Ericson S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines: a CT-study. Angle Orthod. 2000; 70:415-423
Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005; 128:418-423
Bjerklin K, Guitirokh CH. Maxillary incisor root resorption induced by ectopic canines. A follow-up study, 13 to 28 years post treatment. Angle Orthod. 2011; 81:(5)800-806
Liu DG, Zhang WL, Zang ZY Localisation of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:91-98
Cernochova P, Krupa P, Izakovicova-Holla L. Root resorption associated with ectopically erupting maxillary permanent canines: a computed tomography study 2010. Eur J Orthod. 2011; 33:483-491
Strbac GD, Foltin A, Gahleitner A, Bantleon HP, Watzek G, Bernhart T. The prevalence of root resorption of maxillary incisors caused by impacted maxillary canines. Clin Oral Invest. 2013; 17:553-564
Alqerban A, Jacobs R, Lambrechts P, Loozen G, Willems G. Root resorption of the maxillary lateral incisor caused by impacted canine: a literature review. Clin Oral Invest. 2009; 13:247-255
Becker A, Chaushu S. Long-term follow-up of severely resorbed maxillary incisors after resolution of an etiologically associated impacted canine. Am J Ortho Dentofacial Orthop. 2005; 127:650-654
Shellhart WC, Jasper S, Abrams H, Wilson T. Case report: management of significant incisor root resorption associated with maxillary canine impaction. Angle Orthod. 1998; 68:(2)187-192
D'Amico RM, Bjerklin K, Kural J, Falahat B. Long-term results of orthodontic treatment of impacted maxillary canines. Angle Orthod. 2003; 73:231-238
Millberg D. Labially impacted maxillary canines causing severe root resorption of maxillary central incisors. Angle Orthod. 2005; 76:173-176
Falahat B, Ericson S, Mak D'Amico R, Bjerklin K. Incisor root resorption due to ectopic maxillary canines – a long-term radiographic follow-up. Angle Orthod. 2008; 78:778-785
Albaker BK, Wong RW. Diagnosis and management of root resorption by erupting canines using cone-beam computed tomography and fixed palatal appliance: a case report. J Med Case Rep. 2010; 4:(1)
Bjerklin K, Ericson S. How a computerized tomography examination changed the treatment plans of 80 children with retained and ectopically positioned maxillary canines. Angle Orthod. 2006; 76:43-51
Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987; 91:483-492
Kurol J, Ericson S, Andreason JO. The impacted maxillary canine. In: Andreasen JO, Petersen KJ, Laskin D Copenhagen: Munksgaard; 1997
Alqerban A, Jacobs R, Souza PC, Willems G. In-vitro comparison of 2 cone-beam computed tomography systems and panoramic imaging for detecting simulated canine impaction-inducted external root resorption in maxillary lateral incisors. Am J Orthod Dentofacial Orthop. 2009; 136:(6)764.e1-11
Preda L, La Fianza A, Di Maggio EM The use of spiral computed tomography in the localization of impacted maxillary canines. Dentomaxillofac Radiol. 1997; 26:236-241
Ericson S, Kurol J. Incisor root resorptions due to ectopic maxillary canines imaged by computerized tomography: a comparative study in extracted teeth. Angle Orthod. 2000; 70:(4)276-283
Mah JK, Danforth RA, Bumann A, Hatcher D. Radiation absorbed in maxillofacial imaging with a new dental computed tomography device. Oral Surg Oral Med Oral Pathol Endod. 2003; 96:508-513
Kau CH, Richmond S, Palomo JM, Hans MG. Three-dimensional cone beam computerized tomography in orthodontics. J Orthod. 2005; 32:(4)282-293
There is extensive material in the orthodontic literature regarding canine ectopia but far less on the possible sequelae of ectopic canines, such as the resorption of maxillary incisor roots. This is the second paper in a two-part series exploring the subject of ectopic canines inducing root resorption of maxillary incisors. The first paper examined the orthodontic and dental literature in order to compile a review of the prevalence rates and longevity outcomes of maxillary incisor root resorption as a result of impacted maxillary canines. This second paper will explore the clinical management of patients with maxillary incisor resorption as a result of an impacted maxillary canine.
