Goudy S, Lott D, Canady J, Smith RJH. Conductive hearing loss and otopathology in cleft palate patients. Otolaryngol Head Neck Surg. 2006; 134:(6)946-948
Bixler EO, Vgontzas AN, Lin HM, Liao D, Calhoun S, Fedok F Blood pressure associated with sleep-disordered breathing in a population sample of children. Hypertension. 2008; 52:(5)841-846
Role of the ear nose and throat specialist within the multidisciplinary cleft team: CLP series part 11 David M Wynne Toby J Gillgrass Orthodontic Update 2025 7:3, 78-81.
Authors
David MWynne
MB, ChB, MRCS(Glasg), FRCS (ORL-HNS)
Royal Hospital for Sick Children, Yorkhill, Glasgow, UK
A cleft involving the palate can have a significant impact on children in relation to their hearing and airway. A normally functioning ear is important for hearing and therefore speech production. Airway difficulties in children with a cleft may be divided into neonatal, post-operative and long-term and may necessitate both acute and long-term management. As a consequence the Ear Nose and Throat specialist plays an important role within the cleft multidisciplinary team.
Clinical Relevance: Hearing problems in children and adults with a cleft may lead to difficulties in communication between patient and dental practitioner. The patients may also be undergoing long-term airway-related management that may impact on their regular attendance.
Article
In relation to the Ear Nose and Throat specialist, the impact of a cleft of the palate, with or without involvement of the lip, may be divided into those issues relating to:
Hearing; and
Airway.
Hearing
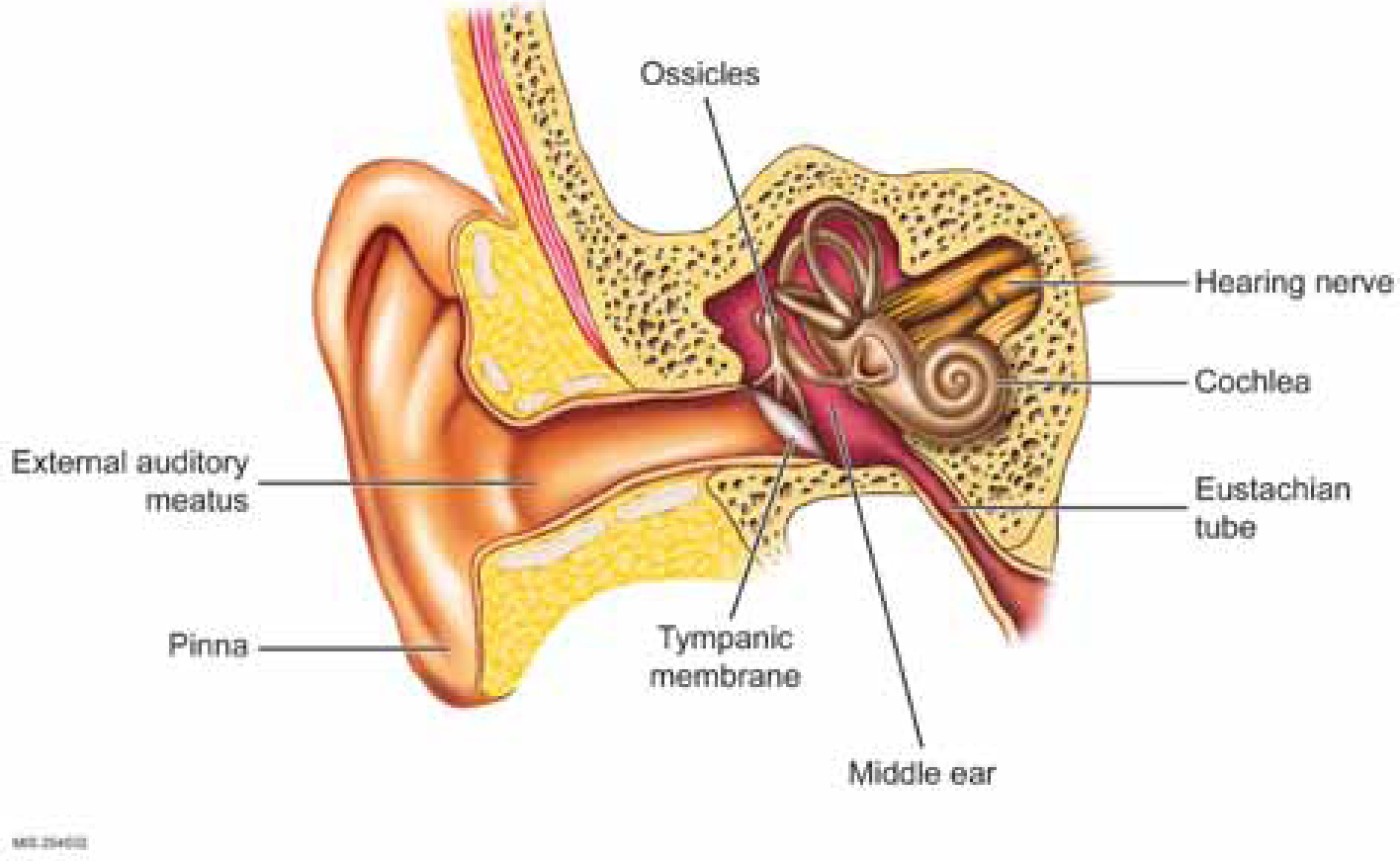
A normal functioning ear apparatus is essential for hearing and ultimately speech development. When a noise is created it sends a sound wave that causes vibration of the tympanic membrane. This vibration continues through the middle ear cavity via the ossicles to the cochlear. Vibration within the cochlear causes cilia to move and these movements change mechanical energy into electrical signals. These signals are transmitted to the brain through the auditory nerve (Figure 1).
Figure 1. Diagrammatic representation of the ear showing external, middle and inner ear.
