Oliver RG, Edmunds DH, Jagger RG, Jagger DC A combined orthodontic/restorative clinic. Rationale, evolution, and experience. Br J Orthod. 1997; 24:159-162
Williams AC, Shaw WC, Devlin HB Provision of services for cleft lip and palate in England and Wales. Br Med J. 1994; 309
Cobourne M, Williams A, McMullan R A Guideline for the Extraction of First Permanent Molars in Children. R Coll Surg Eng. 2009;
Kokich VO, Kinzer GA Managing congenitally missing lateral incisors part 1: canine substitution. J Esthet Restor Dent. 2005; 17:5-10
Morgan C, Howe L The restorative management of hypodontia with implants: 2. Planning and treatment with implants. Dent Update. 2004; 31:22-30
Kokich VG, Spear FM Guidelines for managing the orthodontic-restorative patient. Semin Orthod. 1997; 3:3-20
Jalevik B, Klingberg G Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent first molars. Int J Paediatr Dent. 2002; 12:24-32
Sandler PJ, Atkinson R, Murray A For Four Sixes. Am J Orthod Dentofacial Orthop. 2000; 117:418-434
Ay S, Agar U, Bicakci AA, Kosger HH Changes in mandibular third molar angle and position after unilateral mandibular first molar extraction. Am J Orthod Dentofacial Orthop. 2006; 129:36-41
Yavuz I, Baydas B, Ikbal A, Dagsuyu IM, Ceylan I Effects of early loss of permanent first molars on the development of third molars. Am J Orthod Dentofacial Orthop. 2006; 130:634-638
Thilander B, Skagius S Orthodontic sequelae of extraction of permanent first molars. A longitudinal study. Rep Cong Eur Orthod Soc. 1970; 429-442
Williams JK, Gowans AJ Hypomineralised first permanent molars and the orthodontist. Eur J Paediatr Dent. 2003; 4:129-132
Chadwick BL, White DA, Morris AJ, Evans D, Pitts NB Non-carious tooth conditions in children in the UK, 2003. Br Dent J. 2006; 200:(7)379-384
Robertson A, Andreasen FM, Andreasen JO, Noren JG Long-term prognosis of crown-fractured permanent incisors. The effect of stage of root development and associated luxation injury. Int J Paediatr Dent. 2000; 10:(3)191-199
Andreasen JO, Andersson L, Tsukiboshi M Auto-transplantaion of teeth to the anterior region, 4th edn. Oxford: Blackwell; 2007
Amos MJ, Day PF, Littlewood SJ Autotransplantation of teeth: an overview. Dent Update. 2009; 36:102-113
Andreasen JO, Paulsen HU, Yu Z, Bayer T, Schwartz O A long-term study of 370 auto-transplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod. 1990; 12:14-24
Day PF, Kindelan SA, Kindelan JD, Duggal MS Dental trauma: part 2. Managing poor prognosis anterior teeth - treatment options for the subsequent space in a growing patient. J Orthod. 2008; 35:(3)143-155
Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU Outcome of tooth transplantation: survival and success rates 17-41 years post treatment. Am J Orthod Dentofacial Orthop. 2002; 121:(2)110-119
Multidisciplinary care – how should we manage the complex orthodontic/paediatric dentistry case? part 1 Farnaz Parvizi Peter JM Crawford Nikki Atack Orthodontic Update 2025 5:2, 38-47.
These two articles aim to outline the importance of combined paediatric dentistry-orthodontic planning in the management of complex cases of the developing dentition. They will use case studies to highlight those patients who would most benefit from such a combined approach.
Clinical Relevance: For patients who present with complex needs in the developing dentition, it is important that the paediatric and orthodontic teams work closely in order to achieve optimum patient care at the appropriate time.
Article
In recent years, there has been a movement towards multidisciplinary and patient-focused dental care. A multidisciplinary team (MDT) is a group of individuals from different specialties working closely together and using their expertise to achieve optimum patient care. Joint restorative-orthodontic clinics,1 joint facial deformity clinics and combined cleft care2 have been suggested and developed to facilitate this approach. The suggested advantages in reviewing patients in a multidisciplinary environment include linked treatment provision and a reduction in the number of appointments in the planning stage, all aimed to maximize patient care, clinical provision and efficiency.
The joint paediatric dentistry-orthodontic clinic (CDHCC – Child Dental Health Consultant Clinic) provides access to a MDT, for children and adolescents with paediatric dental and orthodontic problems, enabling each patient to have an allocated time with clinicians of both specialties simultaneously. Formal assessment of the patient can be undertaken, allowing discussion and consultation between the clinicians and patient.
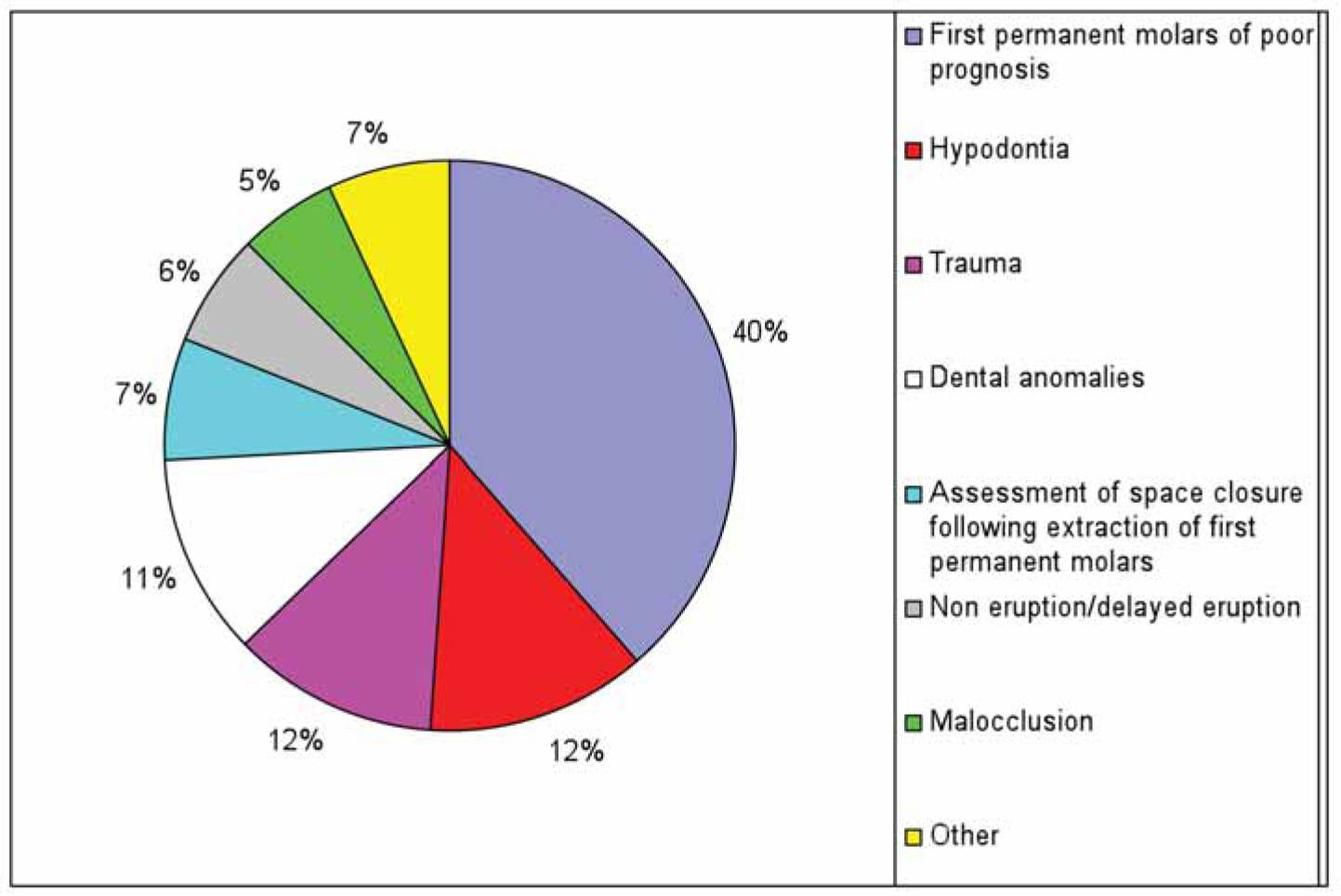
A recent six month survey of referrals to CDHCC of Bristol Dental Hospital from September 2009 to February 2010 demonstrated the range of presenting complaints (Figure 1).
