Mitchell L Decalcification during orthodontic treatment with fixed appliances - an overview. Br J Orthod. 1992; 19:199-205
Gorelick L, Geiger A, Gwinnett J Incidence of white spot formation after bonding and banding. Am J Orthod. 1982; 81:93-98
Machen DE Oral hygiene assessment: plaque accumulation, gingival inflammation, decalcification, and caries: legal aspects of orthodontic practice: risk management concepts. Am J Orthod Dentofacial Orthop. 1991; 100:93-94
Zimmer BW, Rottwinkel Y Assessing patient-specific decalcification risk in fixed orthodontic treatment and its impact on prophylactic procedures. Am J Orthod Dentofacial Orthop. 2004; 126:318-324
Le PT, Weinstein M, Borislow AJ, Braitman LE Bond failure and decalcification: a comparison of a cynoacrylate and a composite resin bonding system in vivo. Am J Orthod Dentofacial Orthop. 2003; 123:624-627
Kanthathas K, Willmot DR, Benson PE Differentiation of developmental and post-orthodontic white lesions using image analysis. Eur J Orthod. 2005; 27:167-172
Zachrisson BU, Arthun J Enamel surface appearance after various debonding techniques. Am J Orthod. 1979; 75:121-137
Diedrich P Enamel alterations from bracket bonding and debonding: a study with scanning electron microscope. Am J Orthod. 1981; 79:501-522
Steffen MJ The effects of soft drinks on etched and sealed enamel. Angle Orthod. 1996; 66:449-456
Dincer B, Hazar S, Sen BH Scanning electron microscope study of the effects of soft drinks on etched and sealed enamel. Am J Orthod Dentofacial Orthop. 2002; 122:135-141
Sadowsky PL, Retief DH, Bradley EL Enamel fluoride uptake from orthodontic cements and its effects on demineralization. Am J Orthod. 1981; 79:523-534
Summers A, Kao E, Gilmore J, Gunel E, Ngan P Comparison of bond strength between a conventional resin adhesive and resin-modified glass ionomer adhesive: an in vitro and in vivo study. Am J Orthod Dentofacial Orthop. 2004; 126:200-206
Tufekci E, Merrili TE, Pintado MR, Beyer JP, Brantley WA Enamel loss associated with orthodontic adhesive removal on teeth with white spot lesions: an in vitro study. Am J Orthod Dentofacial Orthop. 2004; 125:733-740
Vorhies AB, Donly KJ, Staley RN, Wefel JS Enamel demineralization adjacent to orthodontic brackets bonded with hybrid glass ionomer cements: an in vitro study. Am J Orthod Dentofacial Orthop. 1998; 114:668-674
Wilson RM, Donly KJ Demineralization around orthodontic brackets bonded with resin modified glass ionomer cement and fluoride-releasing resin composite. Pediatr Dent. 2001; 23:255-259
O'Reilly M, Featherstone J Demineralization and remineralization around orthodontic appliances: an in vivo study. Am J Orthod Dentofacial Orthop. 1987; 92:33-40
Gorton J, Featherstone JD In vivo inhibition of demineralization around orthodontic brackets. Am J Orthod Dentofacial Orthop. 2003; 123:10-14
Pascotto RC, Navarro MF, Filho LC, Cury JA In vitro effect of resin-modified glass ionomer cement on enamel demineralization around orthodontic brackets. Am J Orthod Dentofacial Orthop. 2004; 125:36-41
Methods used to determine demineralization of enamel associated with orthodontic treatment: a review Harshavardhan Kidiyoor Roopak D Naik Orthodontic Update 2025 4:4, 107-111.
