Goaz PW, Stuart CW., 3rd edn. St Louis: Mosby; 1994
Daley TD, Pringle GA. Relative incidence of odontogenic tumours and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol. 1994; 77:276-280
Gorlin RJ. Cysts of the jaws, oral floor and neck, 6th edn. St Louis: Mosby; 1970
Colbert S, Brennan PA, Theaker J, Evans B. Squamous cell carcinoma arising in dentigerous cysts. J Craniomaxillofac Surg. 2012; 40:e355-357
Berdén J, Koch G, Ullbro C. Case series: treatment of large dentigerous cysts in children. Eur Arch Paediatr Dent. 2010; 11:140-145
Koca H, Esin A, Aycan K. Outcome of dentigerous cysts treated with marsupialization. J Clin Pediatr Dent. 2009; 34:165-168
Escoda Francoli J, Almendros Marqués N, Berini Aytés L, Gay Escoda C. Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2008; 13:438-443
Gnanasekhar JD, Walvekar SV, Al-Kandari AM, Al-Duwairi Y. Misdiagnosis and mismanagement of nasopalatine duct cyst and its corrective therapy. A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 80:465-470
Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst: an analysis of 334 cases. J Oral Maxillofac Surg. 1991; 49:268-271
Velesquez MT, Mason C, Coonar H, Bennett J. A nasopalatine cyst in an 8-year-old child. Int J Paediatr Dent. 1999; 9:123-127
Meyer AW. A unique paranasal sinus directly above the superior incisors. J Anat. 1914; 48:118-129
These case reports illustrate the management of two patients presenting with a dentigerous cyst and nasopalatine cyst, respectively. Both patients were treated with different surgical approaches and the associated teeth were successfully aligned with orthodontic appliances.
Clinical Relevance: Dental practitioners should be suspicious if teeth are missing past the ideal age of eruption, especially if the contralateral tooth has been erupted for at least 6 months. Initial investigations should involve radiographs to identify presence, or otherwise, of the tooth and prompt referral when appropriate.
Article
Dentigerous cysts
Dentigerous cysts are epithelial-lined cavities, typically enclosing the crown of an unerupted tooth at the cemento-enamel junction. As the follicle expands, fluid collects between the reduced enamel epithelium and the enamel of the unerupted tooth, possibly through the production of cell breakdown products. Following impeded eruption of a tooth, an increase in osmotic pressure is said to occur which can result in cyst formation.1 A dentigerous cyst may be suspected if the follicular space around an unerupted tooth is greater than 5 mm, as a normal follicular space is considered to be in the region of 3 mm.1
Dentigerous cysts are the most prevalent odontogenic cysts, making up 24% of all these cysts2 and reach a peak incidence between the ages of 20 and 40. Any tooth may be involved but the mandibular third molars are the most commonly affected.
Most dentigerous cysts are solitary, however, bilateral or multiple cysts may be found in association with certain syndromes, including cleidocranial dysplasia and mucopolysaccharidosis.3
Dentigerous cysts are often identified as an incidental finding on routine radiographs with a typical radiological appearance of a well-defined unilocular radiolucency with a sclerotic border, commonly surrounding the crown of an unerupted tooth. Signs and symptoms which may arouse suspicion include swelling, tooth displacement and/or mobility and sensitivity but there is usually no pain or discomfort associated with the cyst unless secondary infection occurs. A dentigerous cyst is usually lined by non-keratinized stratified squamous epithelium. Although benign, they will continue to expand and, if left untreated, will continue to be locally destructive. Malignant transformation is rare but has been reported in the epithelial lining cells,4 therefore all patients should continue to be reviewed radiographically following the removal of a dentigerous cyst.
Options for cyst management can vary from surgical enucleation to more conservative marsupialization. Marsupialization and decompression involve creating a small surgical window in the wall of the cyst, removing the contents and maintaining continuity between the cyst and oral or nasal cavity or maxillary sinus. Pressure is relieved through the creation of the accessory cavity and occasionally stents can be used to keep the opening patent. It is generally a more conservative approach and helps to preserve surrounding structures5 to allow growth and development to continue uninterrupted. Removable appliances may be useful following marsupialization to continue decompression of the cyst, obturate and maintain space if necessary.
The evidence for marsupialization as a management option is generally empirical in the form of case reports and case series. Berdén et al5 presented a case series of 11 children who had dentigerous cysts treated with marsupialization and decompression. Successful treatment was reported and all permanent teeth associated with the cysts, apart from two, erupted. Koca et al, in a recent case series,6 assessed treatment outcomes in children who had dentigerous cysts marsupialized and reported success in all 35 cases. In all cases, the involved teeth erupted and bony infill occurred.
