Epker BN, Fish LC. Surgical-orthodontic correction of open bite deformity. Am J Orthod. 1977; 71:278-299
Proffit WR, Bailey LJ, Phillips C, Turvey TA. Long-term stability of surgical open bite correction by Le Fort 1 osteotomy. Angle Orthod. 2000; 70:112-117
Umemori M, Sugawara J, Mitani H, Nagasaka H, Kawamura H. Skeletal anchorage system for open-bite correction. Am J Orthod Dentofacial Orthop. 1999; 115:166-174
Sugawara J, Baik UB, Umemori M, Takahashi I, Nagasaka H, Kawamura H Treatment and posttreatment dentoalveolar changes following intrusion of mandibular molars with application of a skeletal anchorage system (SAS) for open bite correction. Int J Adult Orthod Orthognath Surg. 2002; 17:243-253
Kuroda S, Sakai Y, Tamamura N, Deguchi T, Takano-Yamamoto T. Treatment of severe anterior open bite with skeletal anchorage in adults: comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2007; 132:599-605
Anterior open bites are notoriously difficult to correct. A case is described where a 26-year-old Caucasian female with an anterior open bite, due to a previous persistent digit-sucking habit, is treated successfully with upper and lower fixed appliances and skeletal anchorage to intrude the posterior teeth. This remained stable one year post treatment.
Clinical Relevance: Clinicians should be aware that the posterior teeth in patients with mild to moderate anterior open bites can be intruded successfully with temporary anchorage devices.
Article
Anterior open bites are a difficult problem to correct. The aetiology is complex and involves a combination of skeletal, dental, functional and habitual factors. A variety of treatment modalities have been used to treat patients with anterior open bites, including orthodontic extrusion of the anterior teeth or a combination of orthodontic and orthognathic surgical treatments in adults.1 These surgical procedures are relatively stable and produce acceptable results.2
The use of skeletal anchorage to correct anterior open bites with orthodontic intrusion of posterior teeth has been reported in patients with mild to moderate anterior open bites.3,4
A case is described where a 26-year-old Caucasian female with an anterior open bite is treated successfully with upper and lower fixed appliances and skeletal anchorage.
Case report
A 26-year-old Caucasian female was referred by her general dental practitioner with an increased overjet and an anterior open bite. She had been a persistent digit sucker until 18 months previously.
The patient had a mild skeletal II pattern base with average vertical proportions. Her lips were competent at rest. The nasolabial angle was within the normal range and the lower lip was behind Rickett's E-line. There was no incisor show at rest. There were no signs of temporomandibular joint dysfunction.
The oral hygiene was fair with marginal gingivitis affecting the lower labial segment. She had a full complement of permanent teeth apart from the upper third molars. All four first molars and the lower right second molar showed evidence of caries.
The upper and lower arches were well aligned with mild spacing in the upper labial segment. The upper incisors were proclined and the lower incisors were of average inclination. In occlusion, the overjet was 5 mm at the upper left central incisor and there was an anterior open bite of 4 mm extending back to the first premolar region. The upper and lower centrelines were correct and coincident with the facial midline. The canine relationship was a ¼ unit II bilaterally and the molar relationship was Class I bilaterally.
