MacPhee CG The incidence of erupted supernumary teeth in consecutive series of 4000 school children. Br Dent J. 1935; 58:59-60
DiBiase DD Midline supernumaries and eruption of maxillary central incisors. Trans BSSO. 1968–1969; 83–88
Brin I, Zilberman Y, Azaz B The unerupted maxillary central incisor: review of its aetiology and treatment. ASDC J Dent Child. 1982; 49:352-356
Andreasen JO Etiology and pathogenesis of traumatic dental injuries. A clinical study of 1,298 cases. Scand J Dent Res. 1970; 78:(4)329-342
Yeung K, Cheung R, Tsang M Compound odontoma associated with an unerupted and dilacerated maxillary primary central incisor in a young patient. Int J Paediatric Dent. 2003; 13:208-212
Andreasen JO, Ravn JJ The effect of traumatic injuries to primary teeth on their permanent successors. II. A clinical and radiographic follow-up study of 213 teeth. Scand J Dent Res. 1971; 79:(4)284-294
Turgut MD, Tekçiçek M, Canoglu H An unusual developmental disturbance of an unerupted permanent incisor due to trauma to its predecessor - a case report. Dent Traumatol. 2006; 22:(5)283-286
Kuvvetli SS, Seymen F, Gencay K Management of an unerupted dilacerated maxillary central incisor: a case report. Dent Traumatol. 2007; 23:(4)257-261
Cunha RF, Pugliesi DMC, Vieira AEM Oral trauma in Brazilian patients aged 0–3 years. Dent Traumatol. 2001; 17:210-212
Stewart DJ Dilacerate unerupted maxillary central incisors. Br Dent J. 1978; 145:229-233
Crescini A, Doldo T Dilaceration and angulation in upper incisors consequent to dental injuries in the primary dentition: orthodontic management. Prog Orthod. 2002; 3:29-41
Kokich VG, Crabill KE Managing the patient with missing or malformed maxillary central incisors. Am J Orthod Dentofacial Orthop. 2006; 129:(Suppl 4)S55-63
Nashashibi IA Orthodontic movement of a palatally displaced, dilacerated, unerupted maxillary central incisor. J Pedod. 1986; 11:83-90
Sandler PJ, Reed RT Treatment of a dilacerated incisor. J Clin Orthod. 1988; 22:374-376
Arenas M, Barberia E, Lucavechi T, Marota M Severe trauma in the primary dentition - diagnosis and treatment of sequelae in permanent dentition. Dent Traumatol. 2006; 22:226-230
Farronato G, Maspero C, Farronato D Orthodontic movement of a dilacerated maxillary incisor in mixed dentition treatment. Dent Traumatol. 2009; 25:451-456
Ak AT, Eden E, Tasdemir OO Treatment of sequelae in permanent dentition after severe trauma in primary dentition. Dent Traumatol. 2008; 24:e31-e33
Uematsu S, Uematsu T, Furusawa K, Deguchi T, Kurihara S Orthodontic treatment of an impacted dilacerated maxillary central incisor combined with surgical exposure and apicectomy. Angle Orthod. 2004; 74:132-136
Czochrowska EM, Stenvik A, Album B, Zachrisson BU Autotransplantation of premolars to replace maxillary incisors: a comparison with natural incisors. Am J Orthod Dentofacial Orthop. 2000; 118:592-600
Kocadereli I, Turgut MD Surgical and orthodontic treatment of an impacted permanent incisor: case report. Dent Traumatol. 2005; 21:234-239
Macias E, Carlos F, Cobo J Posttraumatic impaction of both maxillary central incisors. Am J Orthod Dentofacial Orthop. 2003; 124:331-338
Lin Y-TJ Treatment of an impacted dilacerated maxillary central incisor. Am J Orthod Dentofacial Orthop. 1999; 115:406-409
Topouzelis N, Tsaousoglou P, Pisoka V, Zouloumis L Dilaceration of maxillary central incisor: a literature review. Dent Traumatol. 2010; 26:335-341
McNamara T, Woolfe SN, McNamara CM Orthodontic management of a dilacerated maxillary central incisor with an unusual sequela. J Clin Orthod. 1998; 32:293-297
Multidisciplinary management of an impacted maxillary central incisor with a severe crown dilaceration Lisa Walshe Ciara Scott Orthodontic Update 2025 8:3, 86-90.