Figure 1. Types of referrals to joint paediatric dentistry-orthodontic clinics at Bristol Dental Hospital.
Cases ranged from the more straightforward consideration of first permanent molars of poor prognosis, where guidelines3 recommend that an orthodontic opinion is sought prior to any decision to extract, to the more complex, such as the consideration of tooth autotransplantation. Most treatment plans were finalized at the first visit to the combined clinic, however, for some patients with complex dental problems, or where growth or dental development needed to be reviewed, subsequent visits were necessary.
Presented in this paper are selections of cases illustrating the range of combined planning in an MDT clinic. Although a number of hypodontia cases have been seen in the MDT clinics, it is not our intention to illustrate them in this paper as their treatment is well reported elsewhere.4,5,6
Management of first permanent molars with poor prognosis
Children can present in the developing dentition with one or more first permanent molars of poor prognosis caused by a variety of aetiological factors, including molar-incisor hypomineralization (MIH), inherited dental anomalies, extensive previous restoration, gross caries, or even apical pathology.
If such teeth are to be restored, technically complicated restorations are required in young children with the potential of increasing dental anxiety and behaviour management problems.7 Such restorations are not ‘forever’ and the elective loss of such teeth must be an option to be considered.
However, the dental literature informs us that extraction of a first permanent molar is rarely the extraction of choice in treating a malocclusion and it has been stated that orthodontic cases involving the extraction of first permanent molars are not only more technically difficult to treat, but will also prolong treatment time.8 It is recommended,3 therefore, that any treatment plan involving the loss of first permanent molars should ideally involve the paediatric dentist and the orthodontist.
The following dental and occlusal factors need to be considered before undertaking such elective extractions:
Underlying malocclusion;
Presence of teeth within the developing dentition, especially the third molars;
Potential timing of the proposed extractions;
Which first molar requires enforced extraction;
The overall condition and long-term prognosis of the other molars.
Underlying malocclusion
In the presence of labial segment crowding, as often seen in Class 1 malocclusions, or Class II div 1 malocclusions, where there is a need to reduce the overjet with or without relief of crowding, little spontaneous relief is provided by first molar extractions. In these circumstances, it may be preferable to restore or temporize the first permanent molars, until the second permanent molars have erupted, and then the extraction spaces can be used for relief of crowding. Therefore, the first molars should be viewed as ‘space maintainers’. The spaces created from the extraction of first molars can subsequently be managed appropriately using fixed appliances.
Presence of teeth within the developing dentition, especially the third molars
Radiographic examination must be carried out prior to extractions to confirm the presence and condition of the successional teeth. If any teeth in the permanent dentition are absent or in a poor eruptive position, this can significantly affect the decision-making process.
Potential timing of the proposed extractions
Early assessment of the long-term prognosis of the affected teeth is essential as timely extraction of the affected molars allows for mesial migration of the second permanent molars, as well as earlier development and better positioning of the third permanent molars.9,10 This timing is especially important in the case of lower first permanent molar extractions in achieving a good occlusion.
The optimum age for the extraction of the molars is between 8 and 10 years, or at the beginning of calcification of the bifurcation of the roots of the lower second permanent molars.11 Earlier extractions, especially of lower permanent first molars, are not recommended because of the risk of the lower second premolar tilting and drifting distally.12 Timing decisions can be delayed and teeth temporarily restored with stainless steel crowns until a more suitable dental age for spontaneous space closure is reached, or until definite treatment of the malocclusion can be undertaken.
Which first molar requires enforced extraction
Generally, if the lower molar is to be extracted, consideration should be given to extracting the upper first molar as well, so as to prevent over-eruption of this tooth (compensating extraction). There is usually no need to compensate for an upper extraction. Guidelines3 also recommend that consideration is given to balancing extractions, ie the removal of the first permanent molar from the opposite side of the same dental arch, however, this is rarely considered unless this tooth is of poor prognosis (see following).
The overall condition and long-term prognosis of the other molars
Although one first molar may be of poor prognosis in isolation, it is not uncommon for others in the same patient to be equally affected with caries or hypoplasia. It is important to assess each individual tooth on its own merits and then, in the context of the patient's individual needs, both from a restorative and overall malocclusion viewpoint.
Very successful treatment plans involving the loss of first molars can be formulated taking into account the patient's social, restorative and orthodontic implications of the extraction decision. The following cases demonstrate the joint approach taken when treating patients with permanent molars of poor prognosis.