Authors
HarshavardhanKidiyoor
BDS, MDS
Reader, Department of Orthodontics and Dentofacial Orthopaedics
Professor and Head, Department of Orthodontics and Dentofacial Orthopaedics, SDM College of Dental Sciences and Hospital, Sattur, Dharwad – 580 009 Karnataka, India
Demineralization/decalcification of the enamel around orthodontic brackets, seen clinically as white spot lesions, remain a sometimes neglected part of orthodontic care. Even though there are numerous studies on decalcification, most of them are based on subjective evaluation of enamel samples. The various techniques used to determine enamel demineralization associated with orthodontic treatment have not been directly compared and the operator is left with limited choice. Since these techniques have their own limitations, the selection of a protocol for the study of demineralization of enamel should be based on the true merit of the technique and its relevance to the study. Hence, the various methods used to determine demineralization of enamel during orthodontic treatment have been critically evaluated and their application in clinical orthodontics and research discussed.
Clinical Relevance: Dental enamel has very limited regenerative capacity; hence prevention of its demineralization is of prime concern to a dentist in general and to an orthodontist specifically. The appearance of white spots/damage to healthy enamel after orthodontic treatment is both unaesthetic and legally questionable. Further, there is a lack of correlation among the various methods suggested to evaluate enamel demineralization. The current article not only summarizes the various methods but also suggests relevant steps to prevent the demineralization of enamel.
Article
Decalcification is defined as loss of calcified tooth substance. It occurs when the pH of the oral environment favours the diffusion of calcium and phosphate ions out of enamel.1 The clinical appearance of a white spot lesion (Figure 1) is caused by an optical phenomenon due to subsurface tissue loss and is exaggerated by thorough drying.2 Preventing this decalcification that may occur during orthodontic treatment is of importance because these lesions are unaesthetic, potentially irreversible and cariogenic. From a legal standpoint, DE Machen, an orthodontist and an expert in dental jurisprudence, has stated that the responsibility of assessment, notification and prevention of any decalcification, which occurs during orthodontic treatment, lies with the practitioner.3
Figure 1. White spot lesions in an orthodontic patient.
Studies on enamel evaluation during/after orthodontic treatment have shown varying degrees of demineralization. The various methods used for evaluation of demineralization of enamel are as follows:
Direct examination;
