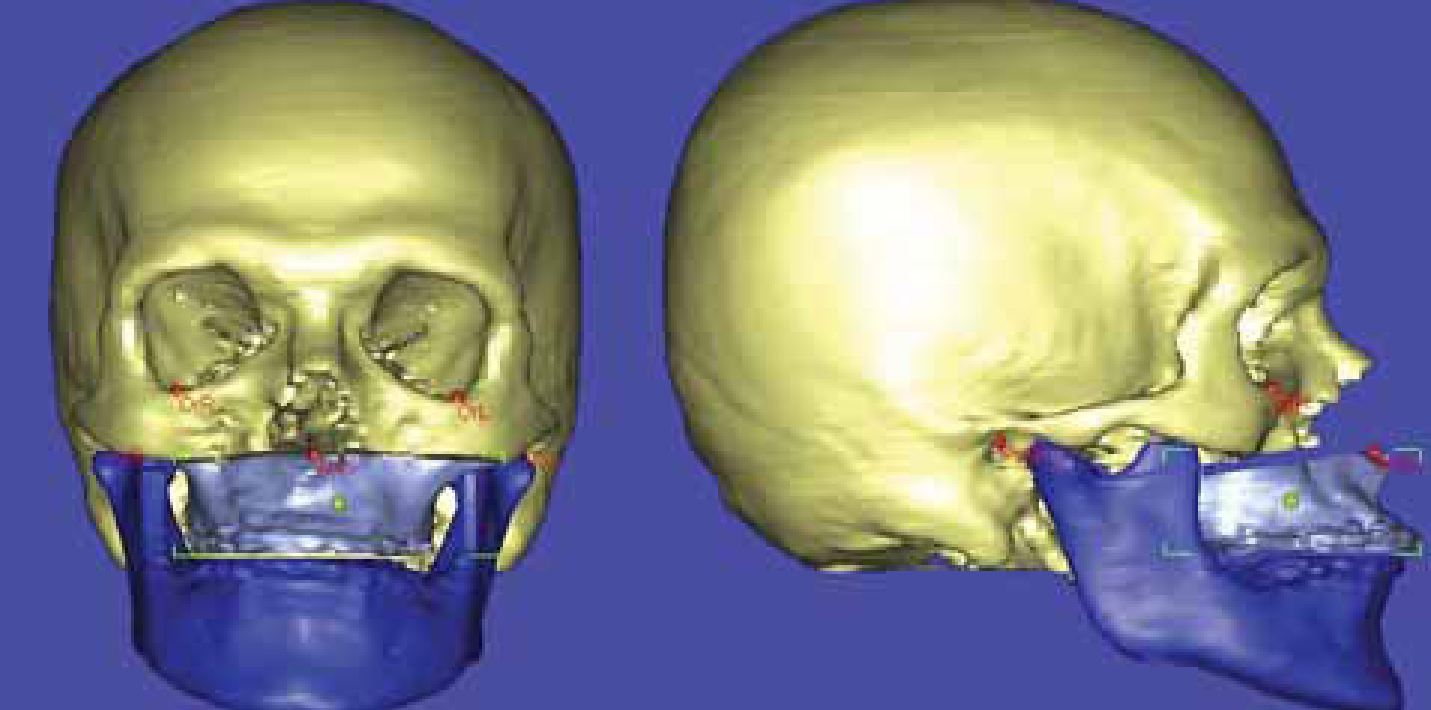
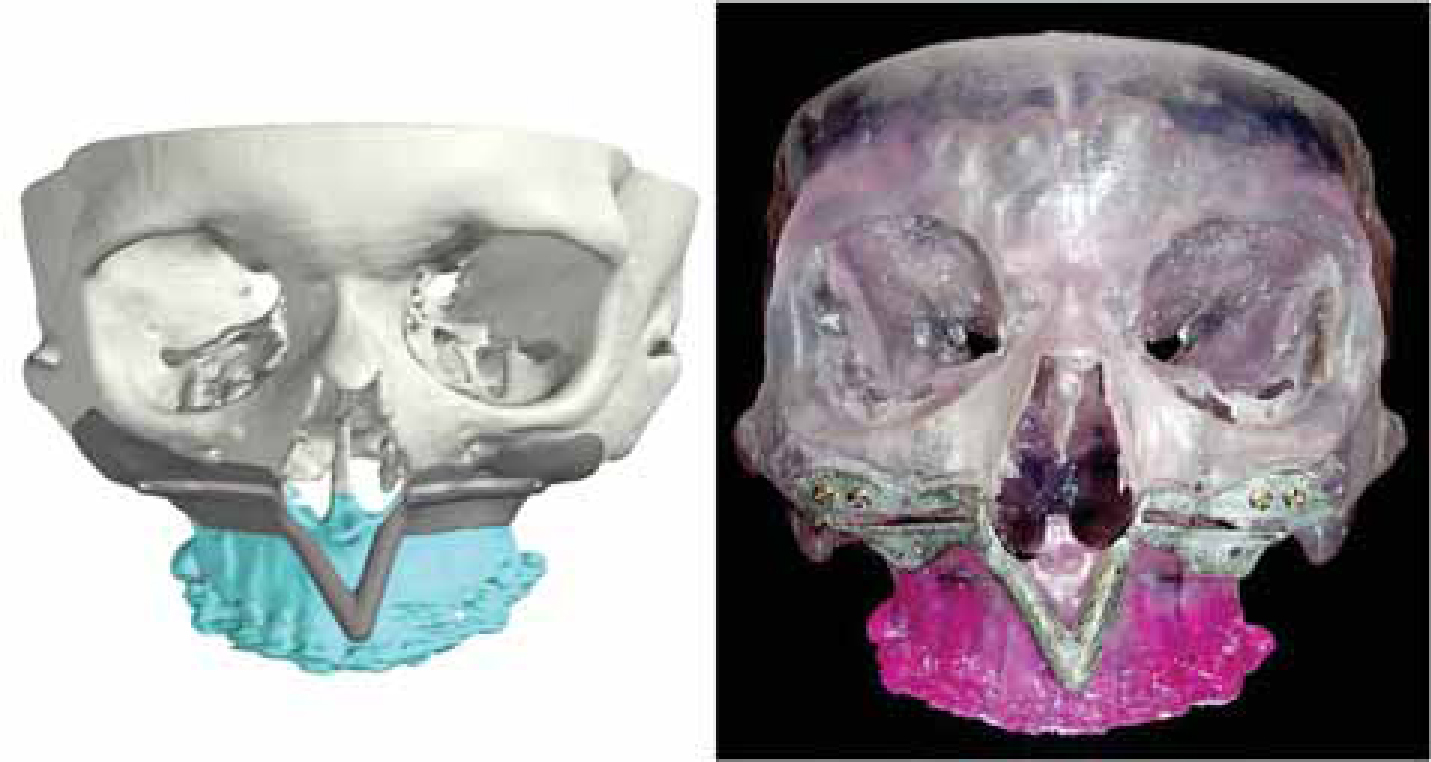
3D planning is also possible using either multislice CT or cone beam CT scans (Figure 8). Such scans (usually as DICOM format data) can be imported into planning software in which virtual surgery can be carried out on screen. It is also possible to obtain physical models from this data using one of a number of methods of rapid prototyping (Figure 9). These models are useful for planning, particularly in cases requiring internal distraction osteogenesis, where prescription of distractor shape and adaptation, vector visualization, and distractor positioning guide construction can be facilitated (Figure 9). Such 3D planning is usually not necessary in routine CLP orthognathic surgery, although it is an invaluable tool for complex syndrome cases and for the correction of gross facial asymmetry. It is also possible using such technology to construct dental splints/wafers/stents through rapid prototyping in the planned jaw/teeth positions.
For the purposes of this article, only mid-face surgery will be considered as surgery to the mandible, including the chin, is not substantially different from that in non-cleft patients.
Maxillary advancement in CLP most commonly requires a Le Fort I osteotomy. These have been be-devilled by the problems of instability and relapse and occasionally by loss of segments. These problems can be avoided by ensuring that the maxilla is always in one piece and that any alveolar cleft defect has been successfully bone grafted previously. The avoidance of ‘multipiece’ procedures improves blood supply to the maxilla and enables the radical breakdown of scar tissue from the cleft palate repair, which is the principal factor in relapse.