Case 1 (MP)
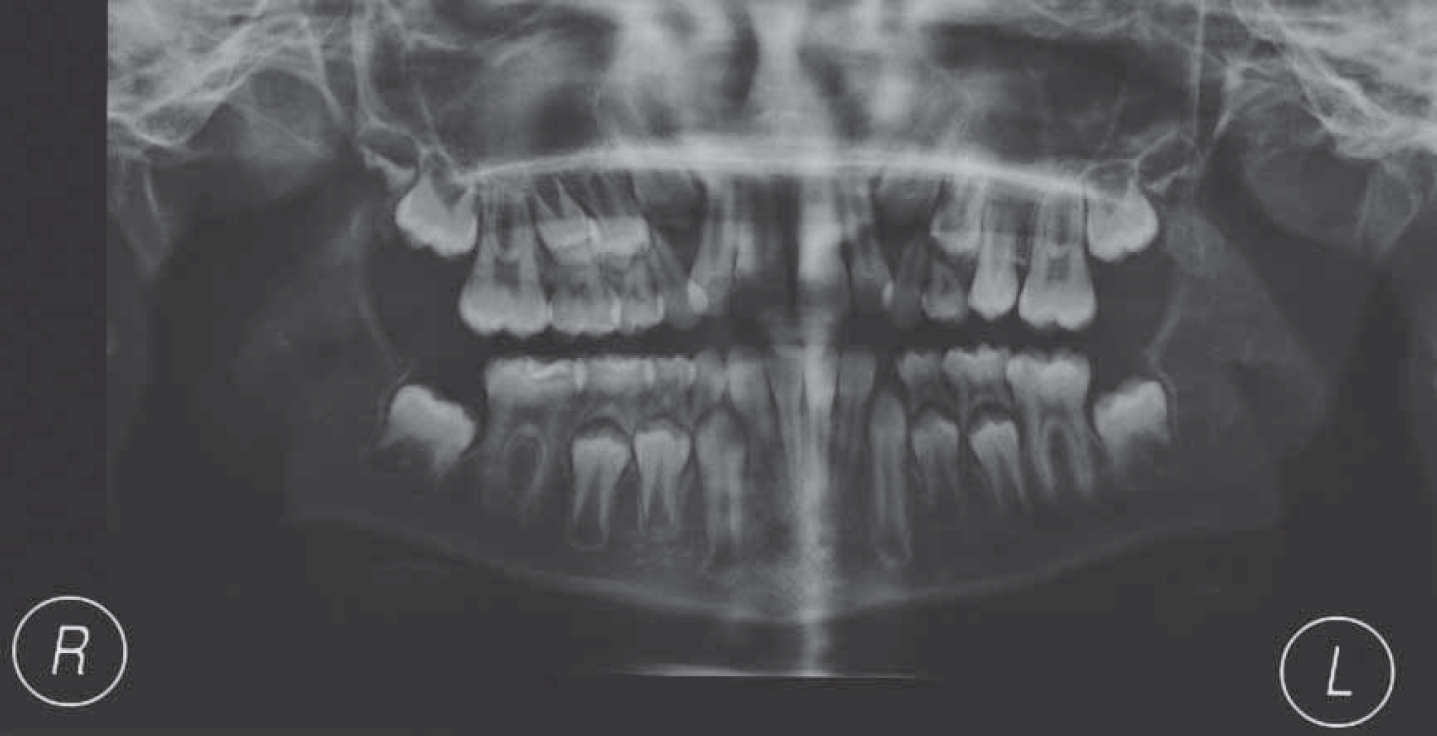
MP was referred to the MDT clinic at 9 years of age regarding MIH. All her first permanent molars were hypomineralized and, in addition, both lower teeth were carious. She had a Class I malocclusion with mild crowding noted in all four quadrants. The DPT (Figure 2) indicated both upper and the lower left third molars were forming and the second permanent molars were showing the development of the furcation – an ideal time to consider the interceptive loss of the 6s. The first permanent molars were removed under general anaesthetic and the patient was followed up over the next 3 years clinically.
Figure 2. DPT of patient MP demonstrating early bifurcation formation of the lower 7s. There is evidence of third molars forming in three quadrants and possibly in the UR quadrant.
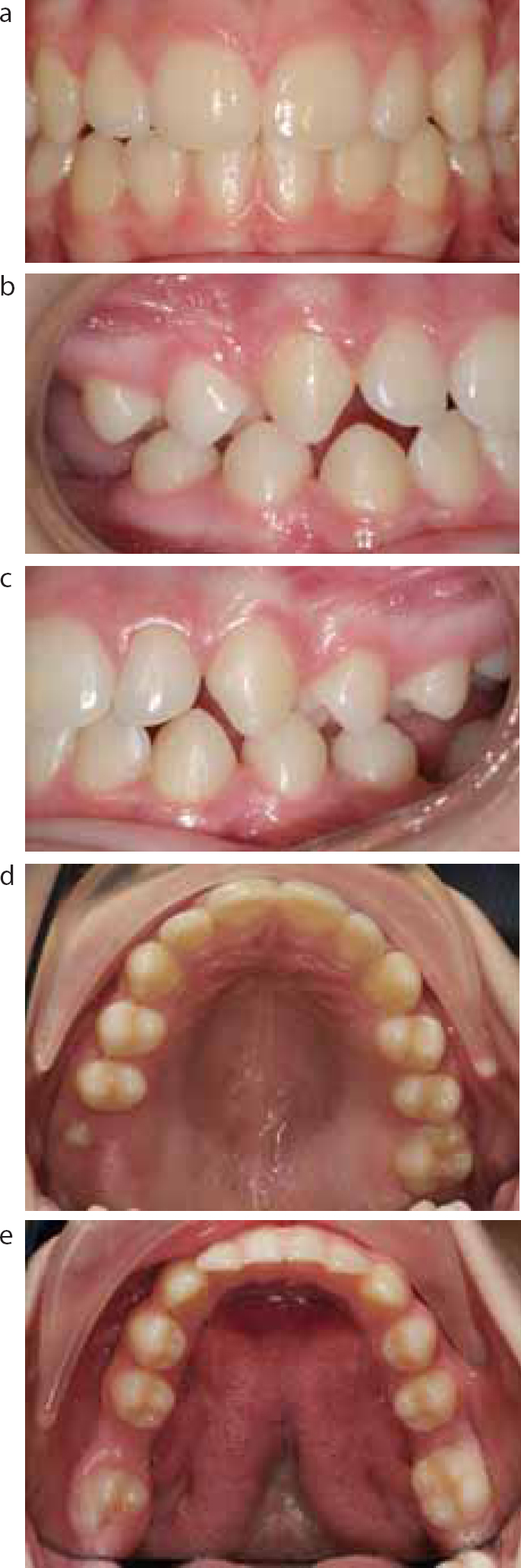
The clinical situation is shown 3 years later, when the patient was 12-years-old (Figure 3 a–e). The second molars have erupted into an excellent position. There is a bilateral posterior crossbite present but no associated displacement and only mild irregularity of the incisors. Once again, the patient was offered further active treatment; understandably, she was happy to accept her malocclusion and no further treatment was undertaken.
Figure 3.
(a-e) Intra-oral photographs of patient MP at 12 years of age, three years after extraction of the first permanent molars.