Clinical Relevance: Maxillary incisor root resorption induced by ectopic maxillary canines is an issue for all dental specialties; however, the awareness of each stage of management is limited. This paper aims to increase awareness and provide a reference point for appropriate management by clinicians.
Article
The prevalence of maxillary incisor root resorption induced by ectopic maxillary canines has been shown to range between 7.7% and 66.7% and the prevalence of central incisor resorption to range between 2% and 23%, according to various studies utilizing CT scanning.1,2,3,4,5,6 In addition, the female-to-male ratio of susceptibility varies between 2:1, 3:1, 4:1 and 10:1.7,8 The process of resorption can be rapid and therefore treatment must be carried out urgently to move the impacted canine away from the affected tooth, as cessation of resorption has been shown to occur following orthodontic treatment.9
Despite the limited data, our previous literature review has concluded that the overall long-term prognosis of resorption of maxillary incisors induced by impacted canines has been shown to be positive, with minimal loss of affected incisors having been demonstrated in various studies over a 1–28-year follow-up.3,9,10,11,12,13,14,15
After exploring the prevalence and longevity outcomes of resorbed incisors, this paper will examine the various clinical factors and treatment options, with the aim of helping clinicians formulate appropriate management plans to achieve optimal outcomes.
Clinical and radiographic investigation
The initial clinical examination begins with a thorough visual assessment and bimanual palpation. Canine ectopia should be suspected if bimanual palpation fails to confirm the presence of the canine in the buccal sulcus by the age of 10–11 years. In addition, if an asymmetrical eruption pattern is noted with the canine on one side of the arch having erupted favourably, but the contralateral canine having failed to erupt for at least 6–9 months later, this may also be indicative of an impacted canine (Figure 1).
Figure 1. Unerupted UR3 with erupted contralateral UL3.
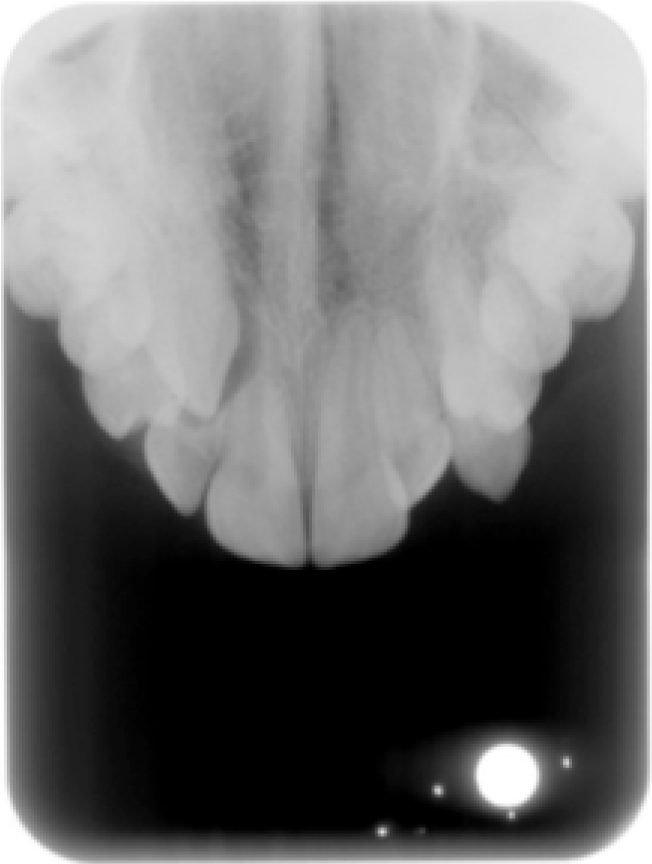
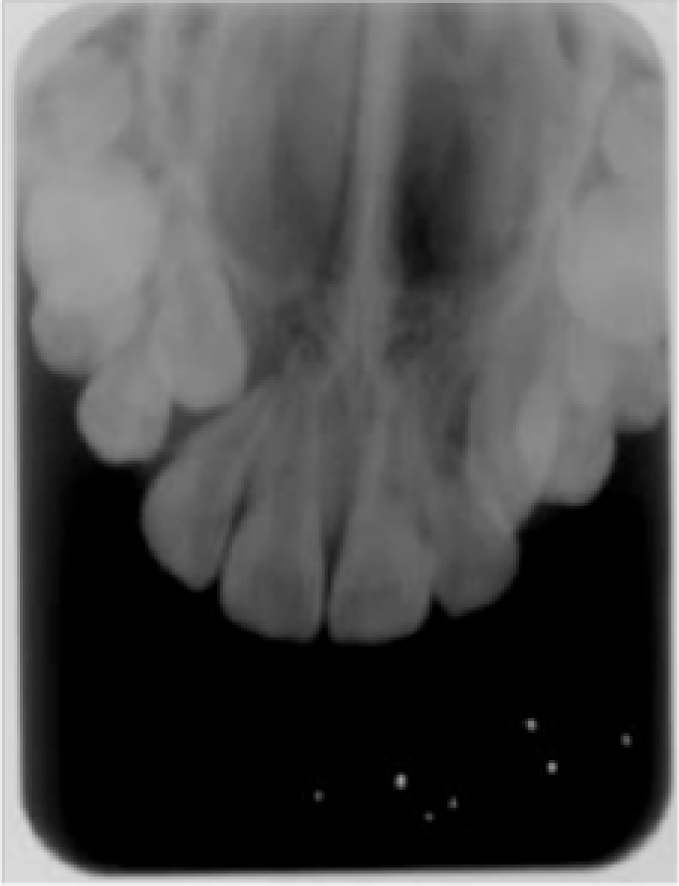
If a definitive diagnosis is not satisfied by clinical examination, then radiographic investigation is justified. Plain film radiography remains the most commonly used diagnostic tool, which allows the vertical and mesio-distal relationship of the unerupted tooth and neighbouring structures to be examined. A number of radiographic views may be used to aid the diagnosis of the position of the canine and to assess the incisor roots for resorption. These include an orthopantomogram or upper standard occlusal, a lateral cephalogram or periapical views. The technique of vertical or horizontal