Shaw WC, Williams AC, Sandy JR, Devlin HB. Minimum standards for the management of cleft lip and palate: efforts to close the audit loop. Ann Royal Coll Surg Eng. 1996; 78:110-114
London: HMSO; 1998
Shaw WC, Asher-McDade C, Brattström V, Dahl E, McWilliam J, Mølsted K, Plint DA, Prahl-Andersen B, Semb G The RP. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 1. Principles and study design. Cleft Palate Craniofac J. 1992; 29:(5)393-397
Prahl C, Prahl-Andersen B, van't Hof MA, Kuijpers-Jagtman AM. Infant orthopedics and facial appearance: a randomized clinical trial (Dutchcleft). Cleft Palate Craniofac J. 2006; 43:(6)659-664
This article discusses primary surgery for patients with cleft lip and palate, which in the UK would conventionally take place in the first year of life. Current protocols in the United Kingdom are described and some of the history in the surgical specialties that led to their development discussed. The basic principles of the surgery are explained and the impact of surgery on future facial aesthetics, dental development and speech are considered.
Clinical Relevance: Clefting of the lip produces a significant deformity and, although not functionally debilitating, will lead to a significant aesthetic impact, which in our modern day, aesthetically driven society can produce significant psychosocial consequences, even with repair.
Article
Aclefting of the palate has no aesthetic impact, but without adequate repair will lead to an inability to produce normal speech, will impact on hearing and the embarrassment of food and drink escaping through the nose.
The aims of surgery are therefore to produce a result that is both functionally and aesthetically as near normal as possible.
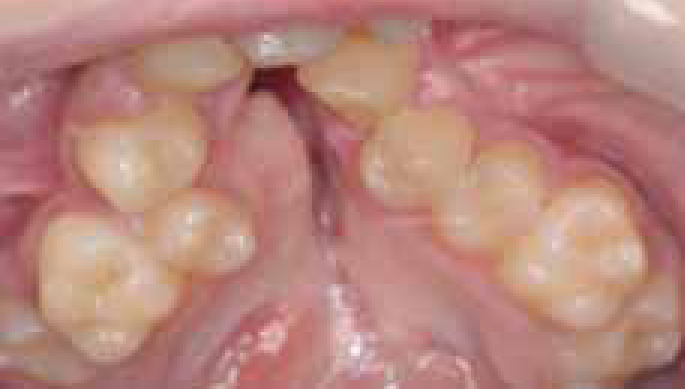
Historically, surgeons concentrated on closure of the clefts at all costs, which led to significant scarring and residual deformity with restricted facial growth (Figure 1).
Figure 1. An occlusal view of a constricted maxillary arch after numerous attempts to close palate.
Closure of the cleft is, however, much more complicated if a functional and aesthetic result is to be achieved. When a cleft occurs, not only is there often a deficiency of tissue, but the associated structures and muscles are also displaced. Surgery therefore aims to close the residual deformity with the minimum of scarring, and also to reposition these structures and, particularly muscles, in their correct orientation to give the best chance of normal function.
Surgical centres and collaboration
In 1996, the Royal College of Surgeons of England (RCS) Steering Group on cleft lip and palate published recommendations for Minimum Standards for the Management of Cleft Lip and Palate.1 These suggested ‘cleft care should be provided by multidisciplinary teams based in regional centres’. The group also recommended that a primary surgeon, who should have undergone a period of extended cleft training, should perform a minimum of 30 cases per year.
In 1995, The Clinical Standards Advisory Group (CSAG) commissioned a national study into cleft care in the UK. As part of this study, the aim was to assess the organization of cleft care in the UK and compare it to the recommendations made by the RCS Steering Group, the results of which were published in 1998.2
They suggested that, at that time, little centralization of services had taken place, leading to low volume primary surgery operators and few of the teams being able to provide all key services within their locality. This showed a clear need for reorganization, if adequate training, research and audit were to be achieved.
England and Wales now have 11 designated centres, with Scotland having a single service in the form of a Managed Clinical Network (MCN) – CLEFTSiS. Despite centralization, several challenges still exist in relation to primary surgery. Despite consensus in Europe on what constitutes optimal cleft care delivery, there is little evidence as to choosing treatment protocols for primary surgery. Throughout Europe there are diverse protocols with significant variation as to timing, number of operative procedures and the type of procedure performed for lip and palate closure.3 There are, however, a number of large multi-centre collaborative studies being undertaken that will hopefully answer some of the uncertainties that presently exist.