Case 2 (DR)
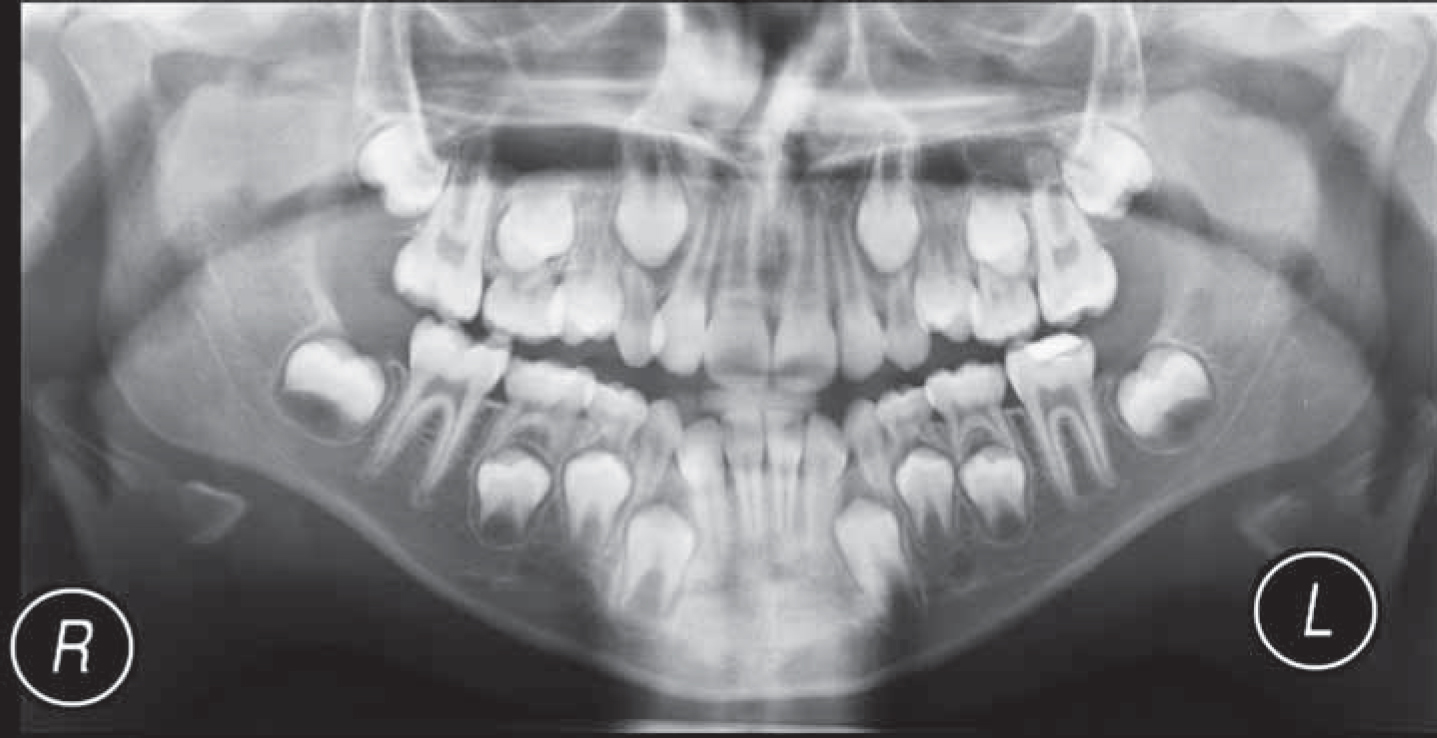
DR was a 10-year-old patient who had been under the care of Bristol Dental Hospital for three years regarding his hypoplastic first permanent molars. He presented with a Class I occlusion on a mild Class II skeletal pattern. The DPT radiograph taken at the time of initial presentation reveals that the bifurcation of the lower second permanent molars is yet to form (Figure 4).
Figure 4. DPT of patient DR on initial presentation showing that the bifurcation of the lower 7s has not yet formed.
The decision was made to maintain the first molars still longer to allow further root formation of the second molars.
A year later, DR presented for review and a new DPT was taken (Figure 5).
Figure 5. DPT of patient DR taken a year later demonstrating the lower second permanent molars at the ideal time to consider loss of the first permanent molars.
Unfortunately, the LR6 had recently been extracted under local anaesthetic due to pain. Because of the further development of the 7s and the presence of the 8s, it was agreed that the loss of the remaining three first molars would now be advisable. These were removed under a general anaesthetic shortly afterwards.
The clinical situation is demonstrated 2 years later (Figure 6a–e). There has been significant, although not complete, space closure in the lower arch and minimal space remaining in the upper arch. Further treatment to close the residual spacing was discussed but the patient was happy with the appearance of the teeth and no further treatment was undertaken. In light of DR's age, further space close could be expected.
Figure 6.
(a–e) Intra-oral photographs of patient DR on review two years following the removal of the first permanent molars.
These cases illustrate that, with good combined planning, very acceptable occlusal results can be achieved with correctly timed extractions of first molars.
Case 3 (TH)
TH was a fit and healthy 10-year-old female referred by her general dental practitioner to the orthodontic department of Bristol Dental Hospital regarding a carious upper right first permanent molar. On examination, she presented with a Class I malocclusion on a Class I skeletal base with average lower anterior face height and competent lips. She had severe upper and lower arch crowding with a bilateral buccal crossbite. The lower right first permanent molar and the upper left first premolar were also carious and the upper left second premolar was hypoplastic.
TH was subsequently assessed on the CDHCC. Although it was thought that, in the long-term, she would require the loss of both upper and lower right permanent molars, in the short term it was decided to restore and maintain them until the upper second permanent molars had erupted (Figures 7a–e and 8).
Figure 7.
(a–e) Pre-treatment intra-oral photographs of patient TH.Figure 8. Pre-treatment DPT of patient TH.
As she was keen to proceed with orthodontic treatment, it was decided to arrange the extractions of both upper first permanent molars and first premolars, the lower right first permanent molar and the lower left first premolar, prior to treatment, with upper and lower fixed appliances together with a lingual arch (Figure 9a–e).
Figure 9.
(a–e) Post-treatment intra-oral views of TH.