parallax may be used to aid positional diagnosis based on the location of the object of interest in relation to x-ray tube shift with two different views.16Figures 2 and 3 exhibit an orthopantomogram (OPG) and upper standard occlusal view (USO) investigating root resorption of an upper right lateral incisor due to an ectopic maxillary canine.
Figure 2. OPG showing impacted upper right canine causing resorption of upper right lateral incisor root.Figure 3. Upper standard occlusal showing impacted upper right canine causing resorption of upper right lateral incisor root.
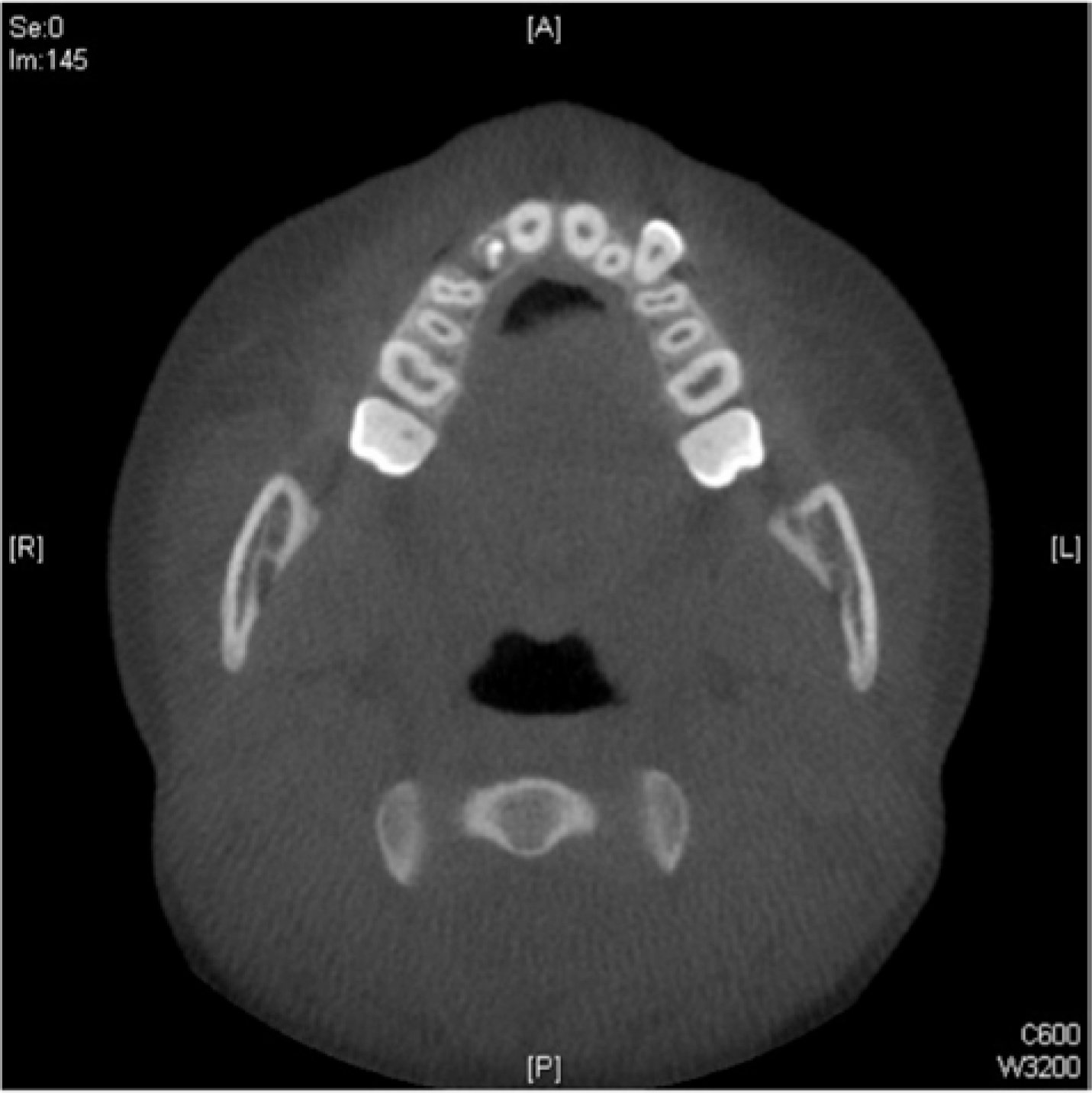
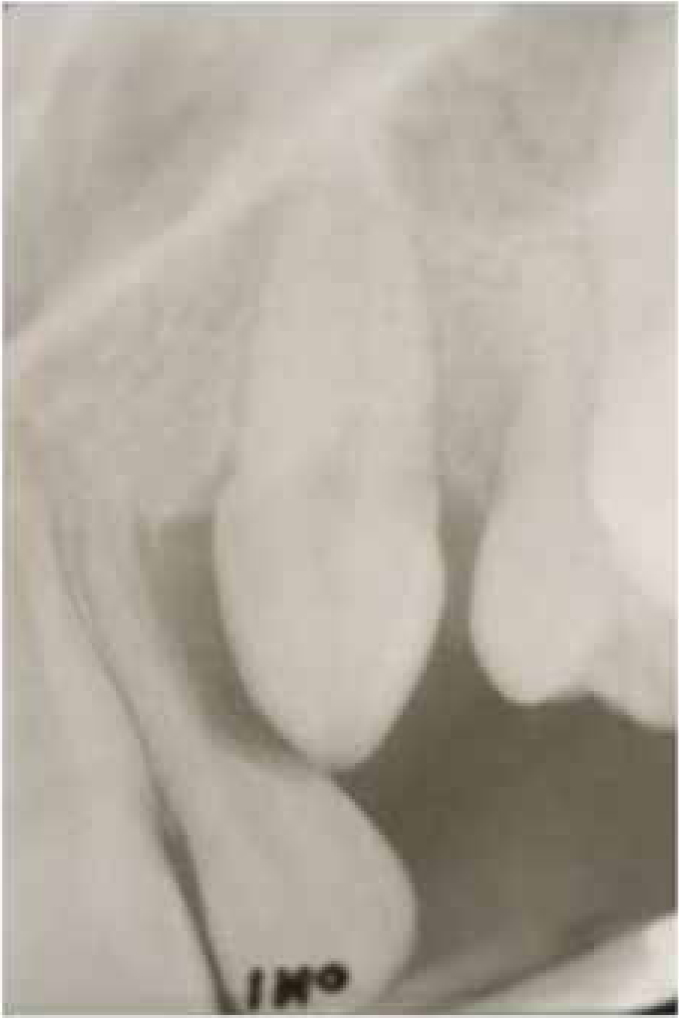
However, the reliability of plain film radiography for the specific diagnosis of resorption of maxillary incisor roots has been found to be unreliable owing to various diagnostic errors, including superimposition, poor definition, distortion and artefacts.17,18,19 Studies have shown severe resorption can occur without any detection on plain films.17,20 These shortcomings have been minimized by the advent of Computed Tomography (CT), which has shown a 50% increase in the detection of incisor resorption compared to that of conventional radiography.17,21Figure 4 demonstrates a CT view of the previously mentioned resorbed lateral incisor that indicates the impacted upper right canine causing resorption of the upper right lateral incisor root.