Lip surgery
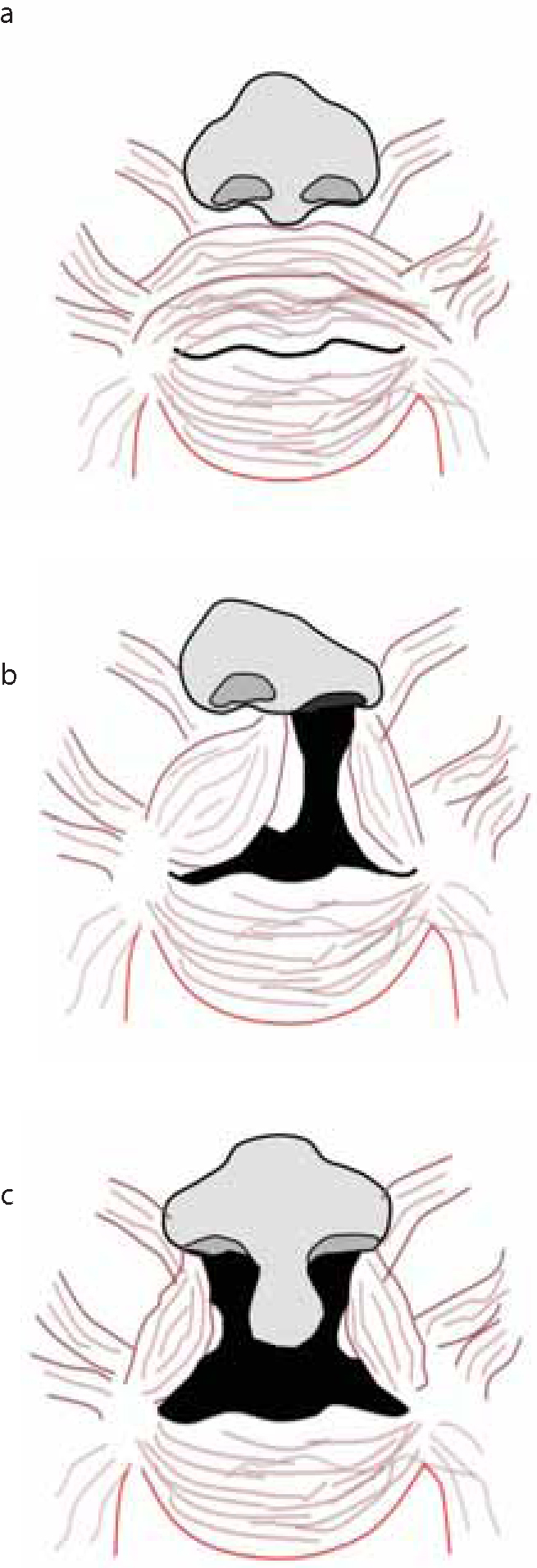
The aim of lip/nose surgery is to create an aesthetic and functional result with minimal scarring. There has been a gradual improvement in the aesthetic outcomes of lip closure and the nasal deformity that co-exists. The normal muscle of the lip is arranged in a circular ring around the mouth, the orbicularis oris muscle also interdigitates with other elevators and depressors of the lips. In the cleft patient, rather than forming a continuous ring, it is attached to the pyriform rim (Figure 2a, b). In a bilateral cleft there is no muscle at all in the prolabium (Figure 2a, c).
Figure 2.
(a) Normal muscle orientation in non cleft individual. (b) The impact of a cleft of the lip. (c) The impact of a bilateral cleft of the lip. Note altered position of insertion and the lack of continuity of the orbicularis oris muscle.
Although, with closure the aesthetics may be good, it will soon become obvious when the child smiles or pouts if the muscles have not been re-oriented in the correct direction.
