Bender PL Genetics of cleft lip and palate. J Pediat Nurs. 2000; 15:242-249
Gregg TD, Boyd D, Richardson A The incidence of cleft lip and palate in Northern Ireland from 1980-1990. Br J Orthod. 1994; 21:387-392
Jensen BL, Kreiborg S, Dahl E, Fogh-Anderson P Cleft lip and palate in Denmark 1976-1981: epidemiology, variability and early somatic development. Cleft Palate J. 1988; 25:258-269
Amaratunga NA A study of etiologic factors for cleft lip and palate in Sri Lanka. J Oral Maxillofac Surg. 1989; 47:7-10
Hagberg C, Larson O, Milerad J Incidence of cleft lip and palate and risks of additional malformations. Cleft Palate Craniofac J. 1998; 35:40-45
London: HMSO; 1998
Milerad J, Larson O, Hagberg C, Ideberg M Associated malformations in infants with cleft lip and palate: a prospective population-based study. Pediatrics. 1997; 100:180-186
Stoll C, Alembik Y, Dott B, Roth MP Associated malformations in cases with oral clefts. Cleft Palate Craniofac J. 2000; 37:41-47
Lees M Genetics of cleft lip and palate. In: Watson ACH London: Whurr Publishers; 2001
Mars M, Houston WJB A preliminary study of facial growth and morphology in unoperated male unilateral cleft lip and palate subjects over 13 years of age. Cleft Palate J. 1990; 27:7-10
Shaw WC, McWilliam J, Sell D, Murphy T, Mildinhall S, Bearn D A six-center international study of treatment outcome in patients with clefts of the lip and palate. Parts 1-5. Cleft Palate Craniofac J. 1992; 29:393-418
Bearn D, Mildinhall S, Murphy T, Murray JJ, Sell D, Shaw WC Cleft lip and palate care in the United Kingdom - the Clinical Standards Advisory Group (CSAG) study: Part 4. Outcome comparisons, training and conclusions. Cleft Palate Craniofac J. 2001; 38:38-43
Fitzsimons KSD, van der Meulen J, Copley L CRANE Database: Annual Report 2011. 2011;
This paper provides an overview of the historical background to the delivery of care in the UK of patients with cleft lip and palate and the impact of the Clinical Standards Advisory Group (CSAG) report. The paper explains the way cleft services have subsequently changed and describes the current delivery of care following CSAG recommendations within the multidisciplinary team. Following this introductory paper will be a series of papers dedicated to describing and explaining the different roles of each specialist member of the cleft team and key stages of delivery of care within that team.
Clinical Relevance: Introduction and background into the delivery of care of cleft services in the UK. This is an introductory paper of a series of papers intended to increase the depth and breadth of knowledge of the reader into the specialist areas required in the multidisciplinary approach for the care of patients with cleft lip and/or palate.
Article
The management of patients with cleft lip and palate is both challenging and highly rewarding. The care of this patient group, from the antenatal diagnosis, continues until late adulthood. Close co-ordination between the many specialist areas involved is essential to provide the highest quality of care for the patient.
The prevalence of cleft lip and palate in non-syndromic children is quoted as 1 in 700 live births.1 Cleft lip with cleft palate is the most common presentation in England and Wales, however, cleft lip does vary in prevalence, not only within but also between different racial groups. Males are more commonly affected than females and are more likely to have complete clefts. Unilateral clefts have been found to be most common on the left-hand side.2
Few prevalence studies discriminate between unilateral CLP and bilateral CLP, although a prevalence ratio of 4:1 has been reported.3 The aetiology of cleft lip and palate is still largely unknown, although it is suggested to be epigenetic where several genetic and environmental factors interfere with the morphogenesis resulting in clefting.4
Unfortunately, patients with cleft lip and palate are associated with lower birth weight5 and increased mortality rates compared with non-cleft populations.6 They also often (21–37%) have other associated health anomalies. The most common of these are cardiovascular, musculo-skeletal, facial dysmorphia and genito-urinary challenges.7,8 Currently, there are over 400 syndromes associated with patients with oral-clefting.9
It is the intention of this series of articles to outline the main topics and specialty areas in the provision of care for patients with cleft lip and palate. They will be published as each specialty/topic affects the patient chronologically.
The areas that will be covered are:
Outreach nursing;
Primary lip and palate repair;
Paediatric dentistry;
Speech and language therapy;
Psychology;
Alveolar bone grafting;
Secondary surgery and distraction osteogenesis;
Orthodontic management;
Restorative dentistry;
ENT;
Speech prosthesis.