Case 4 (TC)
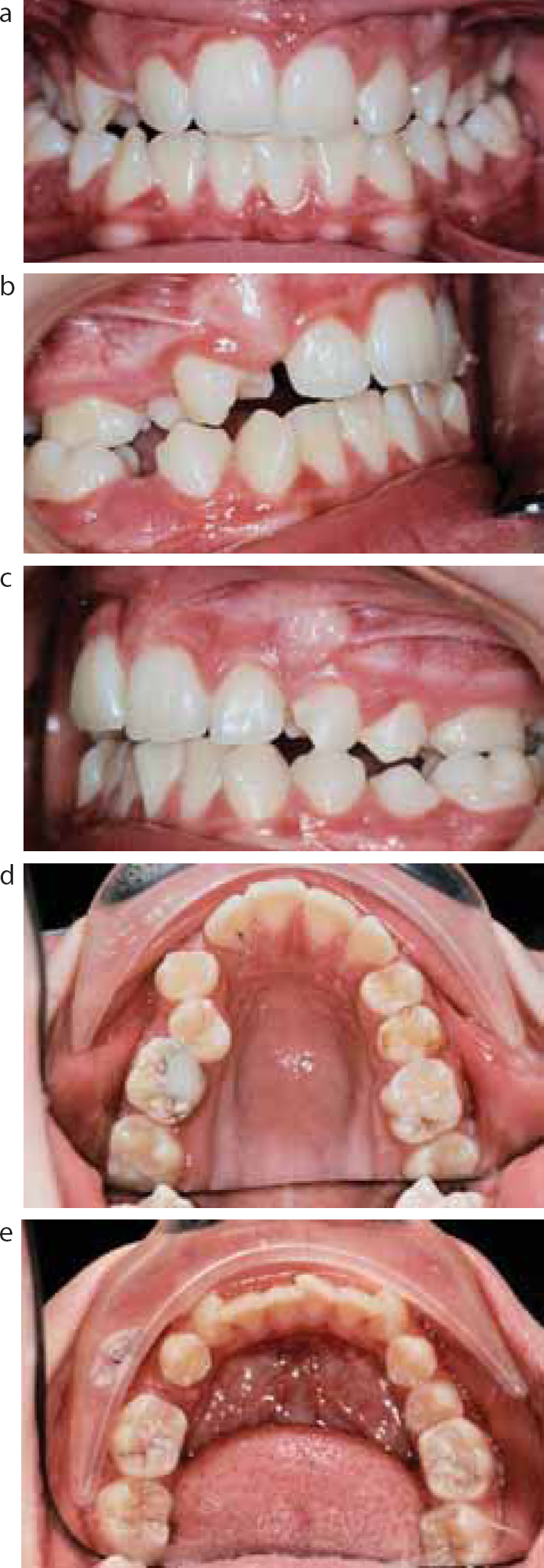
TC was a fit and healthy 7-year-old female referred to the paediatric dentistry department of Bristol Dental Hospital by her general dental practitioner, regarding discoloured lower first permanent molars. Concern was raised about their long-term prognosis. Both lower first permanent molars, the upper left first permanent molar and lower left central incisor had yellow/brown discoloration. The upper central incisor edges also demonstrated a slightly yellow appearance. A clinical diagnosis of molar incisor hypomineralization (MIH) was made and, following discussions in the CDHCC around the very considerable degree of crowding present, it was decided to restore and retain the lower first permanent molars until the bifurcation of the lower second permanent molars had formed before a decision regarding their extraction was to be made (Figures 10a–e and 11).
Figure 10.
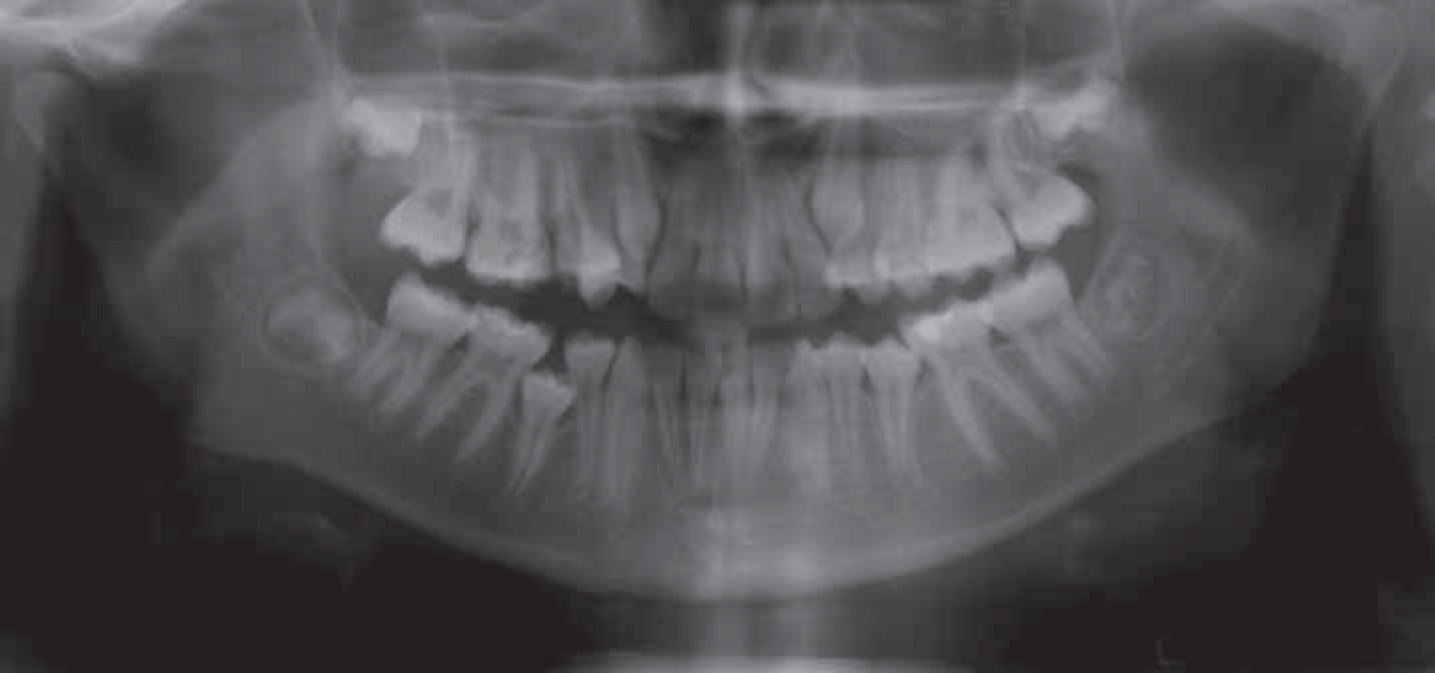
(a–e) Pre-orthodontic treatment intra-oral photographs of patient TC.Figure 11. Pre-orthodontic treatment DPT of patient TC.
Following this treatment, the patient failed to attend any follow-up appointments until she was 12 years of age. At this stage, TC presented with a Class II div 1 malocclusion on a mild Class II skeletal base with increased lower anterior face height and mildly incompetent lips. Severe lower and upper arch crowding had developed, with all four second premolars impacted and unerupted. As TC was keen to proceed with orthodontic treatment, it was decided to incorporate the removal of the lower first permanent molars along with the upper second premolars in the orthodontic treatment.
This demonstrates the space maintenance capacity of the first molars. Early removal of these dysplastic teeth could have resulted in space loss in the lower arch and the need for the removal of further teeth to permit alignment. An argument could have been made to remove the upper first molars instead of the second premolar, however, the upper first permanent molars were healthy and caries free and the upper second premolars were severely crowded and palatally impacted. Their alignment may have prolonged the treatment.
These cases illustrate the potential for paediatric restorative intervention to optimize orthodontic planning choices. In Case 4, the decision was made to delay the extraction of the lower 6s and to restore them in order to enable them to act as ‘space maintainers’ until definitive orthodontic treatment was possible. This involves a degree of ‘crystal-ball’ gazing, to estimate the amount of potential crowding at an early age. In mild cases, the timing of extraction of 6s could be earlier to encourage the potential for spontaneous space closure.
