Cousley RRJ Mini-implants in contemporary orthodontics Part 1: recent evidence on factors affecting clinical success. Orthod Update. 2015; 8:6-12
Cousley RRJLondon: Wiley-Blackwell; 2013
Kokich VG It's only a screw. Am J Orthod Dentofacial Orthop. 2012; 142
Al-Sibaie S, Hajeer MY Assessment of changes following en-masse retraction with mini-implants anchorage compared to two-step retraction with conventional anchorage in patients with class II division 1 malocclusion: a randomized controlled trial. Eur J Orthod. 2014; 36:275-283
Sung SJ, Jang GW, Chun YS, Moon YS Effective en-masse retraction design with orthodontic mini-implant anchorage: a finite element analysis. Am J Orthod Dentofacial Orthop. 2010; 137:648-657
Upadhyay M, Yadav S, Nagaraj K, Patil S Treatment effects of mini-implants for en-masse retraction of anterior teeth in bialveolar dental protrusion patients: a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2008; 134:18-29
Upadhyay M, Yadav S, Nanda R Biomechanics of incisor retraction with mini-implant anchorage. J Orthod. 2014; 41:(Suppl)15-23
Kinzinger GSM, Fritz UB, Sander F, Diedrich PR Efficiency of a pendulum appliance for molar distalization related to second and third molar eruption stage. Am J Orthod Dentofacial Orthop. 2004; 125:8-23
Escobar SA, Tellez PA, Moncada CA Distalization of maxillary molars with the bone-supported pendulum: a clinical study. Am J Orthod Dentofacial Orthop. 2007; 131:545-549
Fudalej P, Antoszewska J Are orthodontic distalizers reinforced with the temporary skeletal anchorage devices effective?. Am J Orthod Dentofacial Orthop. 2011; 139:722-729
Gelgor IE, Karaman AI, Buyukyilmaz T Comparison of 2 distalization systems supported by intraosseous screws. Am J Orthod Dentofacial Orthop. 2007; 131:(2)161.e1-161.e8
Kanavakis G, Ludwig B, Rosa M, Zachrisson B, Hourfar J Clinical outcomes of cases with missing lateral incisors treated with the T-Mesialslider. J Orthod. 2014; 41:(Suppl)33-38
Cousley RRJ Molar intrusion in the management of anterior openbite and ‘high angle’ Class II malocclusions. J Orthod. 2014; 41:(Suppl)39-46
Scheffler NR, Proffit WR, Phillips C Outcomes and stability in patients with anterior open bite and long anterior face height treated with temporary anchorage devices and a maxillary intrusion splint. Am J Orthod Dentofac Orthop. 2014; 146:594-602
Hart TR, Cousley RRJ, Fishman LS, Tallents RH Dentoskeletal changes following mini-implant molar intrusion in anterior open bite patients. Angle Orthod. 2104;
Mini-implants in contemporary orthodontics part 2: clinical applications and optimal biomechanics Richard R J Cousley Orthodontic Update 2025 8:2, 56-61.
Authors
Richard R JCousley
BSc, BDS, MSc, FDS RCS, FDS(Orth) RCS
Department of Orthodontics, Peterborough and Stamford Hospitals NHS Foundation Trust, UK
Since it is well established that orthodontic mini-implants provide stable anchorage in all three dimensions, the focus has progressed to understanding the related biomechanics. This paper describes the key biomechanical advances for mini-implant treatments, especially in terms of optimized movement of the target teeth.
Clinical Relevance: An understanding of the optimum insertion sites and biomechanics improves clinical outcomes in orthodontic mini-implant cases.
Article
Richard R J Cousley
When orthodontic mini-implants (OMIs) became readily available in the early years of the new millennium they were initially ‘competing’ with existing osseointegrated fixtures such as restorative (dental) and orthodontic palatal implants. Therefore, the initial body of research work and publications focused on the biological and clinical factors which appeared to affect OMI success (stability) rates and whether this compared favourably with these other bone fixtures. Subsequently, as both clinicians and researchers began to see clear evidence of OMI stability and low morbidity, these fixtures became more widely utilized for anchorage reinforcement. These aspects have been extensively detailed, using the most recent research evidence, in the first paper in this series.1 However, in recent years the focus has broadened to include new clinical applications, ie how may we use mini-implant anchorage optimally.2 A large number of case reports have been published, often documenting impressive results of different types of malocclusions being successfully treated with OMIs. However, as pointed out by the late Dr Vince Kokich,3 some of these reports have strayed into bone anchorage usage at the expense of other clinical options, and this has perhaps caused a distraction from the quality and innovation of the majority of publications. Fortunately, based on a combination of these case reports, and especially from recent systematic reports (in the form of case series and randomized controlled trials), we can see that OMIs provide reliable anchorage. However, anchorage is only one part of the clinical picture, and these studies did not necessarily analyse the nature and range of biomechanical effects on the dentition.