Nasopalatine cysts
Studies have reported that nasopalatine cysts are the most common non-odontogenic cysts of the oral cavity,7,8 representing up to 1% of all maxillary cysts.7,9. They most commonly present between 40 and 60 years of age and are more frequent in males than in females, with a 3:17 ratio, respectively. It is unclear in which ethnic group nasopalatine cysts are more common,7,10 however, these lesions are uncommon in children, especially in Caucasian children.8
The nasopalatine cyst was first described by Meyer in 1914 and was considered to be the most common non-odontogenic cyst, accounting for approximately half of those reported.11,12,13,14
In the past, nasopalatine cysts have also been known as ‘anterior middle palatine cysts’ and ‘incisor duct cysts’, and were regarded as fissural cysts.7,15 Currently, according to the classification of the World Health Organization (WHO), these lesions are regarded as non-odontogenic cysts of the maxilla, together with maxillary midline cysts and nasolabial cysts.16
The origin of nasopalatine and dentigerous cysts is uncertain, with many authors suggesting a spontaneous proliferation theory7 or development from the epithelial remnants of the oro-nasal ducts within the incisive canals.8,10,11 Other aetiological factors have been proposed, including local trauma and infection. Blockage of glandular ducts, as well as racial or genetic factors are also possible causes mentioned in the literature.11