Figure 4. CT scan exhibiting impacted upper right canine causing resorption of upper right lateral incisor root.
Cone Beam Computerized Tomography (CBCT) has been deemed the successor of conventional CT imaging and has proved to be an excellent medium for the investigation of impacted teeth, the presence of supernumeraries and, indeed, to diagnose root resorption, both from impacted canines and from orthodontically induced forces. The total radiation dosage for CBCT is quoted to be about 20% that of CTs or a full mouth periapical radiographic exposure.22 The clinician essentially has ‘the diagnostic quality of periapicals, panoramic, cephalograms and occlusal radiographs, and temporomandibular joint (TMJ) series along with a view that cannot be produced by regular radiographic machines like axial view, and separate cephalograms for the right and left sides.’23
The management of maxillary incisor teeth that have been resorbed by an ectopic maxillary canine must begin with an assessment of the long-term prognosis of the resorbed incisor, which this paper will now address.
Assessment of the prognosis of the resorbed incisor
A logical and sequential process of clinical and radiographic diagnosis of a resorbed incisor root as a result of an impacted canine must be made to allow for a clinical judgement on the prognosis of the resorbed incisor, as well as on the prognosis for successful alignment of the impacted canine to be made. This decision can be made on the basis of the following factors:
Space requirements;
Severity of resorption of the incisor;
Overall malocclusion.
Space requirements
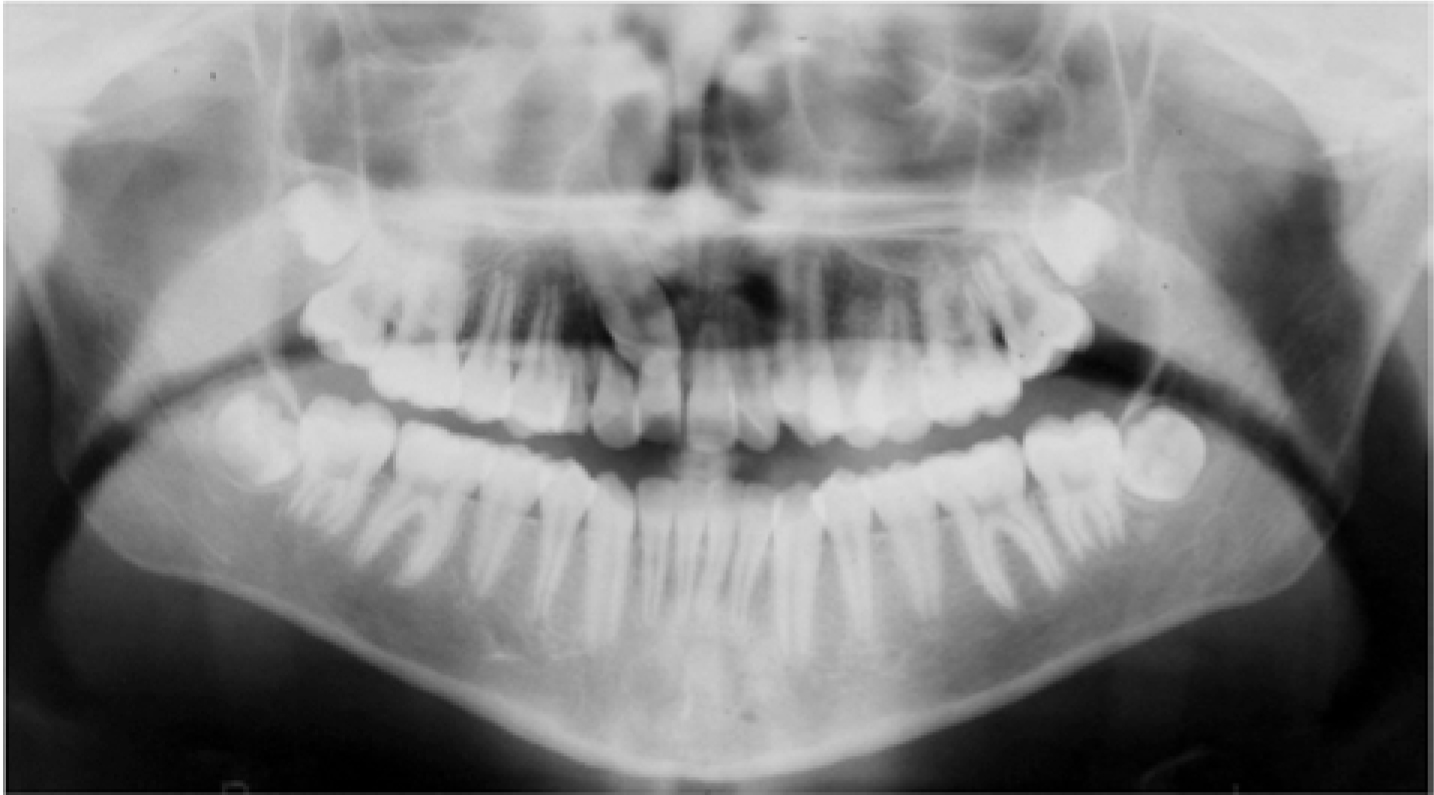
If there is moderate to severe crowding in the maxillary arch and therefore a need to create space in the arch by extraction in order to accommodate an impacted canine in the arch, there are a number of options for extraction. Either a premolar can be extracted to provide space to align the canine or, indeed, the impacted canine (if it is in an unfavourable position for alignment) may be extracted. However, if there is moderate to severe resorption of the lateral incisor, then extraction of the resorbed lateral incisor can be considered to allow the alignment of the impacted canine, which has a better long-term prognosis. An example of such a situation is illustrated in the OPG (Figure 5). Where there is moderate crowding in the upper right quadrant, there is the need to provide space in the arch by extraction, but there is moderate to severe resorption of both the upper right central and lateral incisor.