Normally, the middle ear is air-filled. The eustation tubes are usually closed but are opened by the palatal musculature on swallowing, allowing air to enter; if the eustation tube is not functioning then it can become fluid-filled or the abnormal pressure can cause the tympanic membrane to retract. In cleft palate children, the abnormal development of the palatal musculature and its insertion on the eustation tube opening is thought to affect the ventilation of the middle ear. If this persists then this may cause fluid to persist, ie otitis media with effusion or ‘glue ear’. This fluid in the middle ear can attenuate sound transmission and result in a hearing loss.
Most children, cleft and non-cleft, will have an episode of ‘glue ear’ at some point in early infancy (Cleft Lip and Palate Association Information Leaflet).1 There is a prevalence peak of around 20% at approximately 2 years of age and another at about 6 years. In cleft palate children the incidence is thought to be higher, with some studies reporting up to 90% of children affected.2 The prevalence of ‘glue ear’ can be more chronic and lead to more significant otological sequelae in this group.3
Types of hearing loss
Where hearing loss is due to abnormalities or restrictions of the mobile portions of the ear apparatus (tympanic membrane, ossicles) that transmit the sound, it is known as conductive hearing loss. This is the commonest cause of hearing impairment in children with clefts.
Where there is impairment of the cochlear, auditory nerve or brain, it is known as a sensorineural hearing loss and, when associated with a cleft palate, may be part of a syndrome such as Sticklers, Crouzon, or Apert syndrome.
Hearing testing can be objective or subjective. The type of test chosen is dependant on the child's developmental age. Objective testing does not require an active response from the child; it instead picks up electronic signals produced by the auditory pathway or sounds emitted from the cochlea, for example an auditory brainstem response (ABR) or otoacoustic emissions (OAE). These are often used in hearing screening programmes of newborn babies. Subjective testing requires an active response from the child. This can range from head turning to noise (Figure 2) through to a visual reinforcement audiology to pressing a button when hearing a noise through headphones (Figure 3) (pure tone audiogram).
Figure 2. Example of a young child undergoing visual reinforcement audiology. Note his head turning as a reaction to the noise.Figure 3. Example of an older child performing pure tone audiology; he presses the button when he hears the sound.