Histologically, the type of cystic epithelium varies according to the location involved (palatine, nasal or intermediate). A squamous cell epithelium is often observed, although a ciliary respiratory type epithelium can be seen where the cyst is located higher or nasally.8
Nasopalatine cysts are usually asymptomatic11 and are frequently incidental radiological findings, although pain can occur in larger more advanced cysts,7 and the most commonly reported clinical symptom is swelling affecting the anterior portion of the palate.11,17
Two cases are described below which demonstrate two different approaches to management of cysts where the aim of treatment was to preserve the impacted tooth.
Case 1
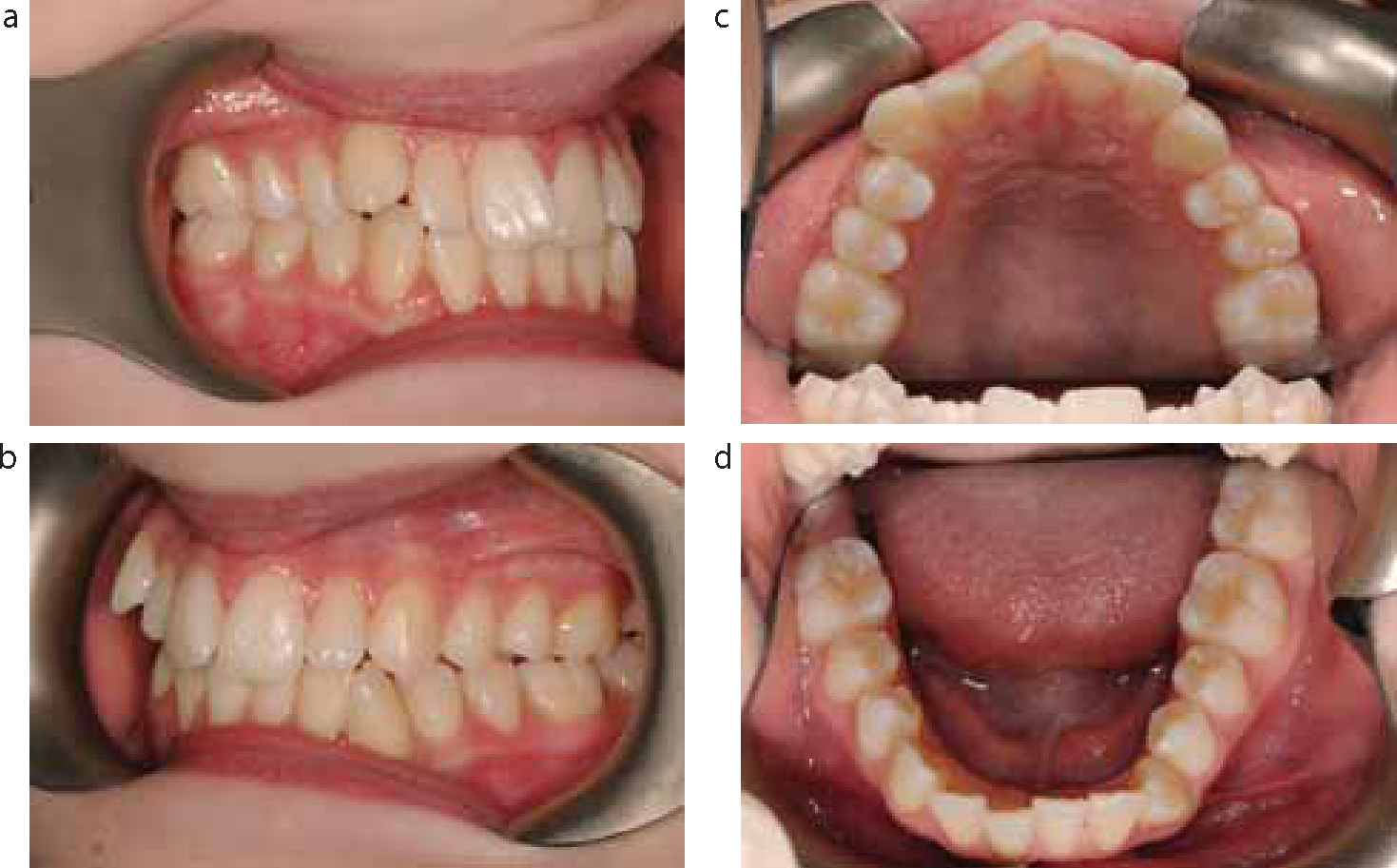
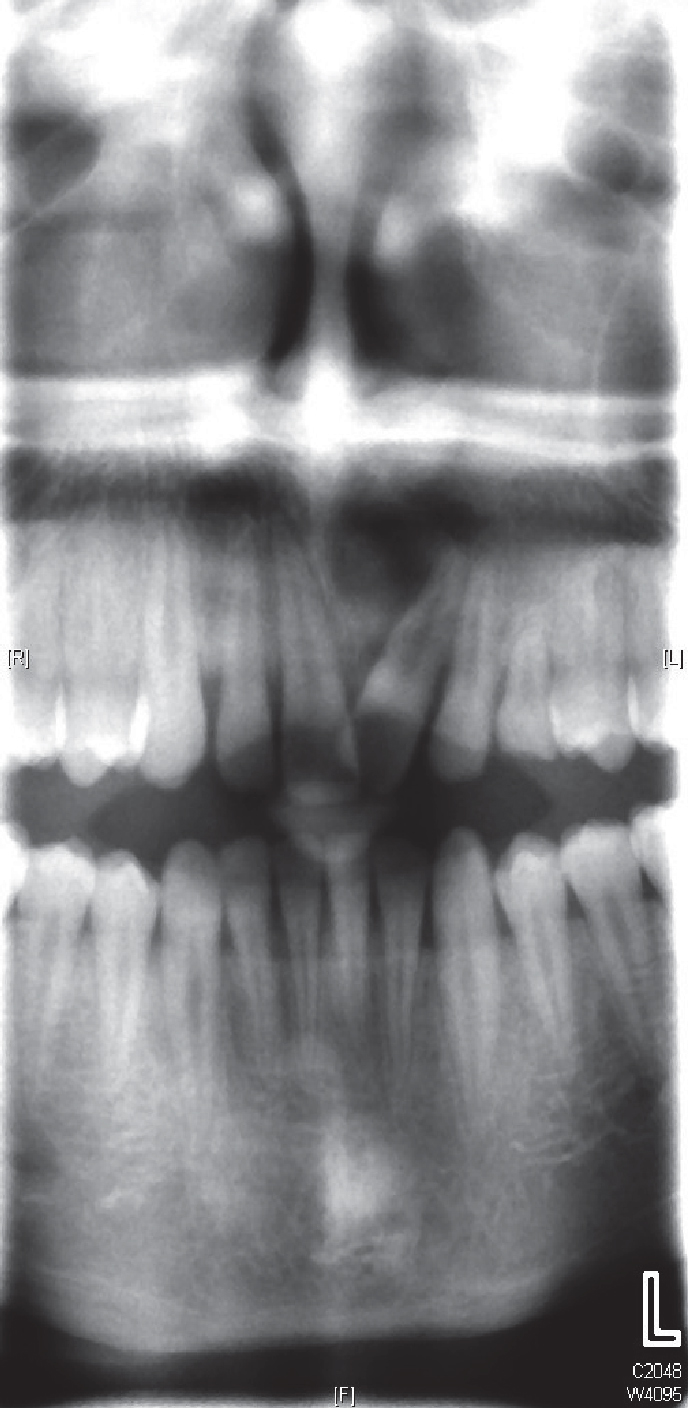
A 14-year-old female presented with mild Class I crowding to the orthodontic unit, dissatisfied with her dental alignment (Figure 1). A panoramic radiograph was taken as part of her initial assessment and a large cystic lesion was noted in the right angle of the mandible (Figure 2). It was unilocular with a well demarcated periphery. At her subsequent appointment, the patient was seen on a multidisciplinary orthodontic-surgical clinic.
Figure 1.