Authors
LisaWalshe
BA, BDentSc(TCD), MFDS(RCSI)
Oral and Maxillofacial Registrar, St James's Hospital, James's Street, Dublin 8
An 8-year-old girl presented with an unerupted upper right central incisor. Clinical and radiographic examination revealed a severe crown dilaceration. Her treatment involved a multidisciplinary approach, including surgical exposure, orthodontics and restorative treatment. The outcome was the accomplishment of a vital, functional and aesthetic maxillary central incisor with a good prognosis.
Clinical Relevance: This case report describes how a dilacerated upper incisor, which has failed to erupt and appears to be of poor prognosis, can be aligned with a satisfactory aesthetic and functional outcome. Alignment of the affected tooth improves dental appearance in the medium term and maintains alveolar bone if restorative replacement is required in the longer term.
Article
Lisa Walshe
An upper central incisor will usually erupt between 7 and 8 years old. Dental age and chronological age do not always correlate, but a central incisor should erupt within 6 months of the contralateral tooth and within 12 months after the lower incisors. The incidence of unerupted maxillary central incisor teeth in the 5–12 year-old group has been reported as 0.13%.1 In a referred population to regional hospitals the prevalence has been estimated as 2.6%.2 Maxillary incisors are the third most commonly impacted teeth in Caucasians, following the third molars and maxillary canines. It is important to detect and manage the problem as early as possible, as missing upper incisors are regarded as unattractive, space can be lost and management may be easier in the younger patient.3
Aetiology
Delayed eruption of maxillary central incisors can be classified into two causative groups (Table 1):
Hereditary; and
Environmental.
Hereditary
Environmental
Supernumerary teeth
Cleft lip and palate
Cleidocranial Dysostosis
Odontomes
Abnormal tooth/tissue ratio
Generalized retarded eruption
Gingival fibromatosis
Trauma
Early extraction or loss of deciduous teeth (with or without space loss)
Retained deciduous teeth
Cystic formation
Endocrine abnormalities
Bone disease
A detailed dental and medical history should be taken, including any history of dental trauma.
Pre-school age children may not have yet developed the psycho-motor skills needed to perform precise and safe movements and, as a result, they are susceptible to falls and other injuries.4 The prevalence of traumatic injuries to the primary dentition ranges from 11% to 30%.5 In contrast to the hard-tissue injuries that are more commonly seen in permanent dentition, luxation injuries predominate in the primary dentition.
Perhaps due to the larger bone marrow space resulting in high elasticity of alveolar bone surrounding the primary teeth,4 intrusive luxations constitute 4.4% to 22% of traumatic injuries in the primary dentition.4,5 Developmental disturbances of the successor permanent tooth can occur as a result of the close proximity of the developing permanent tooth germ to the primary root apex. With an overall prevalence of 41%,6 these developmental disturbances include:
White or yellow-brown enamel discoloration with or without enamel hypoplasia;
A study of Brazilian children aged up to 3 years of age showed an incidence of 16.3% of traumatic injuries and falls represented the most common aetiology for dental injuries. Intrusion was the dental injury in 12.5% of cases. The most frequently affected teeth were the primary maxillary central incisors (86%). In 12.5% of the cases recorded, the parents did not remember the age of the child at the time of the trauma.9 These injuries may have serious consequences for permanent teeth.
Dilaceration
Dilaceration is characterized by an angulation between the crown and root, usually resulting in non-eruption of the tooth. A study of 41 dilacerated unerupted maxillary central incisors revealed that 7% were associated with cysts or supernumary teeth, 22% resulted from trauma to the deciduous predecessor and the remaining 71% were developmental in nature.10 The direction and the timing of the injury to the permanent tooth germ determine the location of the dilaceration on the tooth. The extent of the disturbance of the developing germ is related to the stage of germ development and to the intensity, severity and direction of the impact.11 In the case presented, the injury occurred at age 1 so the developing crown was affected. Loss of a permanent central incisor is significant both aesthetically and functionally. If the malformation is severe or the tooth is ankylosed, the incisor may have to be removed. However, alveolar bone loss will follow and will compromise the site for future implant placement. An alternative strategy is to allow spontaneous space closure in the anterior incisor region and then to open up space with fixed appliances prior to definitive restoration in the permanent dentition. This will preserve more alveolar bone and normal gingival contour.12 Both methods have associated problems: orthodontic space closure is seldom indicated and aesthetically satisfactory, whilst space maintenance using a removable prosthetic appliance during childhood and adolescence may be unsatisfactory for psychological reasons, hence alignment of the dilacerated incisor may offer the most ideal treatment option. The unerupted tooth may be brought into the line of the arch by surgical exposure and orthodontic alignment.13,14 Elective root filling or crown reshaping may be required where there is unfavourable labial root dilaceration. The timing of intervention has been suggested as being important, with several studies suggesting that the younger the age, the quicker the tooth erupts.3 The success rate of an impacted dilacerated tooth, therefore, depends on the degree of dilaceration, stage of crown and root formation, and position of the tooth.