Photographic examination;
Stereomicroscopy;
Scanning electron microscopy;
Stylus profilometer;
Polarized light microscopy;
Microradiography;
Cross-sectional microhardness.
These methods could be used for qualitative or quantitative evaluation of the enamel. The samples of enamel used in the study can be from routine clinical cases (in vivo) or from experimental set-up (in vitro) specifically meant to simulate certain parameters. However, direct comparison between these studies is not possible as each method examines enamel in its own way and most of the conclusions are from subjective evaluation of the samples. Hence, each method will be discussed separately with a brief review of available literature.
Direct examination
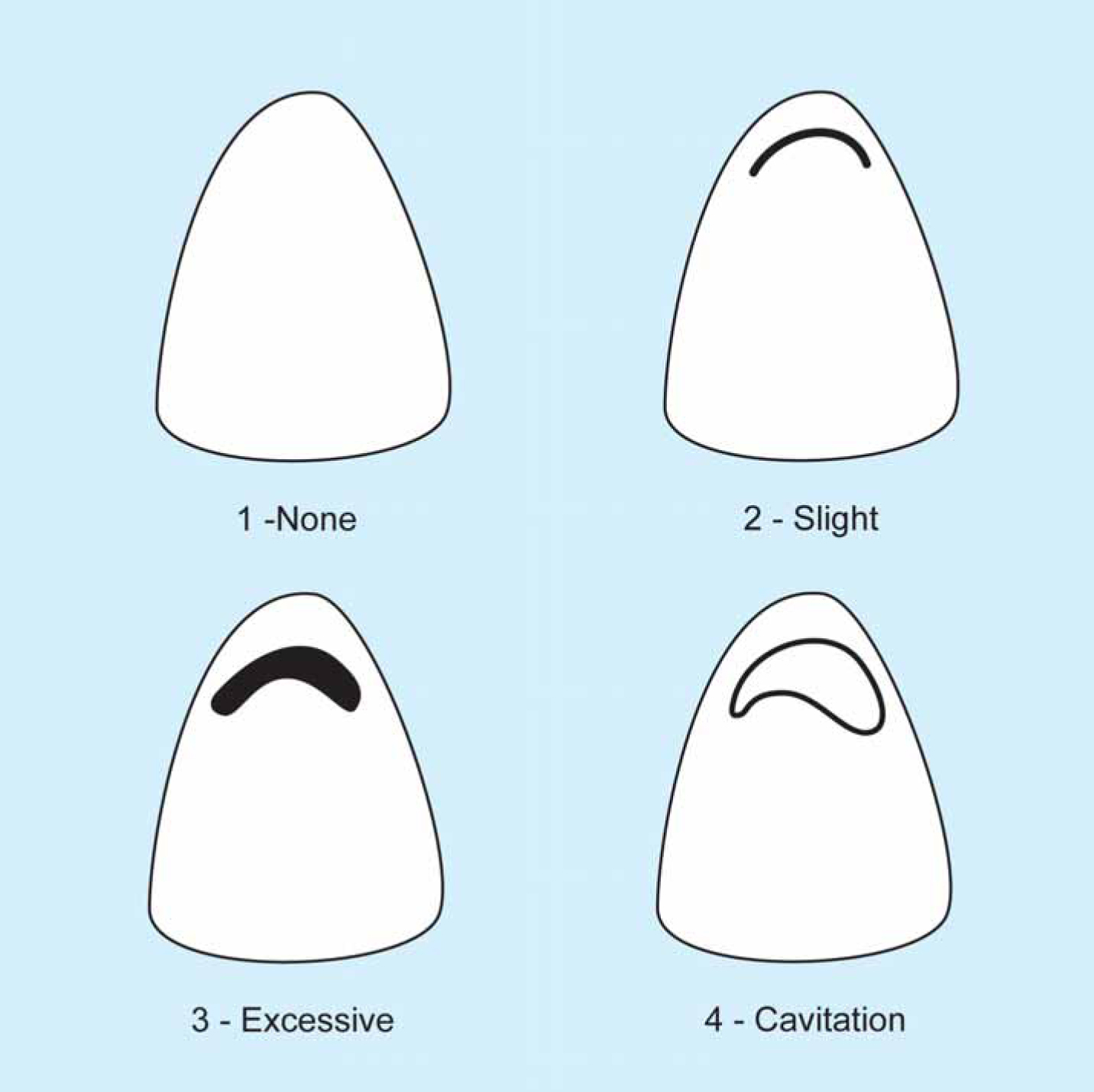
This is a clinical method where the enamel surfaces of the teeth are directly examined. The teeth are first cleaned and dried using an air drier, and then the number of areas of demineralization (white spots) is observed. The white spot lesion index2 can also be used to assess the severity of enamel loss. According to this index, the scores (Figure 2) given are as follows:
No white spot formation;
Slight white spot formation;
Excessive white spot formation;
White spot formation with cavitation.
Figure 2. Scoring according to the white spot lesion index.2
Direct examination of white spots is an inexpensive method which can be included in our routine clinical protocol. Pre- and post-treatment comparison between number of white spots and degree of decalcification can also be undertaken using this method. However, since it is a subjective evaluation method, some operator bias cannot be eliminated. Previous authors have used this method for in vivo studies.
Gorelick and co-workers studied the incidence and severity of white spots after full-term bonded and banded orthodontic treatment using direct examination.2 They concluded that there was an increase in white spots following orthodontic treatment in both banded and bonded teeth. Zimmer and Rottwinkel used the white spot lesion index2 to ascertain whether various indices could be used to predict the decalcification risk associated with orthodontic treatment.4 Secondly, a comparison was made between an extended prophylaxis regime and initial prophylaxis alone, in their ability to prevent demineralization. The results showed that patient selection based on caries risk factors provides a simple and effective method for predicting the decalcification risk. A significantly lower decalcification rate was seen on treatment with fluoride in combination with chlorhexidine than with fluoride alone. Although extended prophylaxis significantly reduced decalcification frequency in the at-risk group, it did not reach the low rate found in the low-risk group.