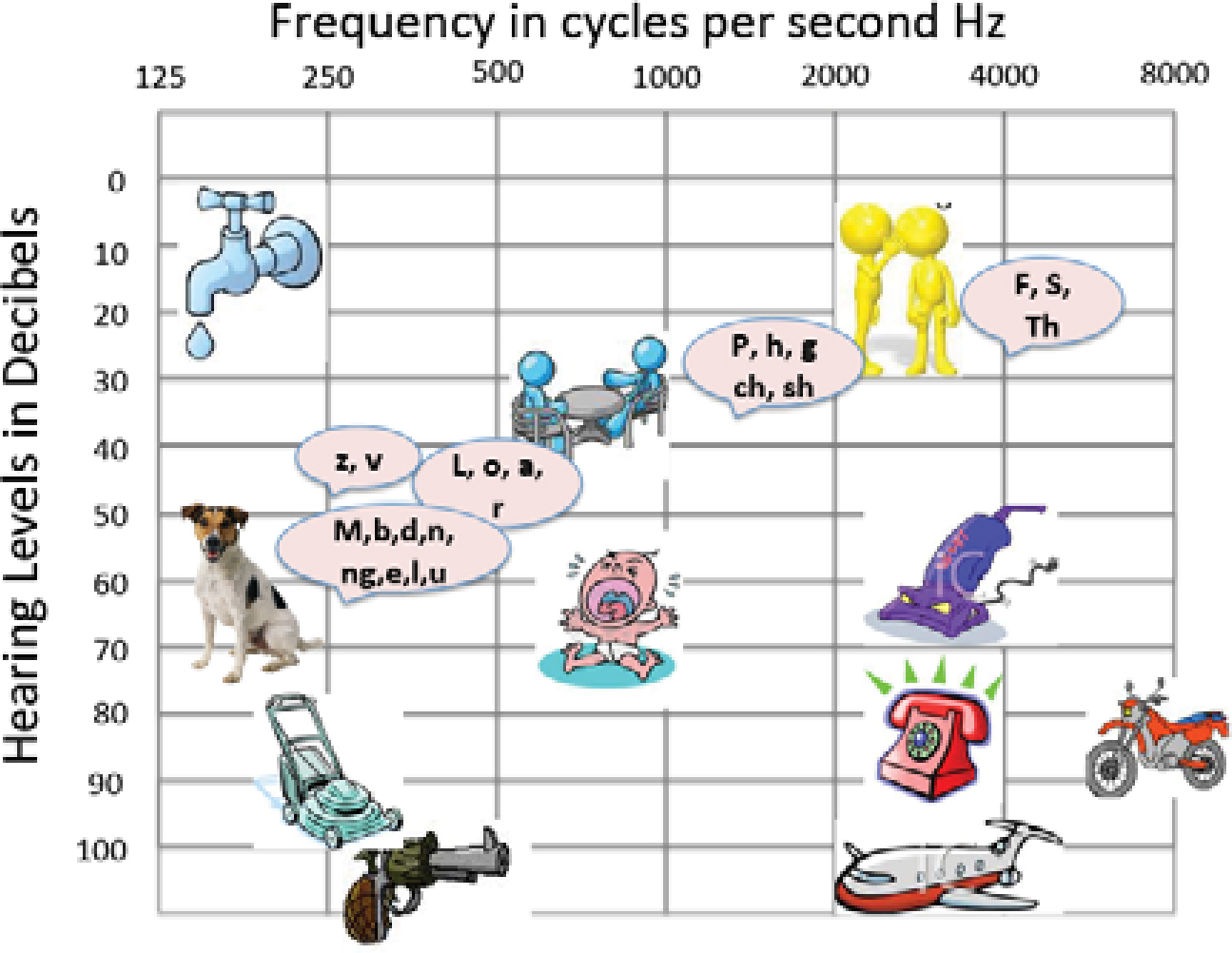
The hearing level is displayed on an audiogram that shows the softest tones detectable. Low frequency tones are to the left and high frequency tones to the right. Quiet tones to the top and loud to the bottom (Figures 4 and 5).