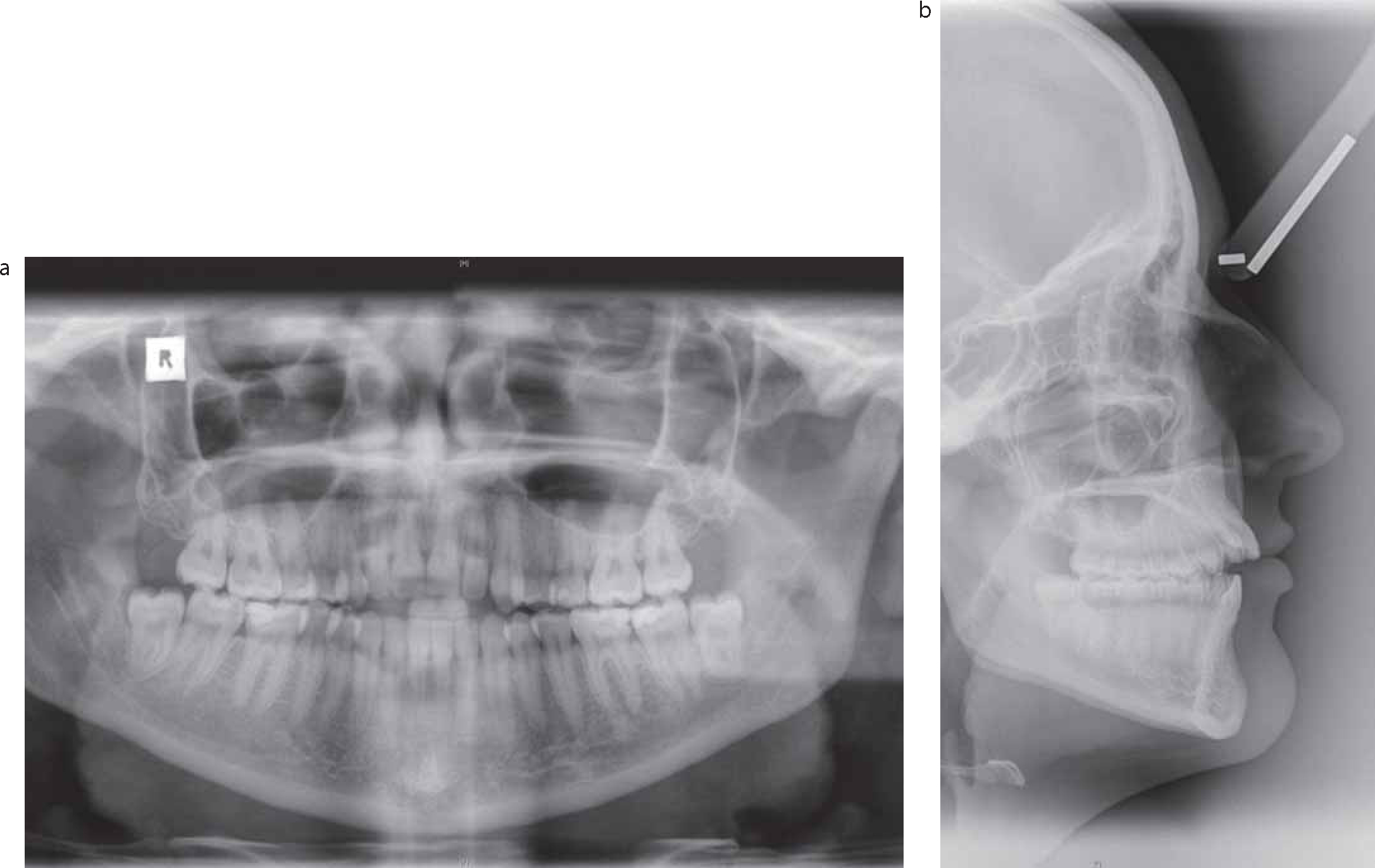
The panoramic radiograph confirmed the presence of all permanent teeth excluding the upper third molars. The alveolar bone levels were normal. There was evidence of caries in all four first molars and the lower right second molar.
Cephalometric analysis (Table 1) confirmed the clinical findings that the patient had a Skeletal I pattern with an ANB of 4°. The maxillary-mandibular plane angle was average at 27° with a lower face height proportion of 55%. The lower incisors were lying on the A-Pog line.
Variable
Pre-treatment
Average values
SNA (°)
82
81 +/- 3
SNB (°)
78
78 +/- 3
ANB (°)
4
3 +/- 2
Wits Appraisal (mm)
3
1 +/-
Upper incisor to maxillary plane (°)
119
109 +/- 6
Lower incisor to mandibular plane (°)
89
93 +/- 6
Inter incisor angle (°)
125
135 +/- 10
Maxillary mandibular planes angle (°)
27
27 +/- 4
Lower anterior face height (%)
55
55 +/- 2
Lower incisor to A-Pog (mm)
0
1 +/-2
Aetiology
The malocclusion was dental in origin where the digit-sucking habit had resulted in an anterior open bite.
Aims of treatment
Improve oral hygiene;
Control of caries;
Align and level the arches;
Improve the overbite;
Sagittal correction of the malocclusion with overjet reduction, whilst maintaining the molar relationship;
Detail the static and functional occlusion;
Retain the corrected occlusion.
Two treatment approaches were discussed with the patient:
Combined orthodontic and orthognathic approach;
Orthodontic treatment only, using Temporary Anchorage Devices (TADs) to intrude the buccal segments.