Case report
The female patient presented at 8.5 years old. She was referred to the Regional Orthodontic Unit as her GDP was concerned about the delay in the eruption of her maxillary right central incisor. The left central incisor had erupted 12 months previously and it had been 6 months since the upper right deciduous central incisor had exfoliated. Her clinical history revealed a history of dental trauma at the age of 1, as a result of a fall. She had no relevant medical history.
Intra-oral examination showed that she was in the early mixed dentition, with early loss of the lower primary molars. The upper left central incisor was fully erupted with normal crown anatomy. The upper lateral incisors were partially erupted (Figure 1). The impacted incisor's crown was palpable as a labial bulge high in the sulcus.
Figure 1.
(a) Dentition at presentation. (b) Occlusal view at presentation.
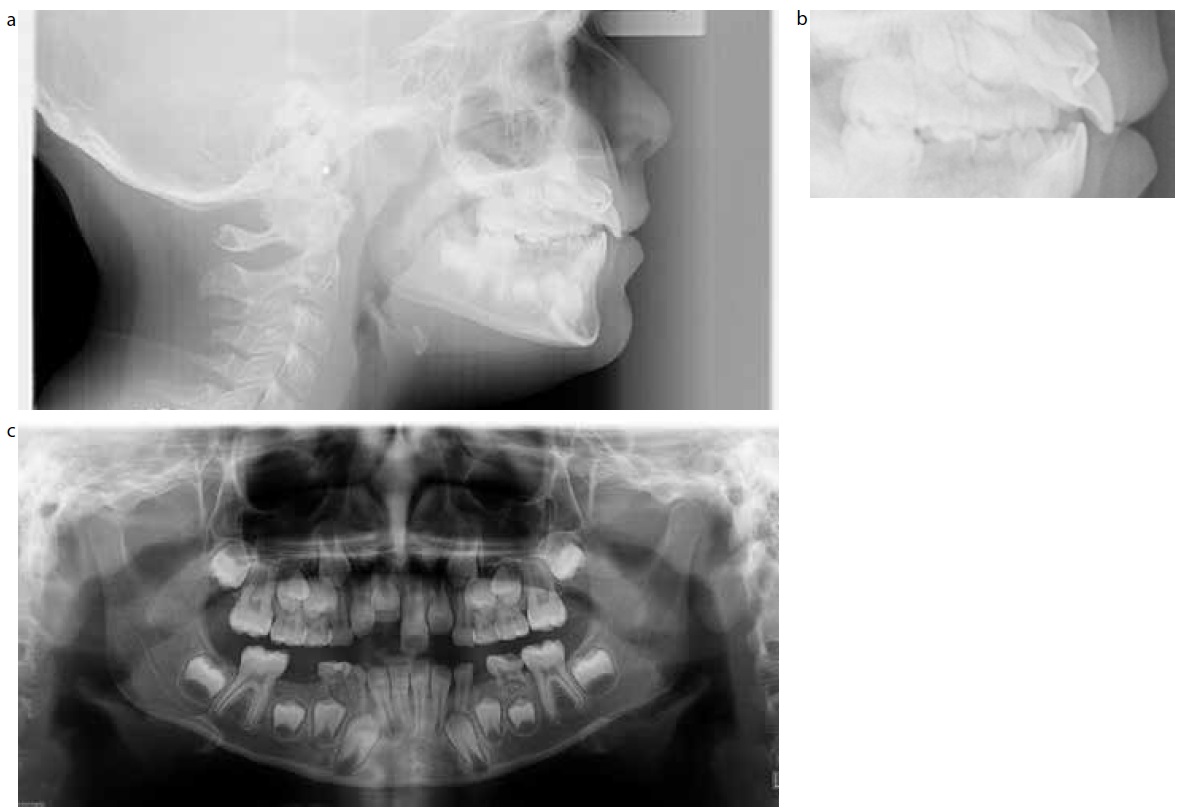
Radiographic examination (Figures 2–4) revealed a marked crown dilaceration of the impacted maxillary right central incisor. The lateral cephalogram clearly showed that the tooth was buccally placed with a 60–90° deviation in the crown formation. The dilaceration was within the crown of the tooth and the root appeared to be developing normally with a normal root canal. The upper right lateral incisor also appeared hypoplastic.