Photographic examination
Photographic examination can be used to evaluate the enamel surface using the same criteria as used in direct examination. The advantage here is that the data obtained can be stored; direct comparison between separate samples can be undertaken, and evaluation/scoring by multiple authors is also possible. However, photographs should be taken with the same camera with standardized setting of distance, illumination, aperture and film for direct comparison. The problem of bias persists even with this method as photographs are again subjectively evaluated/scored. The reflection of camera flash in the photographs may also lead to errors.
Gorelick and co-workers2 first used photographic examination for the comparison of pre-and post-treatment banded anterior teeth and concluded that the duration of treatment did not increase the risk of decalcification. Le et al compared the decalcification between cyanoacrylate and composite resin using photographs of orthodontic patients.5 A rating system was used to evaluate the enamel demineralization in which 10 dental professionals were shown pre- and post-treatment photographs of six anteriors at 1:1 magnification. Based on the results, the authors have concluded that cynoacrylates have similar amounts of decalcification as traditional composites. Kanthathas, Willmot and Benson conducted a study to investigate the differences between developmental opacities and post-orthodontic white enamel lesions.6 Photographic slides were converted to digital format and various measurements like area, luminance and shape of the lesion were made. The results showed that post-orthodontic white enamel lesions were larger in area, less white and had a rougher margin than developmental lesions. The authors suggested roundness/roughness as a useful measurement to distinguish between the two.
Stereomicroscopy
Stereomicroscopy (also known as dissecting microscopy) is a method used to observe surface topography. Since the decalcification of enamel is a surface phenomenon, this method can be used for study of white spots. The microscope applies two separate optical paths, objectives and eyepieces to view the sample from slightly different angles for the left and right eye to provide a three-dimensional view of the subject under observation. This method can be used to obtain images with a maximum magnification of 100x. Though not expensive, this method has not been used extensively in orthodontic research.
Zachrisson and Arthun used stereomicroscopy to study the quality of enamel after debonding.7 In this study, the enamel surface produced by different debonding modalities and composite removal procedures were compared. They designed a grading system called the enamel surface index (ESI) system, to evaluate the enamel observed under 50x magnification of stereomicroscopy. The criteria of the ESI system are as follows:
Score 0 = Perfect surface. No scratches, distinct intact perikymata;
Score 1 = Satisfactory surface. Fine scratches, some perikymata;
Score 2 = Acceptable surface. Several marked and some deeper scratches, no perikymata;
Score 3 = Imperfect surface. Several distinct deep and coarse scratches, no perikymata;
Score 4 = Unacceptable surface. Coarse scratches and deeply marred appearance. Based on the results of the grading, they concluded that a tungsten carbide bur, operated at low speed, produced the finest scratch pattern and the least enamel loss.
Scanning electron microscopy
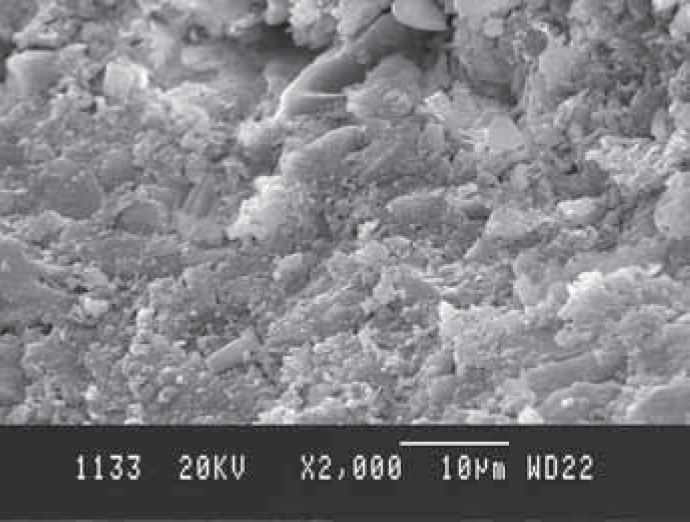
Scanning electron microscopy (SEM) is the most commonly used tool for orthodontic research. It is not only used to examine the enamel surface, but also for evaluation of the surface properties of orthodontic wires, bracket slot and mesh design before and after clinical use. High resolution images with a magnification of up to two million times can be obtained with SEM. When used to study demineralization, SEM images give a dramatic view of the enamel destruction (Figure 3) associated with orthodontic treatment; however, any measurement of mineral loss or estimation of depth of enamel loss is not possible since it is a magnified surface image.