(a–d) Initial presentation views showing a Class I malocclusion with mild crowding.Figure 2. Panoramic radiograph showing initial presentation with the dentigerous cyst present in the right angle of mandible, associated with the unerupted LR7.
The decision was made to marsupialize the cyst owing to its significant size and a provisional diagnosis of a dentigerous cyst was made which was confirmed histopathologically. The cyst was marsupialized and the associated lower right second molar (LR7) preserved (Figure 3). The marked displacement of LR7 was identified and the patient was monitored. Consecutive radiographs taken post-operatively depict bony infilling taking place (Figure 4) and the downward migration of the LR7. Once sufficient bony infill had occurred and the LR7 had descended, the patient was treated with upper and lower fixed appliances and extraction of four second premolars to relieve crowding. Once the LR7 had erupted sufficiently, it was incorporated on to the lower fixed appliance in order to complete its alignment (Figure 5).
Figure 3. Panoramic radiograph taken immediately following marsupialization and decompression.Figure 4. Panoramic radiograph taken 6 months following surgery showing bony infill of the cystic cavity and the LR7 descending.Figure 5. Intra-oral view of lower arch showing that the LR7 has descended and is being aligned orthodontically.
Case 2
An 11-year-old boy was referred to the orthodontic department by an orthodontic specialist who had noted a large cyst associated with the upper left permanent central incisor (UL1) as an incidental finding on a periapical radiograph. The patient presented in the late mixed dentition with a retained upper left deciduous canine and the UL1 which was rotated and tipped mesially (Figure 6). In addition, a small degree of bony expansion was evident in the maxillary anterior left buccal sulcus.
Figure 6. Intra-oral view showing the initial presentation of a case with displacement of UL1.
Radiographs taken showed a well demarcated circular radiolucency associated with the root apex of UL1 and an associated supernumerary tooth contained within the cyst (Figure 7). Again, this patient was reviewed on a multidisciplinary orthodontic-surgical clinic. Treatment involved enucleation of the cyst with concurrent removal of the associated supernumerary. Histopathological analysis of the specimen confirmed a nasopalatine cyst.
Figure 7. Intra-oral radiographs from referring practitioner showing initial radiographic presentation of a cyst extending from UL1 to the retained ULC.
The patient was reviewed radiographically on a regular basis and, once bony infilling started to occur, he was treated orthodontically with upper and lower fixed appliances to complete alignment, particularly of the UL1. Radiographs taken at 2-(Figure 8) and 3-(Figure 9) year intervals post-operatively showed progressive bony infill of the cystic cavity and the patient achieved a good orthodontic result (Figure 10).
Figure 8. Panoramic radiograph taken 2 years following cyst enucleation showing good bony infill.Figure 9. Panoramic radiograph taken 3 years following enucleation showing resolution of the cystic cavity.Figure 10. Intra-oral view taken 4 years following enucleation, at the completion of orthodontic alignment.
Discussion
The development of dentigerous cysts around unerupted teeth is relatively uncommon and, when diagnosed, the options to manage the cyst with enucleation or marsupialization must be considered. The decision to retain or remove associated teeth and the size of the cyst are important factors in treatment planning. Enucleation offers the entire cyst for histopathological investigation but can lead to loss of the associated tooth. Marsupialization in the paediatric patient may be preferable to enucleation, as teeth are more likely to be preserved and often aligned, but has the disadvantage that the entire specimen is not available for investigation. In the case of large lesions, marsupialization preserves valuable tissue and there is anecdotal evidence that this may have less of an effect on further growth and development. In the case of nasopalatine cysts, frequently the treatment of choice is enucleation as these lesions are less likely to be associated with unerupted teeth. The role of the orthodontist is important, not only in the diagnosis, but also in alignment of teeth and, if appropriate, in the fabrication of removable appliances for obturation and space maintenance.
When new patients are seen, it is useful to undertake radiographic examination of all unerupted teeth. Bitewing and periapical radiographs may fail to demonstrate the true extent of cystic lesions fully, therefore a panoramic radiograph is likely to allow better visualization.
If a tooth is absent, the old rule of count or account is very important, as a tooth missing from the line of the arch may be present a significant distance away from a typical ectopic position. Radiographs are essential to assess tooth position and, if teeth are absent, the dentist should be aware that these teeth may actually be very displaced.
Conclusion
The cases described show two examples of displaced teeth associated with cysts managed with different surgical approaches. The importance of good quality radiographs has been demonstrated, both in order to identify tooth position and to monitor the cyst, particularly post-operatively. The option to preserve any associated teeth should be considered as teeth often have the ability to erupt towards the line of the arch when an obstruction is removed. This should be considered within the treatment plan, particularly when discussing treatment options during the consent process.