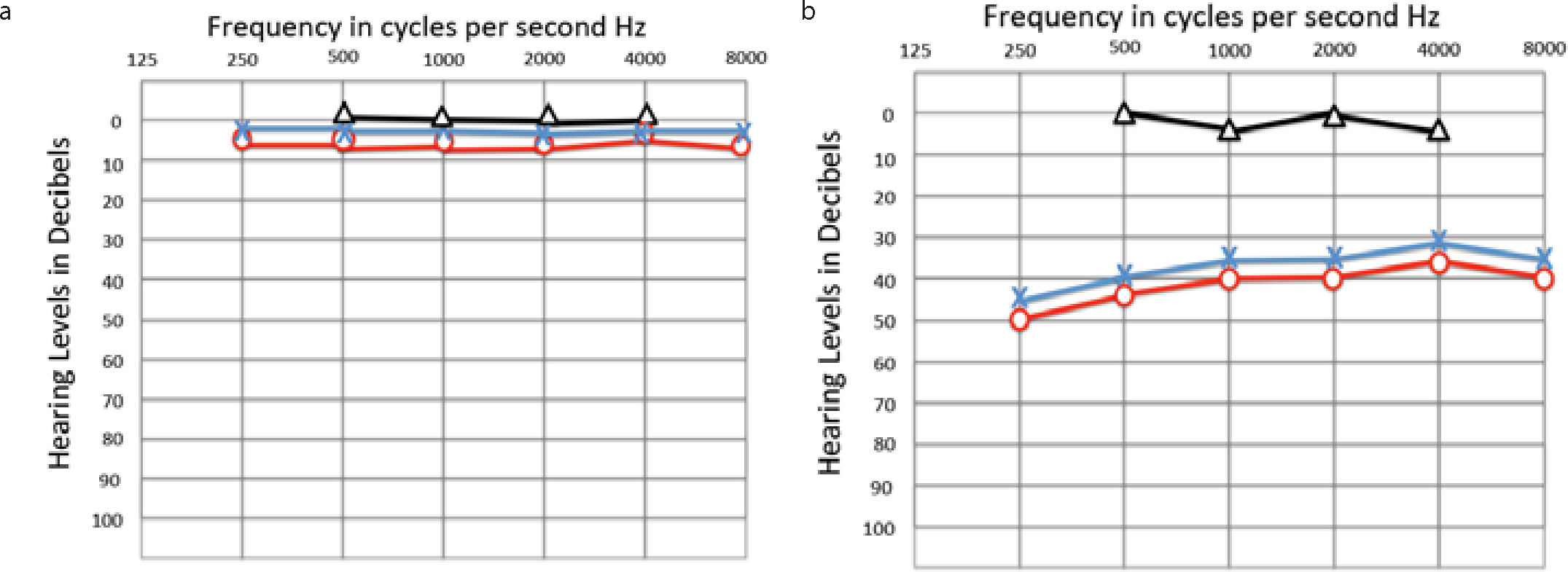
Figure 4. Audiogram with diagrammatic representation of the sounds heard at different areas of the audiogram.Figure 5.
(a) Example of an audiogram with normal hearing thresholds. (b) Example of an audiogram with a bilateral conductive hearing loss, eg ‘glue ear’. Black line: represents bone conduction threshold; Red line: represents right air conduction threshold; Blue line: represents left air conduction threshold.
Management of hearing loss
In the UK, cleft palate children undergo regular audiometric testing from an early age to ensure that they are not being handicapped by a hearing loss.