Figure 5. Moderate to severe resorption of upper right central and lateral incisors.
The options in this case are to extract either the first premolar or lateral incisor in order to accommodate the impacted right canine. However, as the lateral incisor was moderate to severely resorbed, the decision was taken to extract the lateral incisor and the canine could then be aligned in its place. The upper right central incisor was not considered for extraction, despite its resorption, as it may be more difficult to mask the canine as a central incisor from the restorative point of view. In addition, as discussed in our first paper, a literature review of the longevity of resorbed incisors showed these teeth to have a better long-term prognosis than anecdotally assumed.3,11,12,13,14 In the long term, it is also argued that, if the resorbed central incisor is eventually lost due to the extensive resorption, it can be replaced with a dental implant that would guarantee a more predictable aesthetic outcome, from the restorative point of view, than masking a maxillary canine as a central incisor.
The decision to extract a lateral incisor and align an impacted canine in its place will have to be made based on a number of factors. For example, the suitability of the canine as a substitute incisor will depend on its colour, shape, emergence profile, gingival margin and the patient's lip line. If the canine can be easily masked as a lateral incisor, the overall aesthetics of the upper labial segment will be maintained, whereas if the canine will not make a suitable replacement of the lateral incisor, the resulting aesthetics can be compromised. Figure 6 shows an example of a canine that has a very bulbous crown and prominent canine tip, as well as a high gingival margin, and will subsequently make a poor aesthetic replacement for a lateral incisor.
Figure 6. Bulbous canines with high gingival margins.