In many early presentations, the correct timing of the extraction of first permanent molars can result in a dental arch which is very acceptable to the patient and, hence, requires no appliance treatment.
Traumatized anterior teeth
The Child Dental Health Survey of 2003 reported that 11% of the 12-year-old and 13% of the 15-year-old children in the United Kingdom had evidence of visible trauma to their permanent central incisors.13 Out of all the dental injuries, crown fractures were the most common injury seen in children and more so in boys. Immediate management of a crown fracture in a young child aims to preserve pulp vitality to allow completion of root development. The overall risk of pulp necrosis, irrespective of the extent of the crown fracture, is low, however, if there are concomitant luxation injuries, the risk is higher.14 One of the most severe forms of dental trauma is an avulsion injury. Avulsion injuries constitute 0.5–3% of the dental injuries in the permanent dentition.15 Although uncommon in a growing child, missing or failing anterior teeth as a result of dental trauma can have social, psychological and financial implications.
A specialist interdisciplinary team with a holistic approach is essential for management of the dental injury threatening tooth loss. Treatment planning on the joint clinic aims to ensure that bone and soft tissue are preserved so that future options are not compromised. Decision-making in young children takes into account the patient's:
Choice;
Age;
Occlusion;
Oral hygiene;
Medical history;
Caries status; and
Growth potential.
Possible options for the management of these cases are illustrated in Table 1.
Short term
Removable appliance with a prosthetic tooth Allow the space to close
Medium term
Orthodontic space closure and restorative treatment of the adjacent teeth Orthodontic space opening/redistribution and restorative treatment Resin-bonded bridge or a fixed bridge Autotransplantation
Long term (following completion of growth)
Implant (+/- orthodontic space distribution)
Implants are contra-indicated in growing children, as placement of implants prior to completion of facial growth will lead to infra-occlusion of the implant relative to the adjacent teeth. It is therefore advisable to postpone implant treatment until facial growth has completed.15
The following case studies demonstrate how combined case planning can lead to good end results, even in cases where significant dental trauma has occurred.
Case 5 (SW)
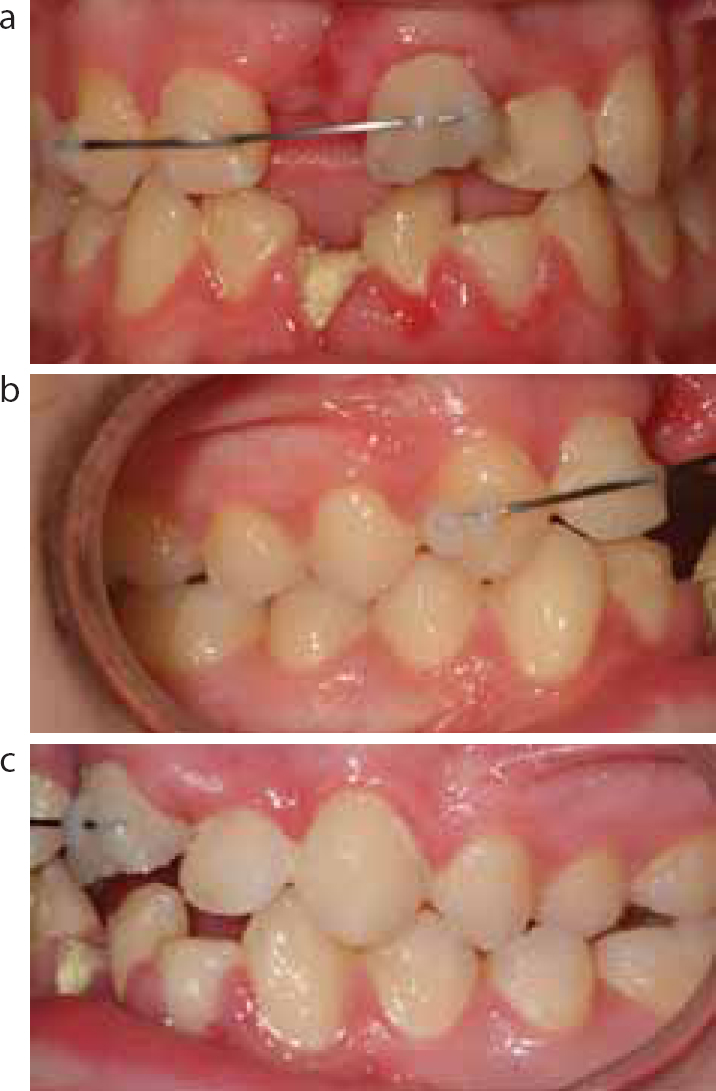
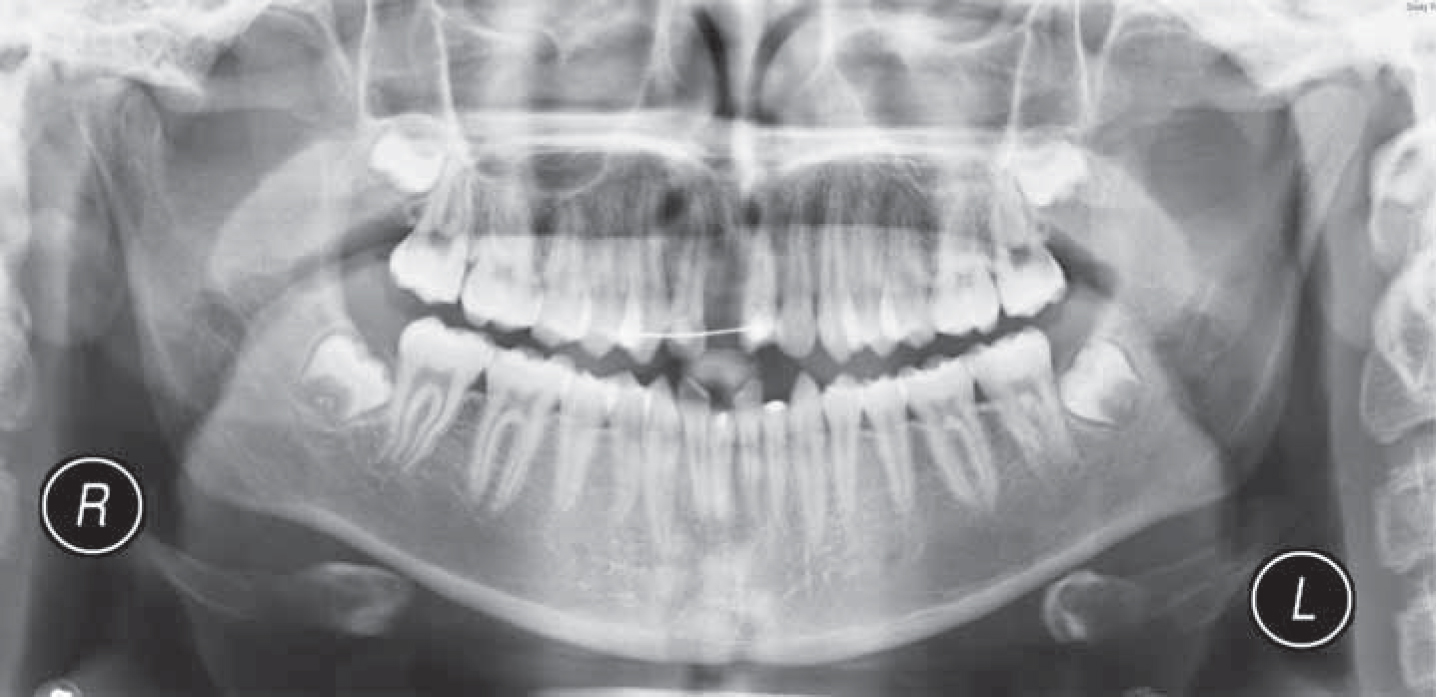
SW was a healthy 15-year-old male, referred by his general dental practitioner for treatment of dental injuries which he had suffered during a bicycle accident. The injury had occurred 3 weeks prior to presentation at Bristol Dental Hospital. He had avulsed the upper right central incisor (UR1) and the tooth had not been re-implanted. The upper left and lower right central incisors had suffered complicated crown fractures, with the lower right central incisor having fractured at the gingival level. A temporary splint had been used to stabilize the UL1. The lower left incisors and the lower right lateral incisor had uncomplicated crown fractures. Prior to the trauma, he had a Class I incisor relationship with a posterior crossbite on the left side and moderate crowding in the upper and lower labial segments (Figures 12a–c and 13).