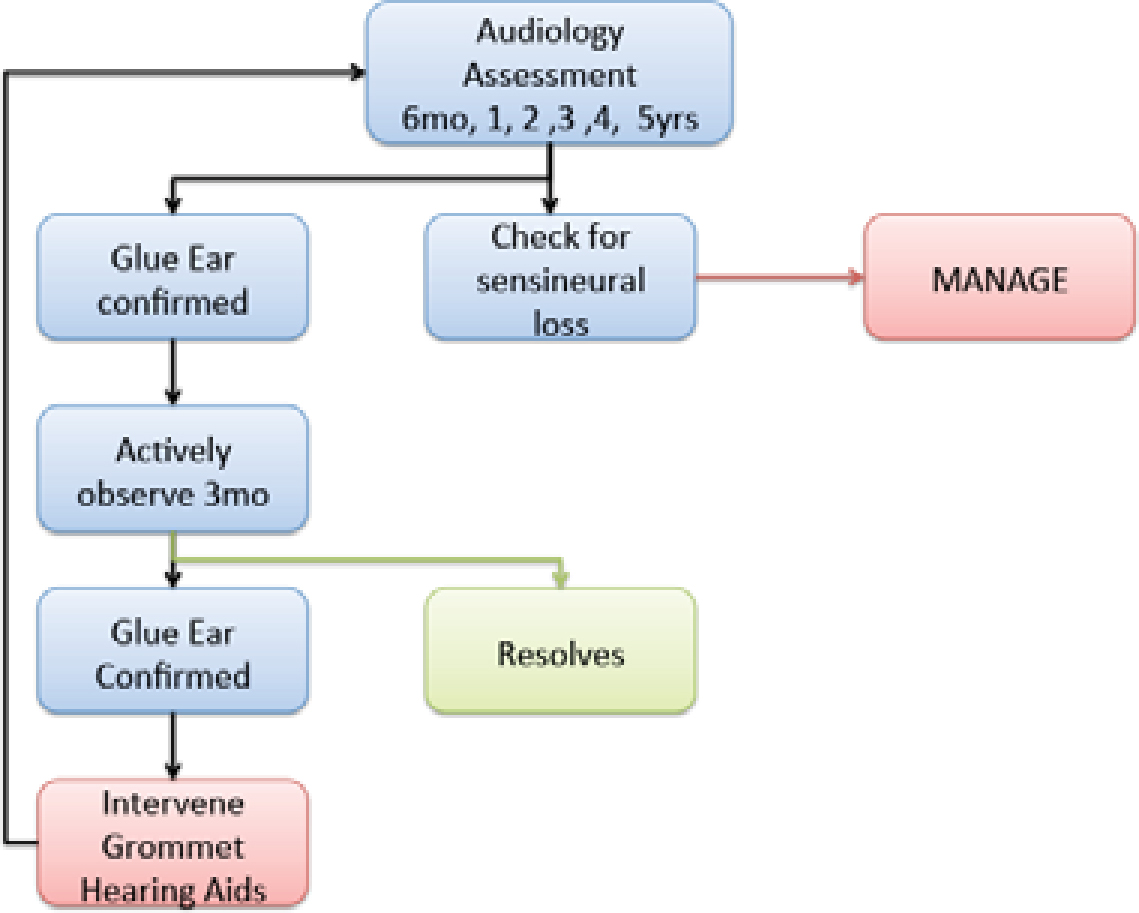
There is a treatment algorithm produced by NICE (NICE guideline)4 which recommends treatment/intervention when the child's hearing is below 25–30 dB. The treatment options would include:
Figure 6. Modification of NICE guidelines for treatment of hearing loss.
Treatment of hearing loss
Hearing tactics
This would include getting the child's attention before speaking, talking in good light and talking face to face. Schoolteachers should be informed and the child positioned closer to the front of the class.
Ventilation tubes (grommets)
These are small plastic tubes place in the eardrum to allow ventilation of the middle ear (Figure 7). These may be considered if there is a persistent hearing loss causing a handicap due to a middle ear effusion. Generally, these would only be considered after a period of observation for three months. Complications may include perforation and ear discharge.
Figure 7. Example of a ventilation tube in a tympanic membrane.
Hearing aids
The two main types of hearing aids used in cleft palate children are bone conduction hearing aids and air conduction hearing aids. Bone conduction aids vibrate the skull and the cochlea directly. Air conduction aids amplify the sound being transmitted to the tympanic membrane, which is then conducted through the middle ear structures to the cochlea.