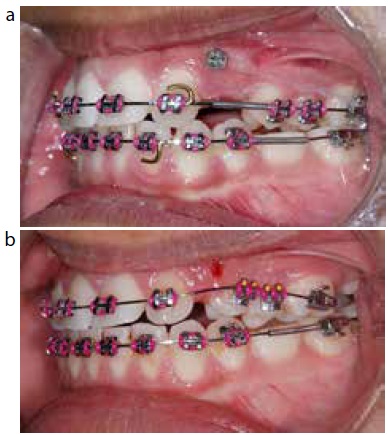
Over a number of years following the introduction of OMI, anchorage orthodontists began to observe clinical side-effects, such as the development of lateral openbites (Figure 1), and realized that this was due to a combination of uncontrolled canine tipping and an unfavourable vertical component of the traction (which isn't overtly expressed with conventional fixed appliance mechanics where the traction runs alongside the archwire). Therefore, it has become apparent that OMIs provide the benefits of enhanced anchorage control, but with the potential for stronger expression of undesirable tooth movements. Consequently, the second phase of OMI clinical innovation and research included a focus on the reduction of such biomechanical side-effects. Furthermore, the clinical observations resulting from customized OMI biomechanics have crucially altered our understanding and expectations of orthodontic tooth movements and treatment outcomes. This paper aims to highlight these new biomechanical approaches, perhaps best exemplified by the addition of powerarms to the OMI armamentarium.
Figure 1. Oblique traction was applied in this hypodontia case to protract the upper molars (a). It resulted in a unit of mesial movement but also ‘rollercoaster’ bowing of the archwire and a lateral openbite (b).
Powerarms (elongated hooks) are now regarded as a key component in OMI treatments since they have enabled direct traction to be applied much more parallel to the occlusal plane during both incisor retraction and molar protraction treatments (Figure 2). This has eliminated the use of oblique vectors of traction and hence reduced any vertical intrusive side-effects. It has also, perhaps inadvertently, paved the way for the next advance in OMI direct anchorage techniques. This centres on the ‘receiving end’ of the traction and possibilities for enhanced control of the target teeth. This review paper will describe current biomechanical approaches based on this latest awareness and the shift from maximum anchorage-focused goals to include maximized treatment effects on the target teeth. Since it is now possible to control anchorage, and hence tooth movements, in all three dimensions (3D), OMI applications are best discussed in each of the three planes of space: antero-posterior, transverse and vertical. Furthermore, OMI treatments may be subdivided within these 3D categories according to the principal treatment objective for the most common orthodontic treatment plans (Table 1). This paper will describe these subgroup topics within the context of these 3D clinical applications.
Figure 2. Traction applied to a ‘shepherd’s crook' type of powerarm in this Class II division 1 case. This makes the force vector almost parallel to the occlusal plane and applied closer to the centre of resistance of the anterior teeth (than a standard archwire hook).
Dimension
Clinical applications
Antero-posterior
Anterior tooth retraction and torque
Molar distalization
Molar protraction
Transverse
Centreline correction
Occlusal plane levelling
Bone anchored palatal expansion
Vertical
Incisor intrusion
Molar intrusion
Tooth extrusion
Clinical applications in 3D
Antero-posterior anchorage
Bodily incisor retraction and torque control
Orthodontists will be most familiar with the classical use of orthodontic anchorage reinforcement to prevent mesial movement (anchorage loss) of the maxillary molar teeth. Such reliable anchorage is readily accomplished with OMIs, using either direct or indirect anchorage. Indirect anchorage involves using OMI(s) to stabilize the anchor tooth/teeth, such as when the maxillary first molar is anchored by a wire connection to mid-palatal OMI(s) (Figure 3). Orthodontic traction, eg a closing coil spring, is then attached between the molar hook (on the anchor unit) and the anterior (target) teeth or archwire hook. However, there is a risk of anchorage loss due to wire distortion or failure of the molar attachment. Indirect anchorage also relies on conventional fixed appliance traction mechanics and therefore entails its limitations, such as the risk of incisor retroclination (controlled tipping), rather than providing scope for true bodily incisor retraction. This is only feasible with direct traction between an OMI and powerarm.