The patient opted for option 2 to start with but was made aware that, if this approach was not successful, option 1 was still available.
Treatment plan
Dental health education;
GDP to investigate the caries and restore as necessary;
Upper and lower pre-adjusted edgewise appliance treatment (0.022 x 0.028 inch slot, MBT prescription) on a non-extraction basis;
Upper and lower vacuum-formed retainers.
Rationale for treatment plan
Skeletal anchorage to intrude the upper buccal segments was the preferred choice in this case as the aetiology of the open bite was due to a habit as opposed to skeletal factors. This approach is less invasive than surgical correction and also avoids the nasal and sensory side-effects of surgery.5 It is also significantly cheaper than a surgical approach. If this approach was not successful there was nothing to preclude the patient from being treated with combined orthodontic and orthognathic treatment.
Consent. Record collection. Placement of separating elastics.
2
Upper and lower pre-adjusted edgewise (MBT prescription 0.022 x 0.028” slot) fitted. All teeth included except for the second molars. Upper and lower 0.016” NiTi archwires placed.
3
Upper 0.018” SS. Retie lower 0.016” NiTi. Power chain placed between the upper canines.
4
Upper 0.018 x 0.025” NiTi placed. Lower 0.018” SS.
5
A removable transpalatal arch was constructed 4 mm space between palatal tissues and the appliance and cemented with glass ionomer cement. The upper second molars were included and a new upper 0.018 x 0.025” NiTi archwire was placed.
6
8 months into treatment following alignment of the arches.10 mm long, 2 mm diameter, Vector TAD placed palatal to upper right second premolar and first molar. 8 mm long, 1.4 mm diameter, Vector TAD placed palatal to upper left second premolar and first molar. No initial activation of TADs.
7
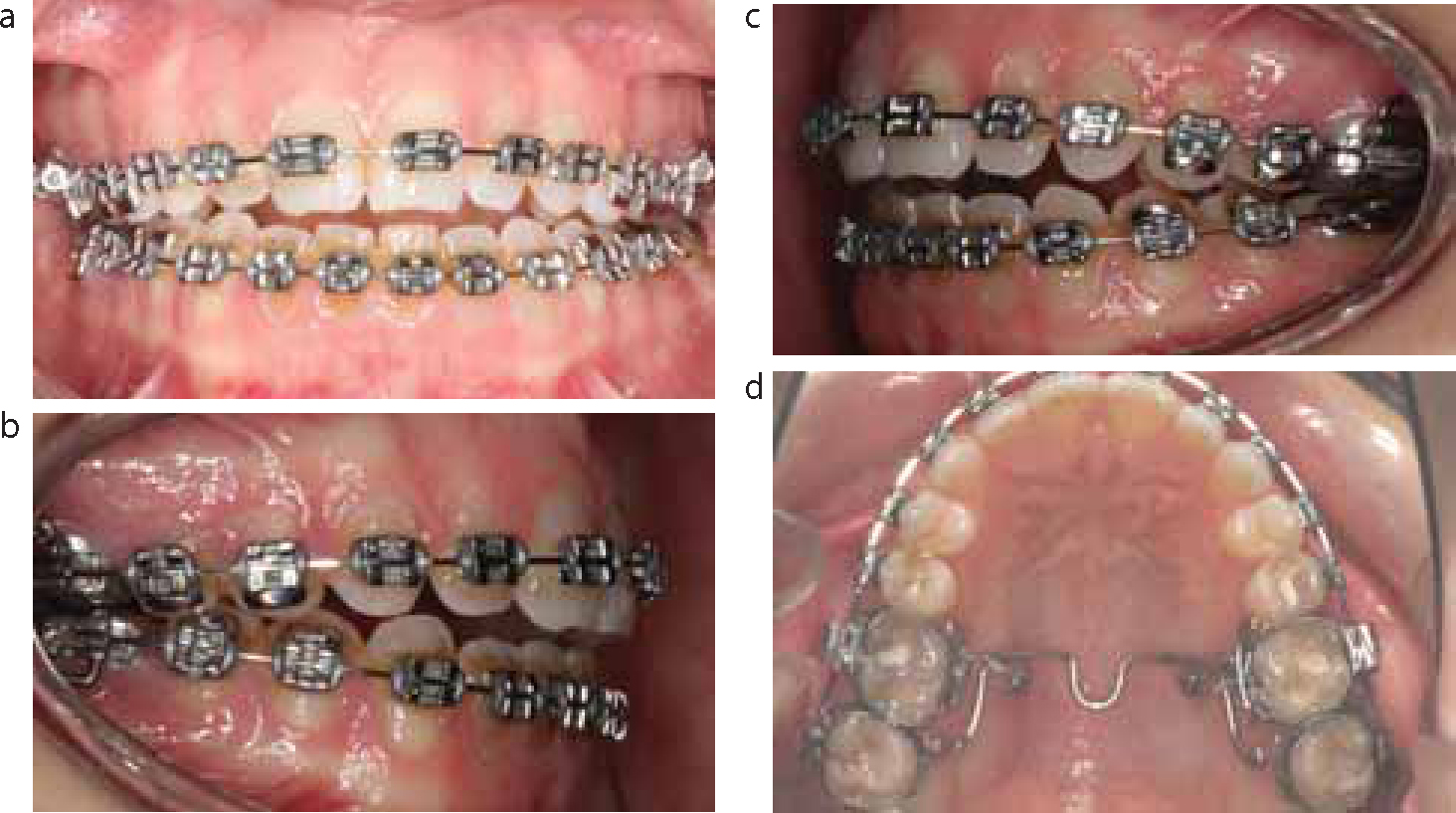
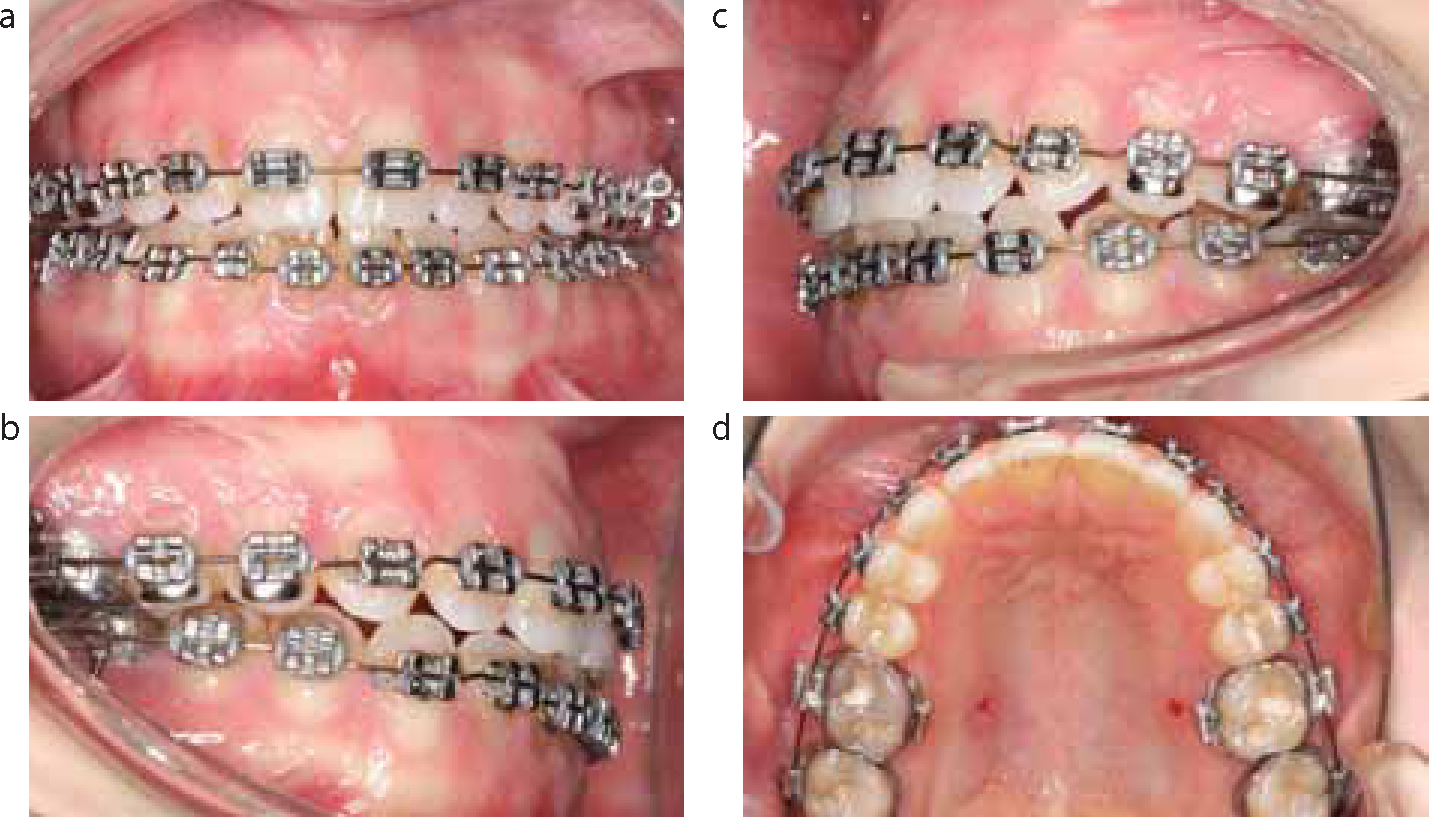
Upper 0.019 x 0.025” SS. Zing string traction from TADs to TPA (Figure 3 a–d).