Airway problems
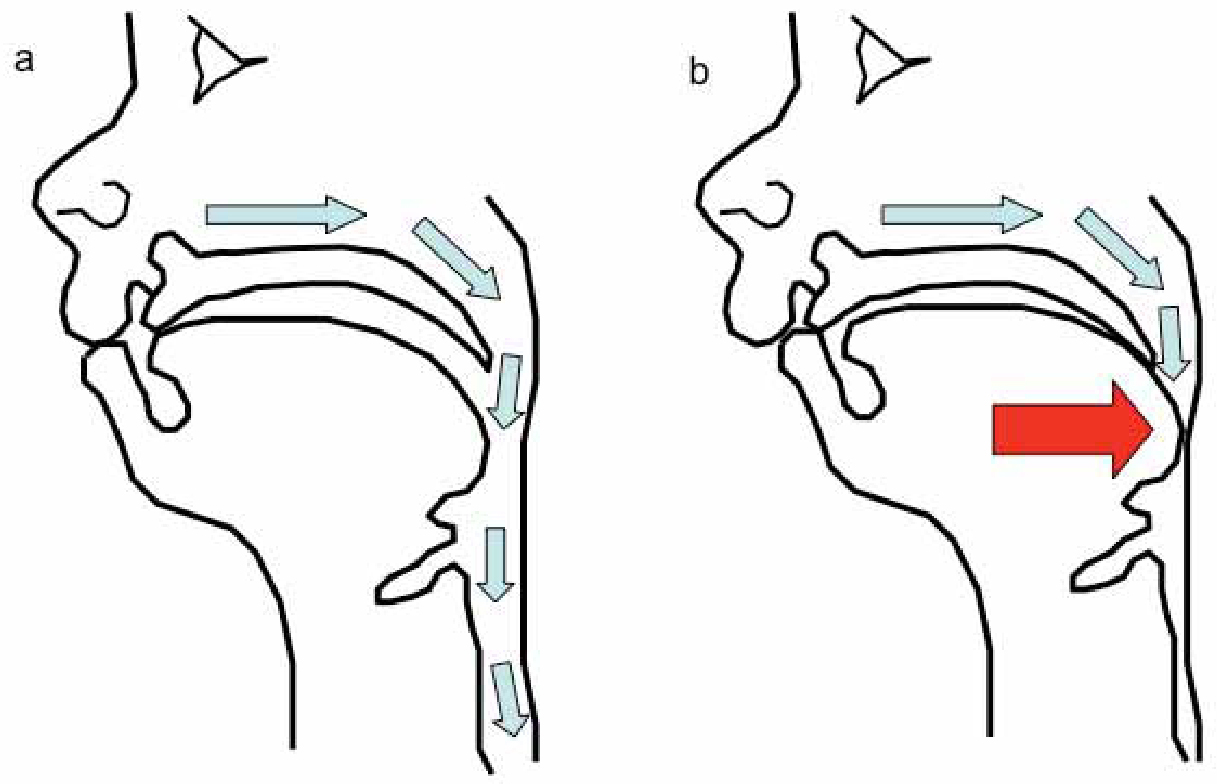
All children are obligate nasal breathers for the first few months of life. This is due to the high position of the infantile larynx that gradually descends. The larynx is high to allow the child to suckle. There are many congenital anomalies associated with cleft lip and plate. Some of these involve potential airway problems. The most common of these is Pierre Robin, where the small mandible results in a retro-position of the tongue which results in a blocked airway (Figure 8). Other anomalies include:
Figure 8. Diagram showing a normal airway (a) in an infant and (b) where retro-position of the mandible has resulted in the tongue blocking the airway.
Treacher Collins;
Goldenhar; and
22Q deletion syndrome.
Even without a clearly defined syndrome, children with a cleft are more prone to anaesthetic difficulties, including intra-operative airway and respiratory complications.
Airway problems in cleft children can be divided into three main periods.
Neonatal period
This can happen immediately following birth or can be progressive over the first few weeks or months of life. Snoring, apnoea during feeds or protracted feeding may indicate chronic obstruction. Definitive diagnosis is made by sleep studies, which may take place as part of inpatient care or using portable equipment at home.