Figure 3. Indirect anchorage of the maxillary first molars, involving a rigid transpalatal arch between the molars and a mid-palatal implant.
Direct anchorage for incisor movements is typically achieved using an OMI inserted transmucosally on the buccal side of the alveolus, between the first molar and second premolar roots. Direct anchorage provides both stable anchorage (the avoidance of mesial movement of the adjacent molars since no traction is applied to these teeth) and enhanced control of incisor teeth movements. Interestingly, this additional torque control is classically more anchorage demanding than conventional traction, which tends to retrocline and tip teeth. The improved biomechanical control occurs because the powerarm's long length applies the traction closer to the centre of resistance of the target teeth (than with a conventional short hook). Powerarms are usually crimped onto a rigid (eg 0.019” x 0.025”) stainless steel archwire (Figure 2), but they may also be bonded directly onto either the labial or palatal surface of an individual target tooth (Figure 4). Several designs of crimpable powerarms are currently available: the original ‘shepherd’s crook' (Figure 2) and the more recently introduced sigmoid version (Figure 5). The author has found that the latter one is more adaptable in terms of the level of traction and the ease with which it may be contoured between the lip and gingival soft tissue zones. Both of these powerarm designs provides better torque control as the incisors are less prone to retroclination (lingual tipping of their crowns) during their retraction.4,5,6,7 In turn, this ensures that the combination of the planned antero-posterior tooth movements and an optimal aesthetic