Each article will deal with a dedicated area describing modern approaches to treatment within that area. It is hoped that these papers will not only enlighten the reader as to the holistic care required for cleft patients, but also give an insight into the workings of the multidisciplinary care required from a cleft team.
This is a group of individuals from different specialties who work within agreed and dedicated care pathways. They work in a seamless way to bring their particular skill sets and expertise to the patient, whilst working in a co-ordinated way with other members of the cleft team.
The care pathway begins at the antenatal stage and continues to adulthood. The patient will undergo a number of in-patient treatment episodes. These procedures will often involve a combination of several members of the team and the team structure allows this to be completed in a co-ordinated manner. In other instances, often in an out-patient setting, for example speech and language therapy, ENT and psychology, treatment is provided in separate environments.
Clinical Standards Advisory Group (CSAG)
There has been a significant change in the delivery of care for patients with cleft lip and palate in the United Kingdom in the last 10 years. This has been largely due to the findings of a Clinical Government report from the Clinical Standards Advisory Group (CSAG report).6 These changes have galvanized the co-ordination of the multidisciplinary care of a cleft team.
Changes to the delivery of cleft care in the United Kingdom were instigated because of concerns raised over the quality of treatment of patients with cleft lip and palate within the United Kingdom.10,11 When children within the UK were compared to children of comparable age within Europe, they were found to have more mid-face retrusion, suggestive of poor growth, and significantly worse bone graft outcomes.11
In 1995, the Department of Health commissioned the CSAG to carry out a report into the quality of care for children with cleft lip and palate within the UK.6 The report included all children aged 5 to 12 years of age in 1996/1997 with complete unilateral cleft lip and palate. Several conditions were examined including:
Dental malocclusion;
Dental health;
Quality of alveolar bone graft outcome; and
Skeletal base relationships.
The report provided some disappointing results. Most centres were found to be poor for reporting the outcomes of treatment and monitoring progress.12
In general, units had a low volume of cleft surgical operators and, although the evidence was equivocal that those with a high volume of operators resulted in a better outcome, a decision was made to centralize cleft care. This would at least verify the quality of outcome by concentrating care specialists and also allow a full range of facilities and experience for complete and comprehensive cleft care to be located centrally.
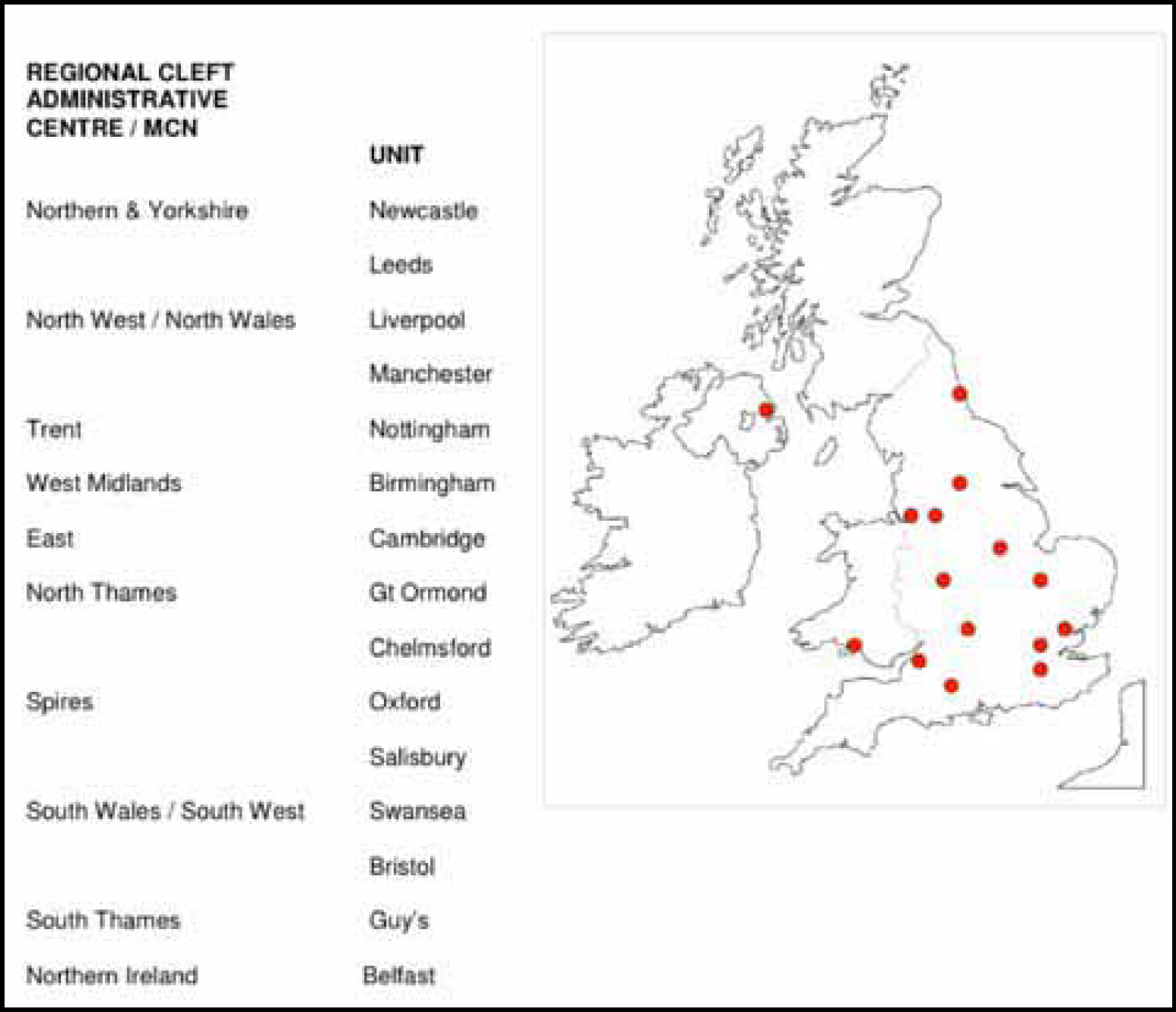
To date, there are ten such designated cleft centres in existence (Figure 1). In Scotland the new service took the form of a managed clinical network (MCN), the first in Scotland, known as CLEFTSiS.
Figure 1. Regional cleft units in the England, Wales and Northern Ireland post CSAG. Reproduced with permission from CRANE database.13
The Clinical Standards Advisory Group (CSAG) made several recommendations:6