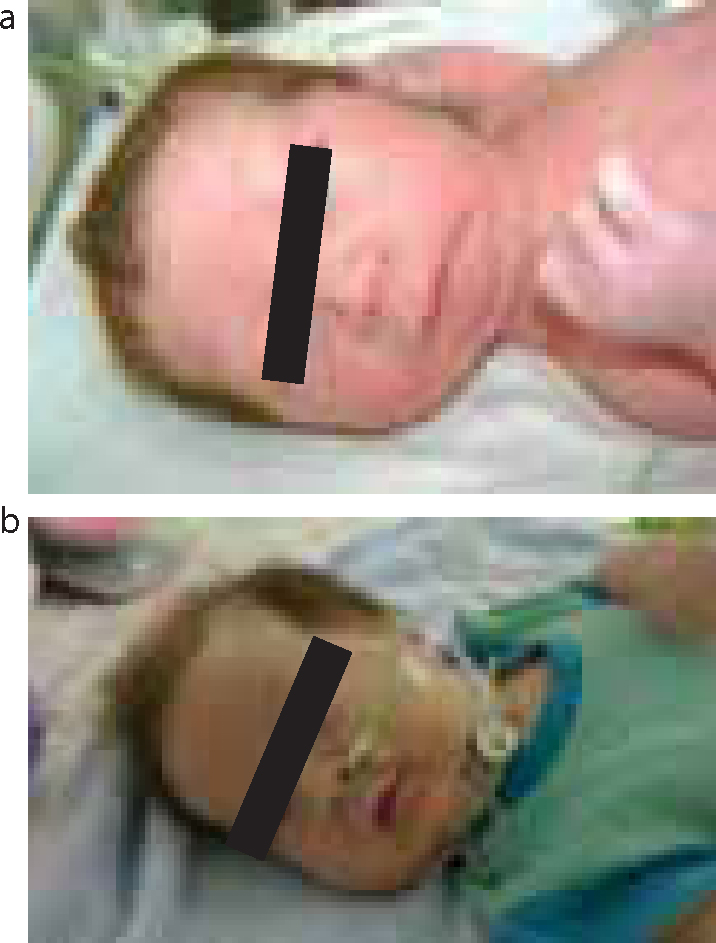
Treatment options depend on the severity of the obstruction. They would include:
Figure 9. A child with tracheostomy to allow breathing and with distractors in place to increase mandibular length and reduce obstruction episodes: (a) before surgery showing a severely retrognathic mandible; (b) and after surgery with significantly more prognathic mandible.
Post-operative period
This tends to happen within 24–48 hours of surgery. It is usually associated with palatal surgery or pharyngoplasties but, on occasion, can occur following lip repair/anterior rhinoplasty. Children are often placed in HDU following primary lip and palatal surgery to allow careful monitoring in the early post-operative period. This allows careful monitoring of the child and early intervention if the child develops any signs of respiratory distress.
Long-term sleep disordered breathing
All cleft children have the same risk as other children with regard to sleep disordered breathing and obstructive sleep apnoea, eg secondary to adenotonsillar hyperplasia. However, they may be at higher risk owing to their anatomical abnormalities being corrected with consequent narrowing of the nasopharynx.
A pharyngoplasty is sometimes performed to reduce the nasopharyngeal airway to help prevent nasal escape during speech. This has the potential detrimental effect of increasing the likelihood of apnoeic episodes. Careful pre-operative discussion and patient evaluation within the multidisciplinary team setting should be undertaken to discuss the risks versus benefits of such a procedure.
The complications of chronic obstructive sleep apnoea (OSA) include:
Hypoxemia;
Hypercarbinemia;
Neuropsychiatric problems; and
Decreased cognitive function.
In severe cases the chronic obstruction can result in pulmonary hypertension and cardiac failure. There is also a link between OSA in childhood and adult hypertension.5
Conclusions
ENT surgeons can offer a variety of skills useful to the cleft multidisciplinary team. With regard to hearing, they can maximize cleft children's hearing ability to prevent any disability and ultimately hearing handicap. Normal hearing is required to obtain normal speech acquisition, which is ultimately the goal of cleft palate surgery. Also, cleft children are at a higher risk of long-term hearing and ear problems that require careful follow-up. ENT surgeons can also assess and manage upper airway problems to prevent any acute or chronic sequelae that may develop.