8 & 9
Zing string refreshed and archwire retied.
10
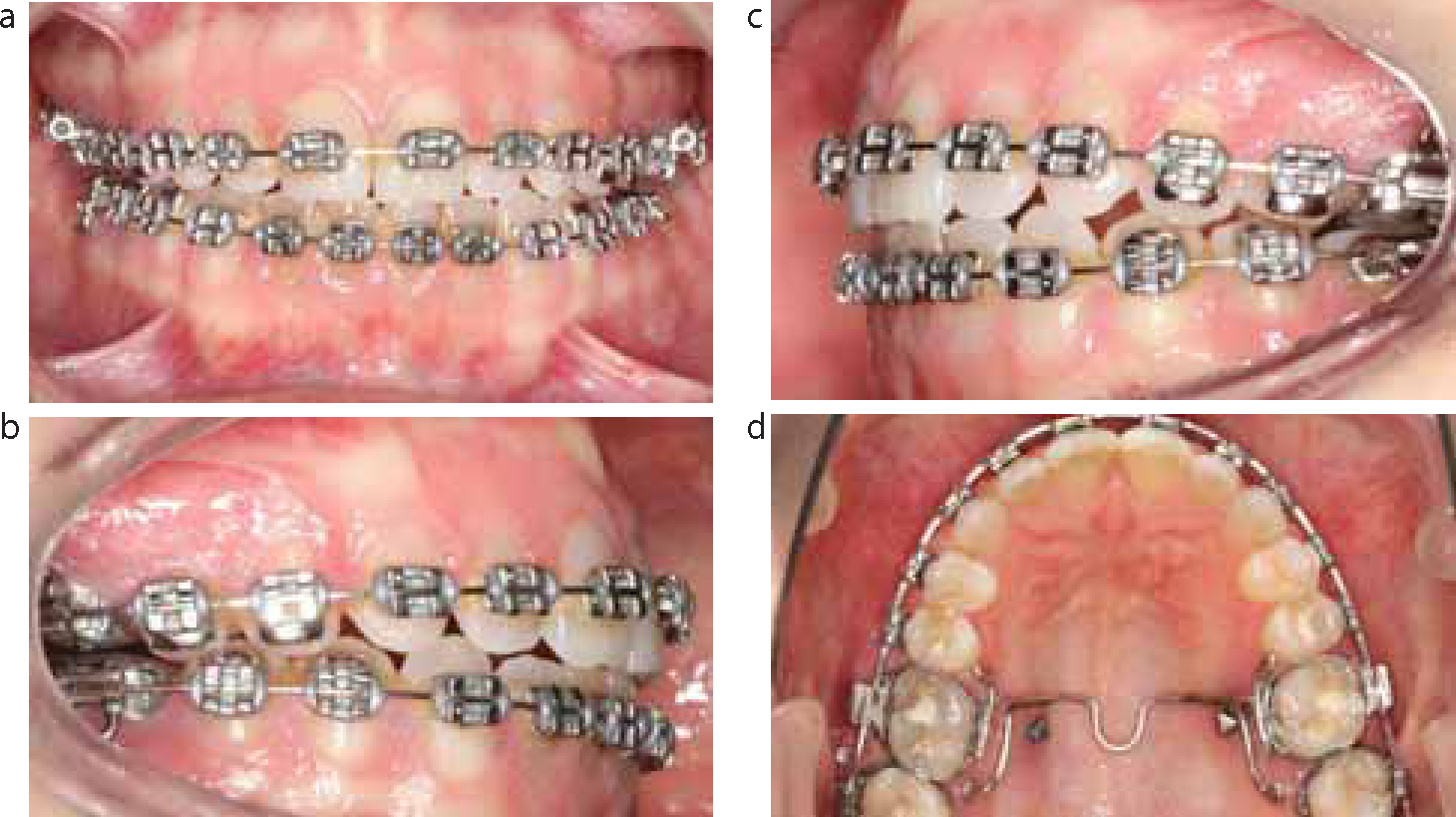
Upper left TAD mobile. AOB reduced. No zing string activation (Figure 4 a–d). 0.019” x 0.025” SS upper archwire placed, lower arch retied.