An incision, which starts and finishes just anterior and superior to each parotid duct opening and crosses the upper labial fraenum (Figure 5), provides a broad posterior pedicle and enhanced blood supply. The osteotomy cuts are made with an angled oscillating saw blade just below the infra-orbital foramina and are completed with fine osteotomes and nasal chisels with the pterygo-maxillary disjunction made with a curved chisel. Mobilization is at first made digitally and then with the use of Rowe's disimpaction forceps and Tessier mobilizers. With the maxilla displaced downwards, the posterior scar tissue can be palpated with a finger and separated from the posterior maxilla with the finger or with blunt scissors dissection. With this approach, advancements up to 2.5 cm can be achieved (Figure 10). The maxilla is then fixed to the mandible across the prepared acrylic wafer (IMF) with orthodontic chain elastic.23 The desired vertical position is achieved, if necessary, by bone removal in contact areas and the maxilla fixed with 4 x 2 mm titanium mini-plates and screws. Two blocks of autogenous corticocancellous bone, harvested from the medial anterior iliac crest, are placed over the bone steps anteriorly (between the mini-plates on each side) to ensure better bony union. The IMF is then removed and the wounds closed with a continuous resorbable suture. Intravenous antibiotics and steroids are routinely used during, and in the 1–2 days after, surgery to prevent infection and reduce swelling. They are invariably very effective.
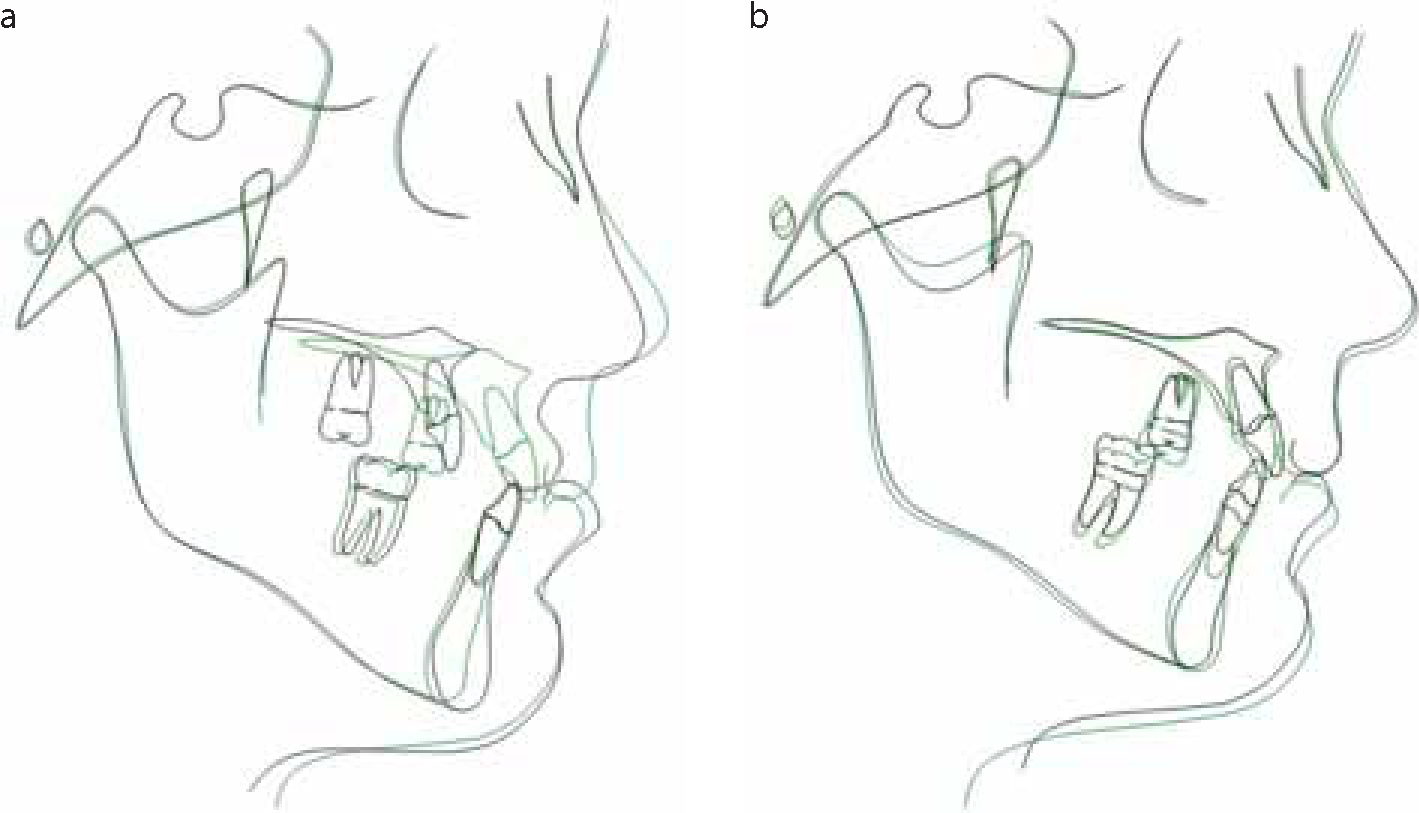
Figure 10.
(a) Pre- and post-operative tracings demonstrating >20 mm maxillary advancement (+ genioplasty). (b) Immediately post-op and 1 year post-operative tracings following >20 mm maxillary advancement (+ genioplasty).
Le Fort II osteotomy
Occasionally, it is necessary to advance the nose en bloc with the maxilla in cleft patients when there is genuine naso-maxillary hypoplasia present (Figure 11). In such cases, the technique described by Henderson and Jackson is used,24 but we always use a ‘coronal and oral’ approach, thus avoiding any scars on the face, with internal fixation using mini-plates and autogenous bone grafting from the anterior iliac crest in gap areas.
Figure 11. Le Fort II CLP maxillary advancement.
Distraction osteogenesis
Sometimes the maxilla in cleft patients needs to be advanced particularly large distances. Where this is the case, there has been a tendency among surgeons to perform this through gradual maxillary or midface advancement using either internal or external distraction osteogenesis (DO).