Figure 3. SEM image of enamel destruction seen at 2000X magnification.
The available literature on SEM clearly indicates that all direct-bonding techniques entail an artificial weakening of the superficial enamel structure, and removal of the adhesive produces localized enamel detachments. Zachrisson and Arthun first used SEM to study enamel alterations produced by bracket bonding and debonding procedures at 320X, 1000X and 3200X magnification.7 Diedrich conducted an extensive study using SEM, wherein a total of 1,764 images of enamel under a range of magnifications between 40X and 10,000X, subjected to different processes of bonding, were obtained.8 It was seen that etching patterns were generally variable and etched adhesive-free enamel areas are only incompletely repaired. The penetration depth of resin tags, the repair process of etched enamel and the alterations by bracket removal were also observed. The resin tags generally reached a depth of 80 microns, sometimes extending to about 100 to 170 microns in length.
SEM studies have been done to demonstrate the effect of soft drinks on enamel. Steffen used SEM to examine teeth that were etched and bonded and held in cola type drinks for 72 hours.9 Dincer and co-workers determined the effect of acidic beverages on etched and sealed tooth enamel in a simulated oral environment using SEM.10 Both studies have reported significant demineralization.
Finally, SEM has also been used to demonstrate the efficiency of fluoride to minimize the demineralization of enamel during orthodontic treatment. Sadowsky et al, using SEM as one of the experimental tools, have concluded that the resistance of enamel to demineralization is directly proportional to its fluoride uptake.11 In another study, SEM indicated greater loss of enamel by phosphoric acid than polyacrylic acid. Hence, Summers et al have suggested that the use of resin-modified glass ionomer is less harmful to enamel than conventional resin adhesives.12
Stylus profilometer
The stylus profilometer is a precision instrument, which has a highly sensitive stylus (Figure 4). It records the surface irregularities and produces a three dimensional digital image. This method is highly sensitive in determining roughness produced by various orthodontic procedures; however, the enamel surface under study should be polished before subjection to test conditions.
Figure 4. Stylus profilometer.
Tufekci et al13 have used the stylus profilometer to determine the volume of enamel loss associated with orthodontic adhesive removal on teeth with white spot lesions. Here the enamel surface was not polished but the test specimens were initially digitalized using the stylus profilometer. After debonding and resin removal the surfaces were redigitized. The exact cubic millimeter of enamel lost was determined using AnSur NT software by comparing the baseline recording with the final debonding recording.
Polarized light microscopy
Polarized light microscopy exploits the optical property of anisotropy to reveal detailed information about the structure and composition of enamel. Here the qualitative assessment of a section of enamel can be undertaken to determine the mineral content. With polarized light, all the waves of light vibrate in the same direction. When this passes through the enamel, depending on the mineral content at different points in the sample, the beam is channelled to produce variable refractive patterns called ‘birefringence’. In this technique, a polarizer is used to produce a beam of polarized light to pass through the cross-section of the sample and the birefringence so produced is visualized using an analyser. The sections are photographed in a water imbibition medium which has a refractive index of 1.33, as compared to sound enamel refractive index of 1.62. The contrast produced is of high quality and even a small amount of mineral loss can be noticed. However, since the cross-section of the sample is taken, the surface roughness cannot be determined.