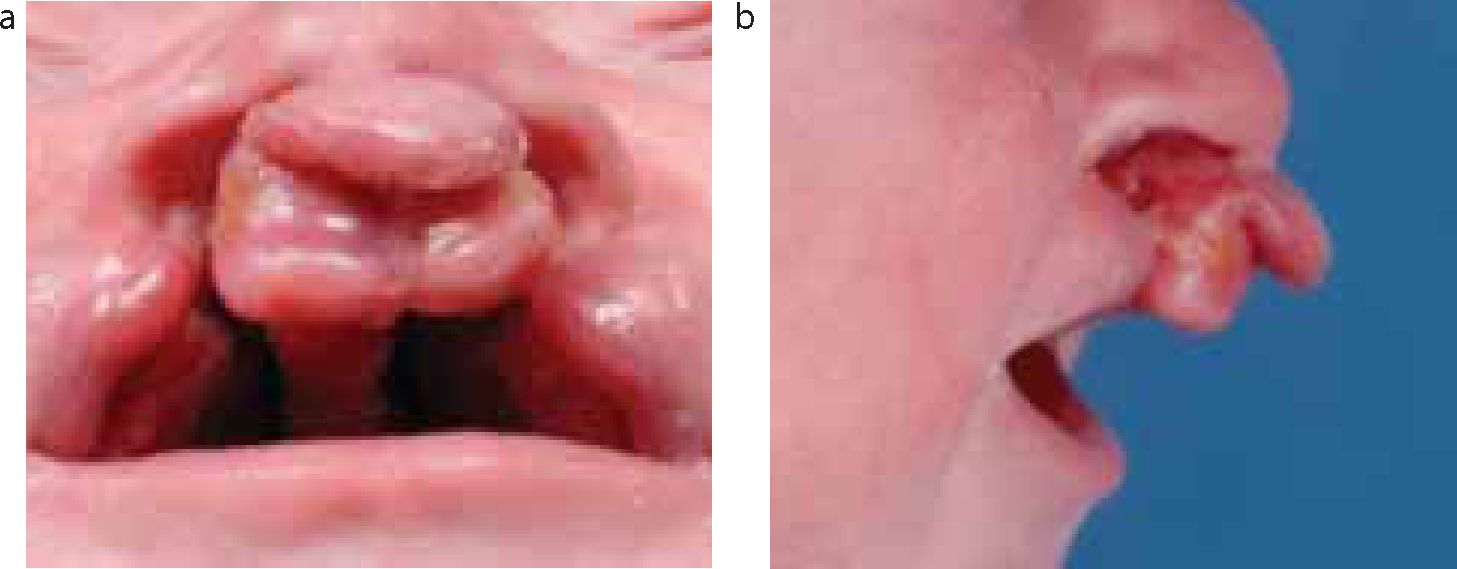
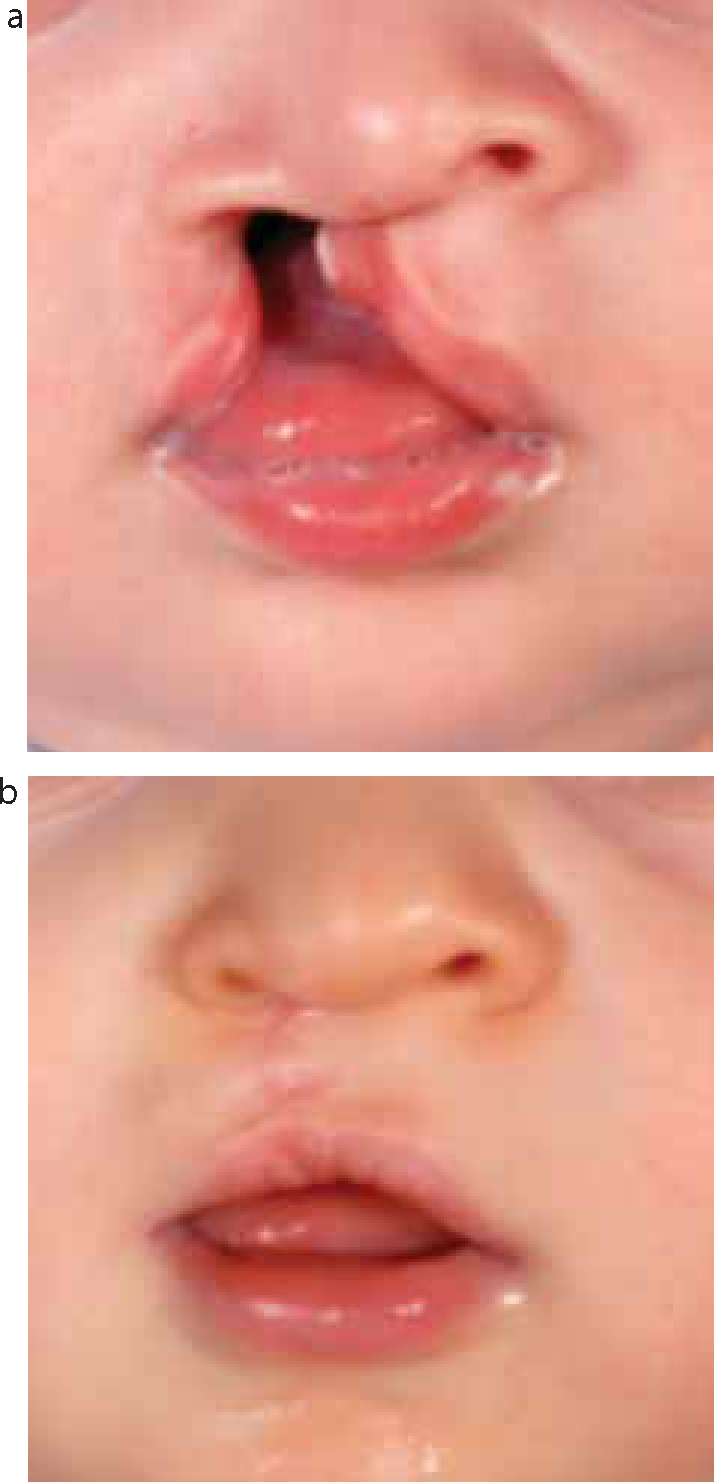
Where a unilateral cleft lip and palate exists, sometimes the gap between the two segments can be significant. A similar scenario exists with a bilateral cleft lip and palate where the prolabium and premaxilla may be suspended from the nasal tip (Figure 3).
Figure 3.
(a, b) A bilateral cleft lip and palate with significant displacement of the prolabium.
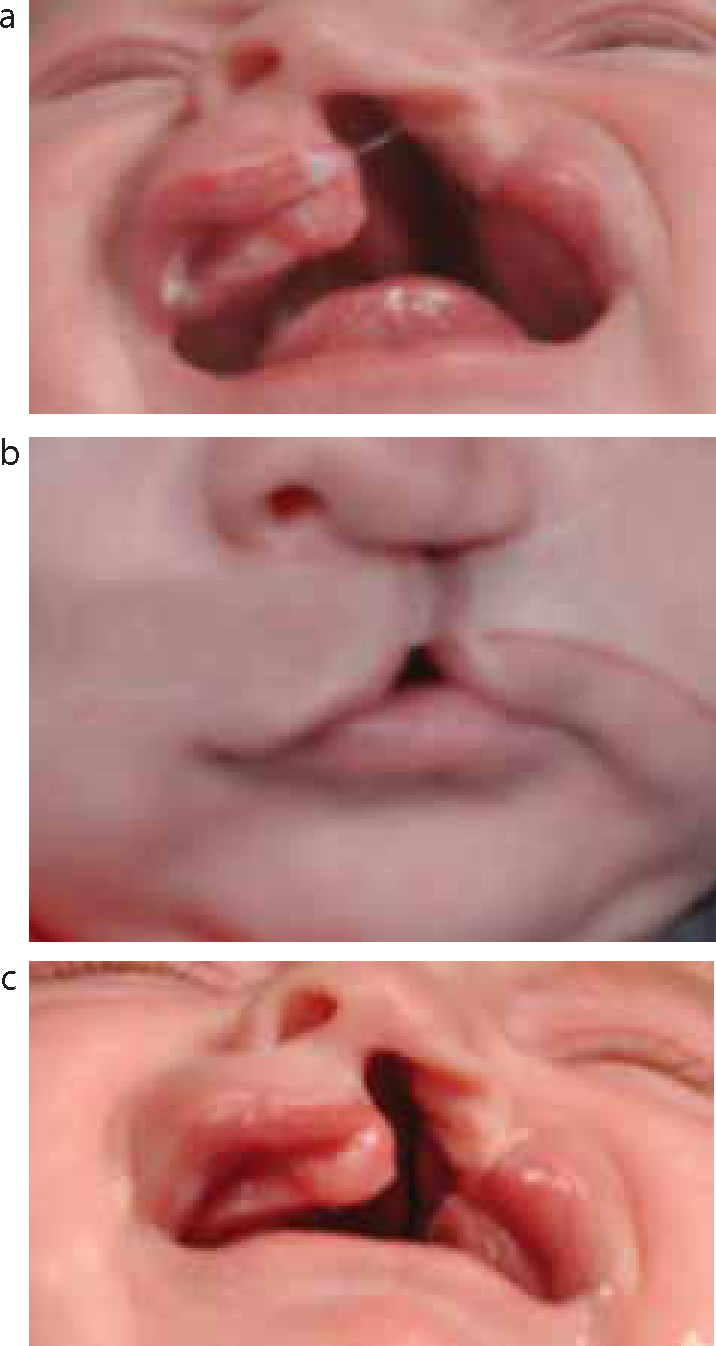
In both cases, the apposition of the segments may be improved by pre-surgical orthopaedics (PSO), adhesive strapping (Figure 4) or, in extreme cases, lip adhesions.
Figure 4. A child with a unilateral cleft lip and palate: (a) before strapping; (b) with strapping in place; and (c) after two weeks of strapping resulting in a reduced cleft width and closer approximation of the segment.
However, clinical trials in patients with unilateral cleft palate utilizing PSO suggest minimal benefit in either short- or long-term outcomes.4
In the United Kingdom, primary lip surgery usually takes place within the first 3–6 months. The most commonly utilized method is the rotational advancement closure and no tissue is discarded. As the flaps are rotated, the muscles are re-oriented into the correct position and sutured to produce the sphincter (Figure 5).