Our approach using internal DO has been to plan in 2D and 3D, as described above, and to adapt the distractors to a cut-down 3D stereolithographic model (Figure 9) to check the right positioning to achieve the right vector. A cutting and drilling guide (Figure 9) is made in stainless steel using Selective Laser Melting (SLM) and the maxilla downfractured with limited mobilization and the distractors placed on the mid-face in exactly the planned position to achieve the correct vector of distraction. After a few days of latency, the distraction is carried out bilaterally at 1 mm per day until a little more than the planned advancement and occlusion is achieved. Consolidation for a minimum of 8 weeks is followed by removal of the distractors at surgery.
It has been claimed that such an approach makes it easier to achieve the advancement, to do large advancements safely, to avoid bone grafting, to avoid speech sequelae and to avoid relapse. The evidence in support of these claims is weak. Research within this unit has not demonstrated that better speech results are achieved following DO maxillary advancement when compared to conventional osteotomy. Using either technique, it has not been difficult to advance the maxilla or midface safely up to 2.5 cm and there has been little demonstrable difference in the stability of the surgical outcome.
Post orthognathic care
Following the surgical intervention, fixed appliance therapy continues to complete the achievement of inter-arch objectives and support the surgical movements. This invariably involves the use of inter-arch mechanics to eliminate any posterior open bite prescribed by the final wafer and work against any surgical relapse tendency through Class III mechanics.
Throughout this period, it is important that patients receive psychological support and that potential psychological issues are identified and addressed. Issues which should be considered include coping with the recovery process, adjustment to change in appearance, coping with the reactions, comments and questions of others and satisfaction with outcome. Further intervention may be required to consolidate the benefits of surgery or to address disappointment, for example if expectations in terms of changes to appearance, as well as other psychological factors such as confidence, are not met. It may also be necessary to offer further input in relation to medical or psychological complications, such as low mood and to facilitate further decision-making about surgery/treatment, as required.