Vorhies et al evaluated the enamel demineralization adjacent to orthodontic brackets bonded with hybrid glass ionomer cements using polarized light microscopy.14 A significant difference in area and depth of demineralization of enamel was seen between glass ionomer cement and composite resin. Enamel samples bonded with hybrid glass ionomer cement had the least demineralization. The brand of glass ionomer and brushing made no difference in the test groups but, in the control group, brushing with Transbond XT (3M Unitek, UK and Ireland) reduced demineralization. Polarized light microscopy was used by Wilson and Donly to compare the demineralization around orthodontic brackets, bonded with resin-modified glass ionomer cement (Fuji Ortho LC, GC America, Illnois, USA) and fluoride-releasing composite resin (Light Bond, Reliance, Illinois, USA).15 Artificial caries solution was employed to create lesions. The results showed that both the fluoride-containing materials had significantly less adjacent enamel demineralization than the non-fluoride-releasing composite resin control.
Microradiography
This is a method similar to polarized light microscopy wherein a cross-section of the sample can be analysed for its mineral content. Here radiographs of higher resolution of the sample are taken; the difference in the mineral content produces a variable pattern of opacities and helps to determine the amount of demineralization of enamel. Sadowsky and co-workers used microradiography as one of the methods for evaluation of enamel beneath cemented orthodontic bands and concluded that the resistance of enamel to demineralization was directly proportional to its fluoride uptake.11
Cross-sectional microhardness
Hardness is defined as the ability of a substance to resist indentation. Barcol, Rockwell, Brinell, Shore, Vickers and Knoop hardness testers are most commonly used in dentistry. The load applied by the tester divided by the surface area gives us the hardness number, which is used to describe the physical properties of enamel, dentine or various restorative materials. The Knoop and Vickers tests are classified as microhardness tests as they apply loads less than 9.8 N, resulting in small indentations. When used at different cross-sections, it is called cross-sectional microhardness.
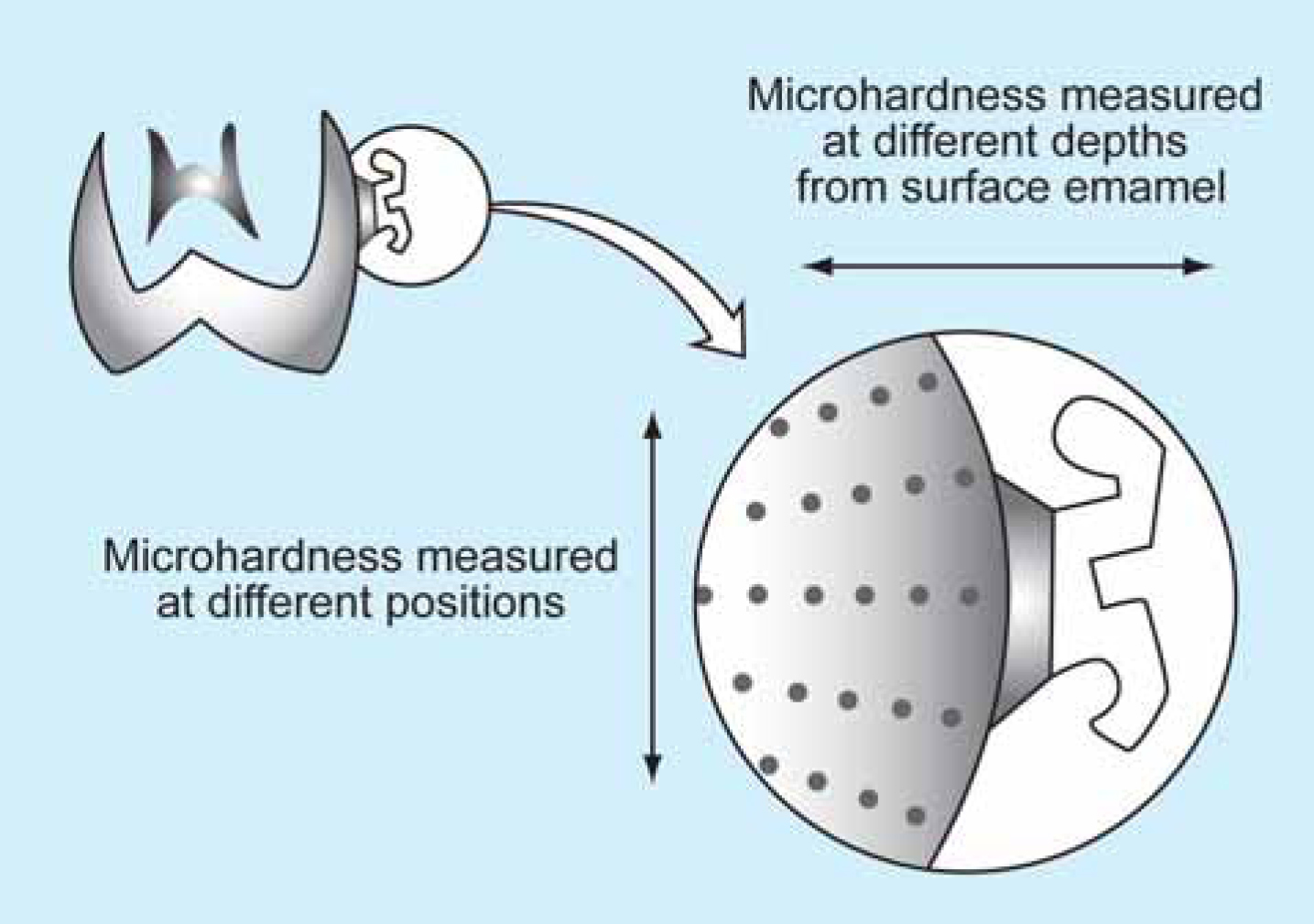
The study sample is first sectioned buccolingually and embedded in epoxy resin. The microhardness tests of enamel are made at various depths from the surface (Figure 5) and different levels vertically. Since the hardness of enamel is related to its mineral content, any reduction in this hardness number is directly proportional to demineralization of enamel. Thus a quantitative estimate of enamel loss at different positions and depths can be easily done using this method.