result may be achieved, even in adult ‘camouflage’ patients (Figure 6). However, given the amount of palatal movement of the upper incisor roots which may now be achieved, it's particularly important to confirm the anterior palatal alveolar width on a lateral cephalogram prior to treatment. If this is limited, eg where the anterior palate has been moulded by a digit habit, then the planned amount of incisor root retraction should be reduced to avoid an increased risk of incisor root resorption, due to contact with the palatal cortical plate.
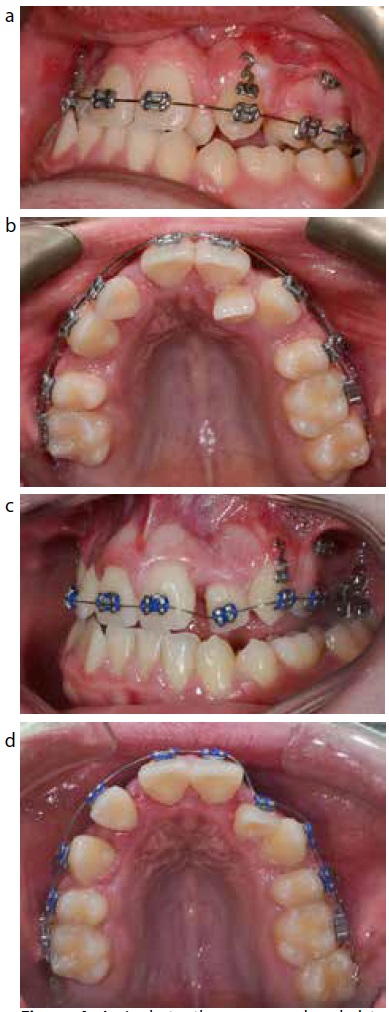
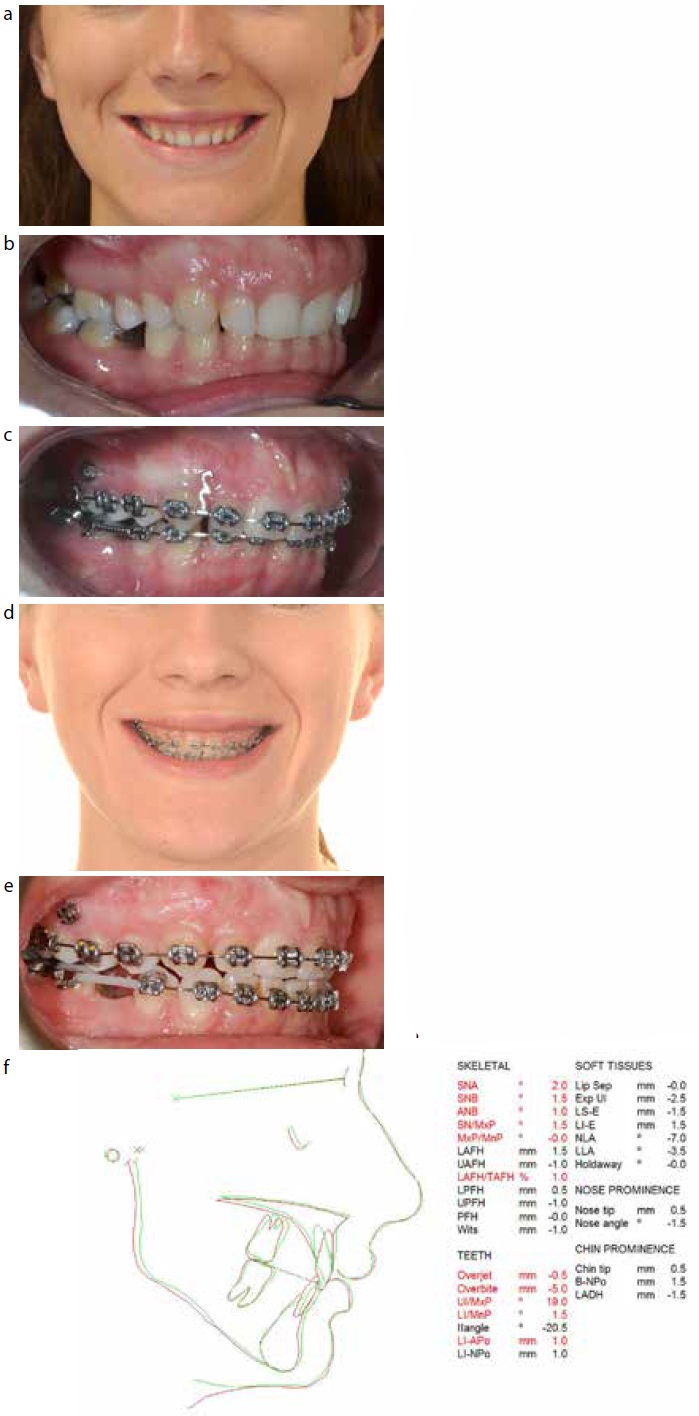
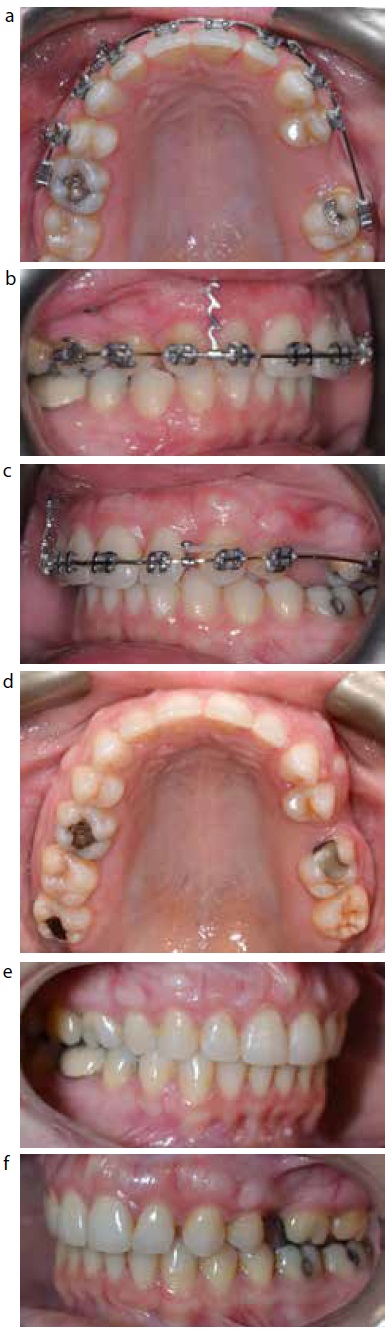
Figure 4. A single-tooth powerarm, bonded to the upper left canine crown. Direct traction was used to distalize the canine in a bodily manner (a, b) prior to alignment of the adjacent lateral incisor tooth (c, d).Figure 5. Traction applied to a sigmoid-shaped powerarm later during treatment in the patient shown in Figure 2. This powerarm has been more easily contoured in a neutral zone between the adjacent mucosa and lip tissue. Its increased length also made the force vector parallel to the occlusal plane and closer to the centre of resistance of the anterior teeth.Figure 6. An adult patient with a Class II division 2 malocclusion featuring increased upper incisor/gingival display (a) and lower premolar hypodontia (b). The arches have been aligned prior to placement of maxillary OMIs and powerarms (c). The upper incisors have been intruded and retracted, as well as lower incisors proclined (d, e). Cephalometric superimposition (f) of the alignment and traction phases demonstrates upper incisor intrusion and torque, plus mild upper molar intrusion.