Figure 2.
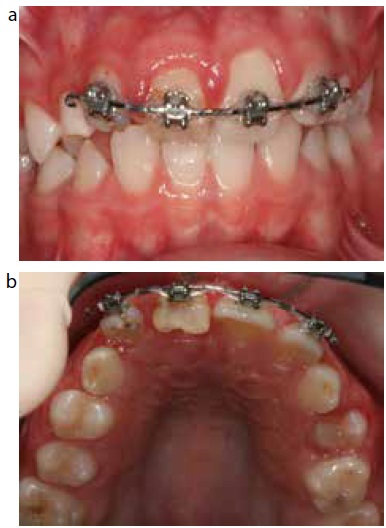
(a) Lateral ceph taken at presentation. (b) Crop of lateral ceph to show dilacerated crown. (c) OPG at presentation.Figure 3.
(a) Centre view mid treatment; more root torque was required to improve the emergence profile. (b) Occlusal view mid treatment demonstrating degree of dilaceration.Figure 4. (a) Periapical mid treatment shows normal root anatomy.Figure 4. (b) OPG mid treatment shows normal root anatomy and alignment and developing dentition.
A couple of treatment options were considered and discussed with the patient and her parents, outlining the relative potential benefits and risks:
Surgical removal of the impacted incisor and subsequent restoration with a bridge or implant after orthodontic space opening when somatic growth completes;
Surgical exposure of the impacted incisor and orthodontic traction to align the dilacerated tooth, utilizing fixed appliances.
They elected to proceed with orthodontic treatment to align the dilacerated central incisor. They were informed that the dilacerated tooth may not erupt and would have a poor appearance when it erupted that would require camouflage. It may not have a good long-term prognosis, however, this offered the best medium-term option aesthetically whilst maintaining the bone for a future implant if the prognosis of the central was poor.
Treatment plan
Treatment involved a combination of oral surgery, orthodontics and restorative intervention.
Surgical
Referral for closed exposure UR1: a full thickness mucoperiosteal flap was raised to gain access to the impacted incisor and a gold chain was bonded to the tooth and the flap was replaced. The bracket was bonded palatally to avoid early buccal fenestration through the nonkeratinized mucosa, which would result in an unfavourable gingival contour.
Orthodontic
A sectional fixed orthodontic appliance was bonded to the other incisors and primary canines. Once in a rectanglar steel base archwire, orthodontic traction was applied, using an elastomeric chain. Once erupted, an orthodontic bracket was bonded on the labial surface to continue alignment. Extra-labial root torque was bent into the archwire to improve the root torque and emergence profile of the tooth. A mid-treatment periapical radiograph revealed that root formation was developing normally and there were no signs of resorption (Figure 4). The poor quality, hypoplastic enamel on the dilacerated crown presented problems with bonding of the orthodontic appliance, as well as sensitivity of the tooth once erupted. The total orthodontic treatment time was 18 months. During treatment, the patient was referred for restorative assessment and she was reviewed prior to debond.
Restorative
The crown was reduced and a direct composite veneer restoration was placed on the labial surface of the dilacerated incisor. This enhanced the aesthetics which were compromised as a result of the discoloration and hypoplastic enamel and the poor tooth anatomy. The lateral incisor was also restored. There was no indication for root canal treatment to be performed at this stage and continued monitoring of vitality and root formation was planned. The patient then had an Essix retainer fitted for retention.
By the end of treatment, tooth function and aesthetics had been restored. The gingival margins were adequate and no loss of attachment was found on the labial surface of the dilacerated tooth (Figures 5 and 6). Probing did not show periodontal damage. The tooth had good periodontal health and a normal root length. Radiographically, the newly positioned incisor revealed a healthy tooth with no apparent root resorption; the tooth was asymptomatic and pulp testing revealed a vital pulp. Long-term follow-up is necessary to monitor the affected tooth and evaluate the necessity for endodontic treatment or further restorative treatment in the future.