Figure 12.
(a–c) Intra-oral photographs of patient SW three weeks post trauma on presentation to the paediatric dentistry department. The upper right central incisor has been avulsed. Upper left and lower right central incisors had sustained complicated crown fractures. The lower left and lower right lateral incisors had uncomplicated crown fractures.Figure 13. DPT of SW three weeks post-trauma.
Immediate management of this case included prosthetic replacement of the UR1, extirpation of the pulp from the non-vital upper left and lower right central incisors and application of a protective dressing to the teeth with uncomplicated crown fractures. SW was then referred to the joint paediatric-orthodontic clinic to decide future treatment needs and the long-term options for his developing dentition in the light of the substantially fractured lower incisor and the avulsed upper incisor (Figure 14a–d).
Figure 14.
(a–d) Intra-oral photographs of patient SW on presentation to the joint paediatric dentistry-orthodontic clinic.
The treatment options discussed on the joint clinic included:
Accepting the space in the upper right central incisor region and its restoration with a prosthetic tooth, together with attempts at restoration of the lower teeth.
Extraction of the lower right central incisor followed by upper and lower fixed appliance treatment to close all the spaces present and align the arches. This would result in the acceptance of the upper arch with three incisors and possible composite build-up of the lateral incisors.
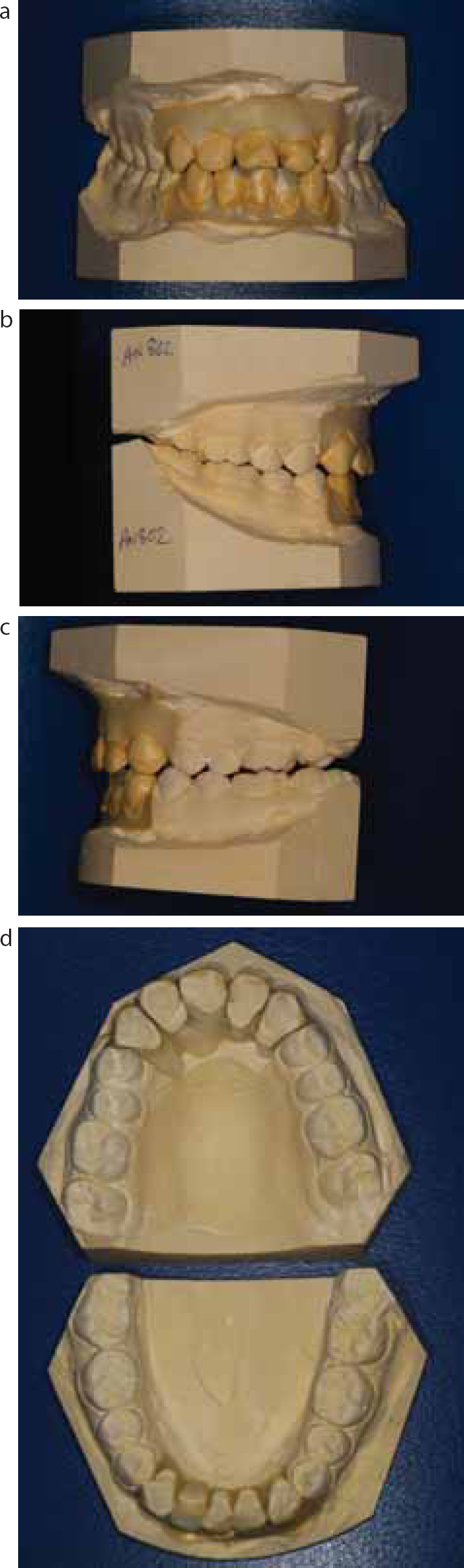
A diagnostic set-up of both options was undertaken and shown to the patient and his family (Figure 15 a–d). They were happy to go ahead with option 2.
SW underwent upper and lower fixed appliance treatment to close and re-distribute the space in the upper arch. It was planned to leave small spaces distal to the upper lateral incisors to facilitate the build-up of these teeth post-treatment. Unfortunately, early in treatment it became evident that the LL1 had suffered mid-third root fracture in the initial trauma, infection persisted and could not be resolved and this tooth had to be extracted (Figure 16 a–e).
Figure 16.
(a–e) Intra-oral photographs of patient SW following removal of orthodontic appliances.
SW has now completed his restorative work and is wearing vacuumed-formed retainers at night (Figure 17). In the long term, he will still require restorative maintenance, however, with joint planning, the extent of this has been reduced.
Figure 17. Intra-oral photograph of patient SW following restoration of the upper left central incisor.
Autotransplantation
Autotransplantation is the surgical repositioning of teeth within the same patient. When a permanent anterior tooth is lost before the completion of skeletal growth, and donor teeth are available, autotransplantation could be considered. Apart from orthodontic space closure, autotransplantation of teeth appears to be the most biologic approach. Immature teeth with an open apex have a higher chance of success, with the ideal root being 3/4–4/5 complete.16 Hence, the careful assessment of the potential donor tooth, with the aid of a panoramic radiograph in the context of the malocclusion, is essential.