Bodily molar movements
Conventional fixed appliance biomechanics for molar distalization is typically applied at the coronal level. However, this tends to tip the molar teeth because the force is applied at some distance coronal to the molar's centre of resistance (furcation point). This tipping effect on the first molar is exacerbated if it is not counteracted by contact with an adjacent fully erupted second molar crown, although in turn the second molar then tends to tip distally.8 All of the so-called ‘non-compliance’ distalizers also inevitably suffer anchorage loss, both during molar distalization and then during retraction of the anterior teeth, unless they have been bone anchored.9,10 Fortunately, the use of mini-implants now provides the required combination of effective anchorage and better control of bodily tooth movements when molar teeth are being distalized or protracted (mesialized).
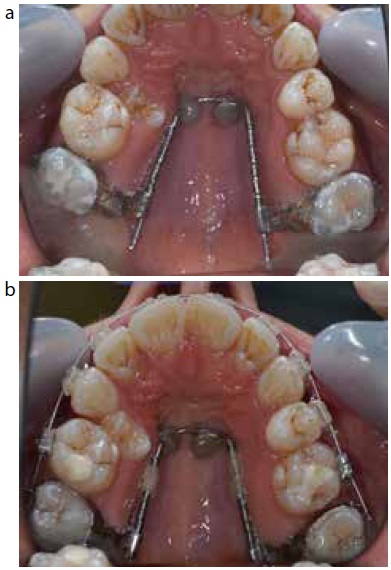
Alveolar insertion sites provide limited scope for such antero-posterior molar movements, especially when molar distalization needs to be followed by a second phase of premolar and anterior tooth retraction. Therefore, maxillary molar distalization, especially involving half a unit or more of molar movement, is best achieved with OMIs inserted in the mid-palate area, since there is no potential root interference (Figure 7). This also facilitates application of the distalizing force at the furcation level and hence better bodily molar movement.2,11 Whilst this indirect anchorage is more technically demanding, in terms of distalizer appliance design, fabrication and insertion, such distalizers tend to be easy to re-activate during molar distalization. This typically involves re-compression of the pushcoil (active component) to ensure continuous force application.
Figure 7. A palatal distalizer in an adult patient, anchored on two paramedian OMIs and where the pushcoil pressure is applied to the molar furcation levels (a). Spaces have been opened in the buccal segments, and the pushcoil recompressed with composite stops, prior to bonding of a fixed appliance (b).
Similarly, mid-palatal anchorage may be used for molar protraction, where the posterior teeth need to be moved mesially to close spaces due to either hypodontia or premature tooth losses. This involves a similar combination of midpalatal anchorage and a U-shaped base wire, but with traction applied from the frame to the molar(s). Alternatively, direct anchorage may be utilized when premolar mesialization is not required in the maxillary arch and for any form of molar protraction in the mandibular arch. This involves the application of traction from an OMI, ideally inserted mesial or distal to the first premolar, to a molar powerarm (Figure 8). Such molar protraction can obviate the need for long-term restorative pontic provision and it should be considered as a treatment option where there is sufficient alveolar bone for orthodontic space closure.12 However, in the author's experience, the greater the alveolar deficiency then the greater the potential for side-effects such as mesial tipping of the molar and subsequent binding of the archwire in the molar tube. This leads to mesial shunting of the entire arch and manifests as advancement and intrusion of the anterior teeth, although these side-effects can be counteracted with the use of conventional intra-arch traction (Figure 8).
Figure 8. Pre-treatment panoramic radiograph showing ectopic lower canines and impacted lower second molars (a). OMIs could only be sited in the canine regions, then traction applied via powerarms to protract the molars (b). Sufficient mesial movement of the buccal segments has been achieved, although lower incisor proclination has also occurred. The OMIs were then removed and standard space closure undertaken (c-e) to achieve a Class I incisor relationship (f, g).