The challenges with bilateral cleft lip are greater for the surgeon, particularly if the prolabium is significantly displaced. Although pre-surgical orthopaedics can improve the segment approximation, there is still the issue of a lack of muscle in the prolabium; the philtrum is not present and the tissue deficiency is greater.
The deformity associated with the nose is as noticeable as the lip itself. Although results with a number of advocated procedures carried out at the same time as lip closure are encouraging in the short term, the aesthetics tend to deteriorate as the child grows.
The cleft through the alveolus is often left at this time or undergoes a single layer closure, utilizing a flap from the vomer. This obviously reduces the chance of damage to developing tooth buds, excessive scarring and collapse of the bony segments. Bone grafting and alveolar cleft closure (gingivoperioplasty) at this time has been advocated. It requires very close apposition of the bony segments and is usually preceded by a period of pre-surgical orthopaedics (naso-alveolar moulding) to achieve this. Although this appears attractive at first, as it may alleviate the need for bone grafting, long-term follow-up suggests that this is not the case and also leads to poor maxillary growth. The unrepaired alveolar cleft will be closed at the time of alveolar bone grafting; this is also a useful time to carry out any minor revisions as they will improve access to the graft for the surgeon. However, the commonest time for lip revision after primary surgery is prior to the child starting school, if he/she is becoming self-conscious.
Palatal surgery
Clefts of the hard palate can be either unilateral or bilateral with varying degrees of hard and soft tissue deficiency. Complete clefts of the hard palate extend forward to the incisive foramen; sometimes, when incomplete, the soft tissue defect may be less than the underlying bony defect. The extreme example of this is the submucous cleft palate, where the soft tissue is uninterrupted but there is an underlying bony defect.
The normal soft palate is composed of oral mucosa inferiorly, nasal mucosa superiorly and, between them, a complex arrangement of mucous glands, muscles and fibrous tissue or aponeurosis. At the free posterior end is the uvula and it is attached anteriorly to the hard palate through a fibrous aponeurosis.
The complex series of muscles, which are responsible for soft palatal function, form a series of slings meeting in the midline, the levators causing elevation of the palate and the palatopharyngeus and palatoglossus causing depression.
In clefts of the soft palate, the muscles that are unable to meet in the midline pass more anteriorly to fuse to the margins of the cleft and into the back of the hard palate.