The advantages of autotransplantation are the ability of the transplanted tooth to induce alveolar bone growth, continued eruption of the transplanted tooth and maintenance of gingival margin. Its disadvantages include patient commitment to a lengthy treatment plan involving multiple visits and a surgical procedure, usually carried out under general anaesthesia or sedation, as well as the need for a multidisciplinary team for planning and treatment.17
Selecting a graft is primarily based on the root anatomy and cervical contour.17 The cervical aspect must appear similar to its antimere,18 hence, it is recommended that the graft tooth be selected from the opposite side of the arch. Suitable graft (donor tooth) for the maxillary central incisor can include mandibular or maxillary premolars, teeth which are commonly removed as part of an orthodontic treatment plan. In the maxillary lateral incisor region, only the mandibular first premolars are transplanted.15 Occasionally, pre-surgical orthodontics is required to create space for the graft tooth, both in the mesio-distal and vertical dimension. Czochrowska et al19 conducted a long-term follow-up study of 33 transplanted teeth. A success rate of 90% was reported over a 26-year period.
The following case demonstrates where, with the correct timing of treatment, excellent outcomes can be achieved using autotransplantation of a tooth that would otherwise have been discarded as part of the orthodontic treatment.
Case 6 (HM)
HM was a 10-year-old female with an unremarkable medical history. She was referred to the paediatric department of Bristol Dental Hospital for management of a failing upper right central incisor (UR1). The tooth had been avulsed in the past and had been re-implanted. HM presented in the mixed dentition stage with a Class I malocclusion on a Class 1 skeletal base with moderate upper and lower arch crowding. Clinical and radiographic examinations revealed a non-vital UR1 with internal and external root resorption. The long-term prognosis for this tooth was poor. Following pulp extirpation and placement of calcium hydroxide dressings in the UR1, HM was seen on the joint paediatric dentistry-orthodontic clinic to discuss the long-term options for the failing UR1.
The three options considered on the multidisciplinary clinic were:
Accept the situation and eventually replace the UR1 with a prosthetic tooth;
Consider definitive orthodontic treatment involving loss of upper first premolars, lower left second premolar and the lower right first molar and fixed appliance treatment, then replace the UR1 when lost with a resin-bonded bridge.
Consider definitive orthodontic treatment involving the loss of a unit in each quadrant (as above), transplantation of the lower left premolar into the UR1 space and fixed appliance treatment.
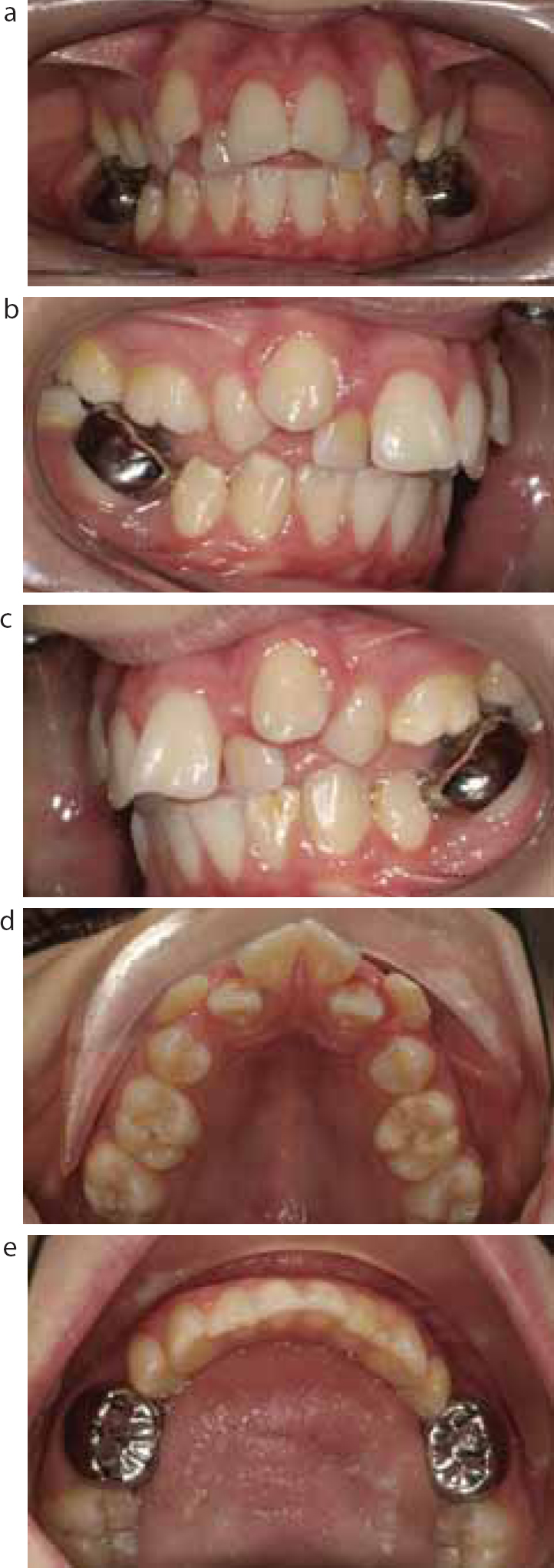
HM wished to have the third option involving upper and lower fixed appliance treatment to align her teeth utilizing autotransplantation (Figures 18a–e and 19).
Figure 18.
(a–e) Pre-treatment intra-oral views of patient HM.Figure 19. Pre-operative DPT of patient HM showing the failing UR1.
Initially, HM was fitted with an upper removable appliance with a flat anterior bite-plane to reduce the overbite prior to the transplant being undertaken. Following the extraction of the UR1, the LL5 was transplanted to the UR1 position under general anaesthesia (Figures 20 and 21).
Figure 20. Patient HM at the time of transplantation of LL5 to UR1 socket.Figure 21. Post-transplantation photograph of patient HM.
Seven weeks after the surgery, an interim composite veneer was placed on the LL5 so that it resembled the extracted UR1 (Figure 22 a–b).
Figure 22.
(a–b) Post-operative composite build-up of LL5.
HM is currently undergoing lower fixed appliance therapy as she is happy with the appearance of the upper teeth and the transplanted LL5 remains vital, with no obvious resorption. Pulp survival and periodontal healing are vital for the success of autotransplantation. Periodontal ligament (PDL) healing can result in regeneration of the PDL or replacement ankylosis (Figure 23).
Figure 23. Two years post autotransplantation DPT of patient HM.
Conclusion
In this article, we have tried to demonstrate the advantages of undertaking combined paediatric dentistry-orthodontic planning in the care of patients with first molars of poor prognosis, either due to caries or hypoplasia and cases with trauma to anterior teeth. These presentations are an all-too-common occurrence in our practices. Working together and viewing the issue from different angles can facilitate excellent outcomes in these young patients.
In the second article of these series we will be discussing some uncommon cases which would equally benefit from a joint approach.