Transverse anchorage
Some patients present with a large asymmetrical displacement of the dental centreline, due to either the unilateral absence of teeth or an underlying transverse skeletal asymmetry. Correction of this centreline discrepancy requires anchorage reinforcement on the contralateral side to the centreline displacement. Unfortunately, conventional anchorage, such as a transpalatal arch or headgear, connects the anchor teeth on both sides of the arch even when this anchorage on the side of the centreline shift is at best unwarranted and may even be contra-indicated for tooth movements on this side (such as molar protraction). In contrast, OMIs provide the benefit of effective unilateral anchorage specifically applied to the target side (Figure 9). Unilateral anchorage is also beneficial for correction of vertical asymmetry where the patient has an occlusal plane cant, ie the occlusal plane is tilted (relative to the face) with one side at a lower vertical level than the other side. Fortunately, it is now possible to correct both centreline displacements and many vertical occlusal plane cants using mini-implant anchorage. Such vertical anchorage is best exemplified in the context of molar intrusion, as described in the next section.
Figure 9. An adult patient with absent upper left second premolar and first molar teeth, requiring movement of the upper centreline to the right side as well as left molar protraction (a). OMI-powerarm traction was used on the right side and conventional traction (anchorage loss) on the left side (b, c), to achieve the desired tooth movements (d–f), which would normally be mutually exclusive.
Vertical anchorage
It is now recognized that skeletal anchorage has caused a paradigm shift in the management of patients with excessive vertical growth discrepancies, especially those with anterior open-bite (AOB).13,14 This is especially the case for patients with Class I and Class II malocclusions, where closure of the AOB is typically accompanied by Class II improvements such as an overjet reduction (Figure 10).13 Conversely, this may worsen the antero-posterior and facial profile discrepancies in patients with Class III and bimaxillary incisor proclination features. These cases are best treated using conventional options, involving either premolar extractions (with subsequent incisor teeth retraction during space closure), or orthognathic surgery (typically a maxillary osteotomy with vertical impaction and possibly advancement movements). Patients with a significant anterior vertical facial excess, presenting as a ‘gummy smile’, and gross lip incompetence, are also still more appropriately treated with a maxillary impaction osteotomy since the surgical approach is currently more effective at achieving a large reduction in the anterior mid-facial length.
Figure 10. An adult patient with a Class II division I malocclusion, on a skeletal II base with increased vertical proportions and increased upper incisor display (a–c). Expansion and intrusion of the maxillary molars has resulted in anterior bite closure and premature canine contacts, prior to bonding of upper fixed brackets (d, e). The AOB has been corrected with improvements in the smile aesthetics and Class II profile at debond (f, g). The occlusal corrections were stable 15 months later despite poor retainer compliance (h).
Whilst OMI-assisted intrusion of the maxillary molars may represent more ‘effort’ for the orthodontist, from the patient's perspective it's a minimally invasive treatment compared to dental extractions and orthognathic surgery. Although some authors advocate OMI placement on the buccal side of the maxillary alveolus14 or in mid-palatal sites, this author has found that palatal alveolar sites are ideal for posterior vertical anchorage purposes. In particular, the posterior palatal alveolus offers sufficient interproximal root clearance, a suitable soft tissue environment, reliable cortical bone support, and adequate distance between the OMI and intruding teeth.13 In addition, the insertion of OMIs distal (rather than mesial) to the upper first molar teeth enables direct intrusion of the first molars and makes it simple to apply direct traction to the second molar teeth. The latter is beneficial when the terminal molars require additional intrusion (especially of the palatal cusps) or torque control (Figure 11). The potential negative side-effect is that palatal traction risks causing arch constriction because the anchorage point is medial to the molar crown and its fulcrum point. However, this is readily countered by a customized rigid TPA or quadhelix expander (Figure 10).2,13 These are all technique findings based on clinical observations. More formal research findings are becoming available, initially in the form of retrospective research. For example, a recent study of 31 maxillary molar intrusion cases has indicated that adolescent patients have greater scope for favourable mandibular skeletal improvements following molar intrusion than adults,15 but ideally this requires a prospective study as future evidence. In addition, there is still a need for long-term research results, since AOB correction is classically one of the most prone malocclusion traits to relapse.
Figure 11. Buttons have been bonded to the palatal aspect of the maxillary second molars to enable direct intrusion/torque of these teeth, using elastomeric traction.
Conclusions
Orthodontic mini-implants provide several advantages over and above those available with conventional anchorage reinforcement. On the one hand the resultant anchorage is reliable, minimally invasive, largely independent of patient compliance, and feasible in all three dimensions, while at the same time, it's now possible to produce more consistent bodily movements of the target teeth than with conventional biomechanics, because correct biomechanical designs mean that the forces are applied close to the centres of resistance of the target teeth. This is achieved with the use of powerarms in direct anchorage scenarios, and the positioning of palatal appliances near the level of the molar furcations in indirect anchorage cases.