Figure 5. Measurement of cross-sectional microhardness of enamel.
Cross-sectional microhardness was first used by O'Reilly and Featherstone to determine quantitatively the demineralization and remineralization around orthodontic appliances in patients, using different oral hygiene aids.16 The Knoop hardness number of five areas with respect to the bracket at varying depths within surface enamel was determined and the percentage of mineralization determined. The authors concluded that measurable demineralization (15% demineralization up to a depth of 50 microns) was seen in a time period of less than one month and that a combination of various fluoride-containing oral hygiene aids inhibit demineralization of the surface at risk. The same protocol was used by Gorton and Featherstone17 to verify whether fluoride released from glass ionomer inhibits demineralization around orthodontic brackets. The quantitative evaluation by cross-sectional microhardness testing demonstrated less demineralization around brackets bonded with glass ionomer. But the cariostatic effect was localized to the area around the bracket. The efficiency of resin-modified glass ionomer cement (Fuji Ortho LC) in reducing enamel demineralization when compared with composite resin (Concise, 3M Unitek Corp, Monrovia, Calif) was demonstrated by Pascotto et al using the same method.18
Cross-sectional microhardness is an efficient method for quantitative estimate of enamel. As cross-sections of the sample are taken, this method can only be used for experimental evaluation of various bonding materials and cannot be used for enamel surface evaluation or routine clinical evaluation of white spots.
Conclusion
All clinicians and researchers agree that orthodontic treatment procedures are associated with some degree of enamel demineralization. However, the method used to determine this destruction is highly variable. Direct examination and grading can be used for enamel evaluation in routine clinical cases and this data can also be stored using photography. Stereomicroscopy, scanning electron microscopy (SEM) and stylus profilometer are useful to study the surface alterations of enamel. Stereomicroscopy is applicable at lower magnifications and SEM at higher magnifications. A profilometer can be used in cases where accurate calculations of surface topography are needed. However, when mineral loss at different depths of enamel is to be evaluated, polarized light microscopy, microradiography or cross-sectional microhardness should be used. Thus we can conclude that the selection of the method for study of demineralization of enamel associated with orthodontic treatment should be based on the scientific objectives of the study and not merely on the availability of equipment.