Expertise and delivery of care should be limited to a restricted number of centres: 6 to 15 centres.
Within each centre, there must be a full range of cleft care.
The quality of record-keeping must be improved, as well as the development and implementation of a National Database.
All treatments have to be audited on a regular basis so as to allow comparison between different centres.
The future training and development of specialties required for the delivery of care of cleft patients must be focused within these centres, and restricted only to units that have a high volume of patients.
The team members within each unit comprise:
A specialist cleft surgeon, in both primary and secondary surgery;
A specialist orthodontist;
A specialist speech and language therapist;
Geneticists;
A paediatrician;
An ENT specialist; and
A psychologist.
As specified in the CSAG report, it is critical that systems and support staff are in place to facilitate and be responsible for data collection and auditing outcomes. The care is delivered through dedicated care pathways, which are based on the best evidence available.
In reality, owing to geographical and demographic challenges within each regional centre, there will always be minor variations in the care pathways from one centre to the next. However, because of structured protocols adhered to by units, meaningful audits can be carried out between units.
CRANE database
From the recommendations of the CSAG report,6 it was suggested that the reporting of outcomes for cleft care in the UK was inferior to that of other Western European countries. For this reason, a National Database was developed and implemented.
Prior to CSAG there was a Craniofacial Anomalies Register (CARE), which was established in 1990 and was maintained by the Craniofacial Society for Great Britain and Ireland (CFSGBI). CRANE was a natural development of this database. Currently, the CRANE database collects information about children born with cleft lip and/or palate in England, Wales and Northern Ireland. In Scotland, CLEFTSiS maintains its own separate database. The funding for CRANE is supplied centrally from the Specialist Commissioners. The Cleft Development Group (CDG) is responsible for making the arrangements for the running and commissioning of the CRANE database.
CRANE currently records the births of cleft children, the treatment that they have received, as well as selected agreed outcomes, all of which facilitates a National Audit. With the recording of births, this will ensure an up-to-date register of cleft children, as well as the frequency and incidence within the population. The auditing and reporting on the quality of care of patients with clefts will promote higher standards in clinical management for these patients.13
Cleft Care UK (CSAG II)
A similar piece of work to the first CSAG report is currently being undertaken within the UK, assessing 5-year-old children with complete unilateral cleft lip and palate (born 2005–2006). All aspects, with the exception of the quality of the alveolar bone grafts, are being re-assessed, with the addition of the dental health and psychological outcome indicators. The findings will hopefully be available in the very near future and will be keenly awaited to see if all the recommendations have borne the fruit of improving our patients' care.