11
AOB monitored. Archwires retied.
12
Emergency appointment: Cleat from palatal aspect of molar band loose, therefore TPA removed.
13
TADs removed with no local anaesthesia. Upper and lower 0.016” SS archwires, with finishing bends to extrude upper canines, intrude the lower right canine and extrude the lower right lateral incisor (Figure 5 a–d).
14
Debond. Upper and lower vacuum-formed retainers fitted (Figure 6 a–h).
Figure 3.
(a–d) Treatment at 10 months: first intrusive force applied.Figure 4.
(a–d) Treatment at 15 months: de-activation of TADs.Figure 5.
(a–d) Treatment at 20 months: finishing wires placed.Figure 6.
(a–h) Appliance removal at 22 months.Figure 7.
(a–h) Following 12 months of retention.
Active treatment was initiated once the oral hygiene had improved and the caries was controlled. Upper and lower fixed appliances were fitted on all teeth except for the second molars. Upper and lower 0.016” Nickel Titanium (NiTi) archwires were placed.
Five months later, bands were selected for the maxillary first molars and a custom made, removable trans-palatal arch (TPA), which was constructed so that there was a 4 mm space between the palatal tissues and the TPA. This was then cemented with glass ionomer cement. The upper second molars were included and an upper 0.018 x 0.025” NiTi archwire placed.
Eight months into treatment following aligning the arches, two temporary anchorage devices (TADs) were placed in the palate under local anaesthesia as outlined below:
10 mm long, 2 mm diameter, Vector TAD placed palatal to upper right second premolar and first molar.
8 mm long, 1.4 mm diameter, Vector TAD placed palatal to upper left second premolar and first molar.
No activation was placed to the TADs at this stage.
At the following visit an upper 0.019 x 0.025” stainless steel (SS) and lower 0.018” SS archwire were placed and zing string was used to place an intrusive force on the upper molars (Figure 3 a–d). Zing string was refreshed at two successive visits at six-weekly intervals.
The TAD in the upper left side of the palate was slightly mobile 7 months after the TADs had been placed. All attachments to the TADs were removed and there was no more intrusive force on the upper posterior teeth (Figure 4 a–d). The upper and lower archwires were retied.
The overbite was monitored for several visits and the archwires checked. Five months post de-activation of the TADs there was minimal relapse of the anterior open bite and the TADs and TPA were removed. The occlusion was detailed with upper and lower 0.016” SS archwires with finishing bends to extrude the upper canines, intrude the lower right canine and extrude the lower right lateral incisor (Figure 5 a–d). A near end of treatment radiograph was not taken as the patient announced she was pregnant and did not consent to having any further radiographs.
The appliances were removed 11 months following active intrusion of the upper molars and the patient was fitted with upper and lower removable vacuum-formed retainers (Figure 6 a–h). The patient has been reviewed at 3 months and 12 months following appliance removal and there has been no more relapse in the anterior open bite. The patient remains incredibly pleased with her occlusion (Figures 7 a–h). The treatment time was 22 months.
Discussion
The authors would like to note that, with increased use of TADs within the department, confidence has grown and it is now routine practice to load the TADs on insertion.
This case has shown a technique to treat an adult with a 4 mm anterior open bite successfully without recourse to orthognathic surgery, which would be the routine method for correction of this type of malocclusion. This treatment remains stable one year following appliance removal.