Early pioneers in cleft surgery emphasized the importance of closure and lengthening of the palate, but this resulted in significant scarring; they were not concerned with a functional repair of the muscles. As a consequence, the extent of maxillary collapse and the speech results were disappointing.
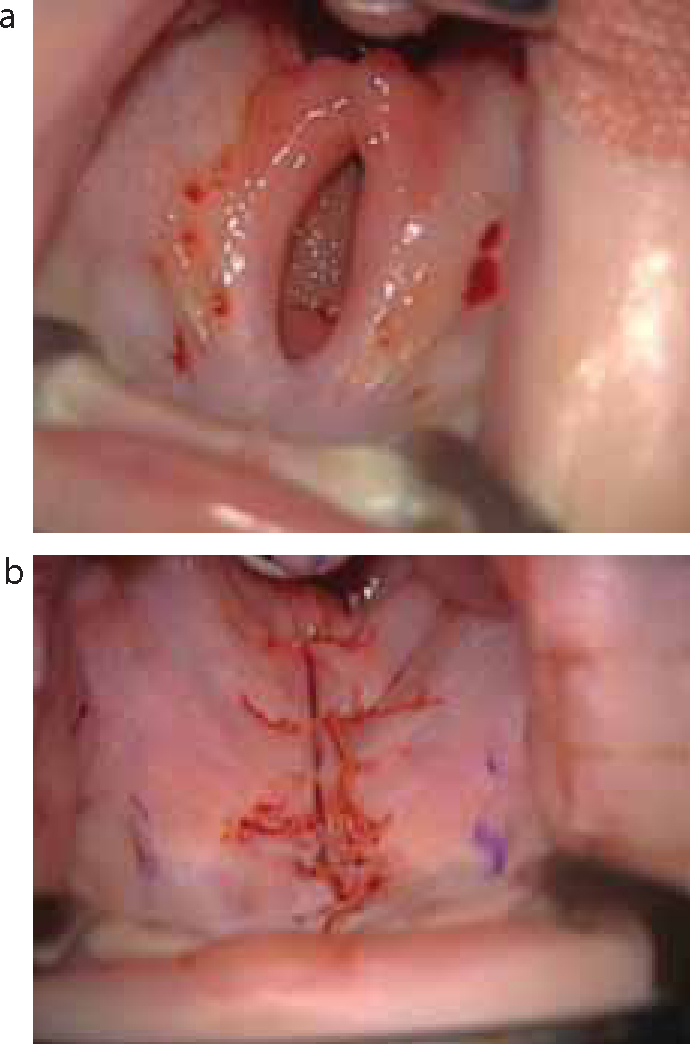
Modern techniques, rather than aiming for palate closure in one operation with extensive relieving incisions, aim to close in one or more stages (Figure 6). In the initial stage, the muscles of the soft palate are dissected, repositioned and re-oriented, to encourage normal function. The mucosa on the nasal side and on the oral side is closed with resorbable sutures. The repair is continued forward until the defect is closed, or until undue tension is encountered on the wound edges. If this is the case, the residual defect is closed at a second procedure, by which time it has usually significantly decreased in width. In cleft palate repair, the surgeon aims both to close the cleft and, more importantly, anatomically reconstruct the muscular ‘sling’ of the soft palate so that the velopharyngeal closure can be achieved.
Figure 6.
(a, b) Upper occlusal photographs showing a child with a cleft of the hard and soft palate: (a) pre- and (b) immediately post-repair.
The timing of surgery in cleft deformity is a matter of some debate, but in every case represents a compromise between function, development and appearance versus scarring and its effect on growth. In the UK, the aim is to close the palate by the end of the first year, producing a more normal anatomy and better functioning muscles before speech starts to develop fully. The children are, however, closely followed up and assessed by the speech and language therapists within the team and, where appropriate, more locally. This close monitoring allows prompt intervention in the form of therapy, or even further surgery, if appropriate.
Conclusions
Primary cleft surgery continues to develop in terms of procedure and timing. At present, it is not possible to say what constitutes the ideal protocol but, with numerous collaborative, multicentre trials coming to fruition, they will hopefully answer many of the presently unanswered questions.