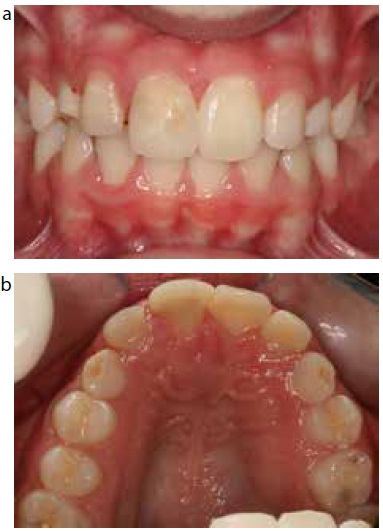
Figure 5.
(a) Centre view at debond. (b) Occlusal view at debond.Figure 6.
(a) Centre view following restoration. (b) Occlusal view following restoration.
Discussion
Trauma to the primary dentition, especially traumatic intrusion, may result in dilaceration of the developing permanent tooth and discoloration of the crown. Eruption of the permanent tooth may not occur.15
There are contrasting opinions on the treatment options available in cases of dilacerated teeth.16 Ak et al surgically removed the permanent incisor and constructed an aesthetic fixed appliance with the crown of the extracted tooth, later replaced by an implant when the patient ceases to grow.17 Extraction of the impacted central incisor, closure of the space and alignment of the lateral incisor in place of the central incisor is a possible alternative.18 Czochrowska et al19 have combined surgical removal of the impacted tooth with autotransplantation of a premolar providing ‘physiologically sound results’.
However, several authors8,11,16,18,20,21,22 have shown that surgical exposure and orthodontic traction can be used to manage impacted maxillary anterior teeth successfully. The disadvantages include treatment time, management of a younger patient and the prognosis of the tooth involved, including the risk of ankylosis, non-vital pulps, root resorption, root exposure, and loss of attachment that may be associated with this method.23 Historically, the treatment of choice was extraction and the restoration of choice for the missing incisor was a fixed or removable prosthesis. However, now implants are easily available, loss of so much alveolar bone after removal of an anterior tooth in a young child can compromise the site and necessitate bone grafting later when implants are planned. Also, patients are less accepting of wearing a temporary anterior tooth during their adolescent years. Therefore, using the dilacerated tooth as a temporary measure to hold the space offers acceptable aesthetics and maintains bone, so may be the most ideal treatment option in the short term, even if it may not have a good long-term prognosis. The degree and level of the tooth dilaceration, vertical position, and the root maturity are factors determining the success rate of orthodontic-surgical management of the impacted dilacerated tooth.
Reports on the management of severely dilacerated anterior teeth, however, are few.22,24 This could be due to the clinical difficulty of bringing the dilacerated tooth into the correct position. Parents and clinicians may be reluctant to plan treatment for young children when the prognosis is questionable. However, early loss of the permanent tooth and alveolar bone may affect the long-term restorative options and prognosis of prosthodontic treatment. If the impacted incisor is diagnosed in an 8-year-old and an implant cannot be placed until the patient has stopped growing, there is a time frame of at least 10 years when the patient will need a temporary incisor. The patient's own tooth should offer the most biocompatible, periodontal, functional and aesthetic result, even if the long-term prognosis is not favourable. Importantly, it will maintain adequate space and bone for later implant placement. Becker suggested that alignment of the dilacerated tooth, even if this required the amputation of the severely dilacerated crown or root, may offer a better restorative site.25 Kuvvetli et al8 concluded that, if the condition is diagnosed early, if the stage of root development and the shape of the crown are appropriate and, finally, if the patient can comply with the procedures involved, the guided eruption of the tooth may be accepted as the best treatment option. Macias et al21 also assert that guided eruption of impacted teeth must always be considered in young patients because this technique can lead to very acceptable results at the periodontal, occlusal and aesthetic levels.
Conclusions
This article describes the successful treatment of an impacted dilacerated maxillary central incisor crown using a multidisciplinary approach involving oral surgery, orthodontics and restorative dentistry. Considering the many risks and consequences involved, a multidisciplinary approach is essential when orthodontically moving an impacted dilacerated permanent incisor. This is often the optimum approach when the patient and parents are willing to comply.