Severity of resorption of the incisor
Severity of resorption is a determining factor in the long-term prognosis of the incisor. The most popular classification was devised by Ericson and Kurol in 2000, which utilizes four categories:
‘No resorption’ describes an intact root surface;
‘Slight resorption’ depicts extension up to half the dental thickness to the pulp;
‘Moderate resorption’ extends midway to the pulp;
A pulpal exposure is subsequently classed as ‘severe resorption’.1
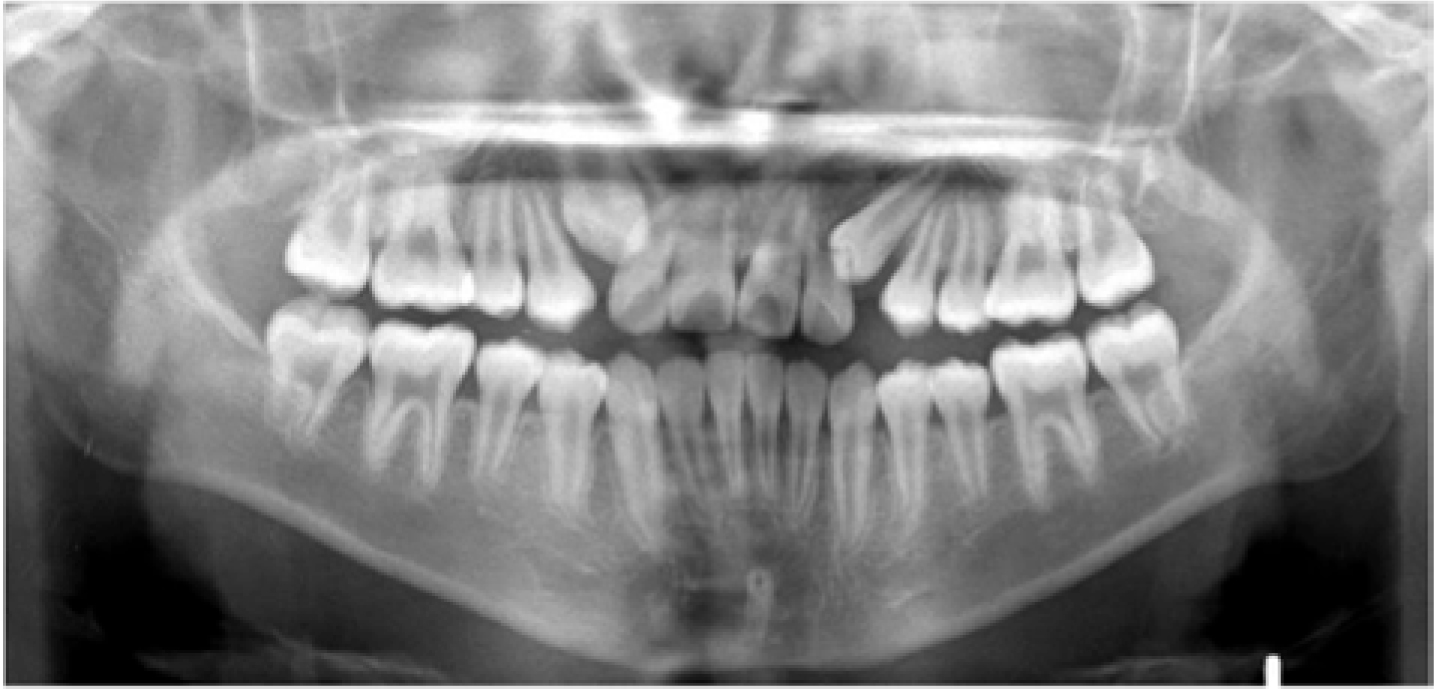
If it is only slightly resorbed, then the long-term prognosis is better and the tooth may be maintained in the arch as opposed to being extracted. Figures 7 and 8 demonstrate severe resorption relating to the upper left lateral incisor, which indicated a poor long-term prognosis.
Figure 7. OPG exhibiting impaction of upper canines.Figure 8. Upper standard occlusal showing resorption of the upper left lateral incisor which appears to have affected over two-thirds of the root.
Overall malocclusion
The overall malocclusion has a bearing on the management of a resorbed incisor as, for example, in a Class III camouflage case it may be better to keep the resorbed incisor rather than to extract it and close the space, as this may cause over retraction of the upper incisors, which may worsen the Class III relationship. This decision is dependent of course on the severity of resorption. Only following this clinical judgement on the prognosis of alignment can detailed discussion be undertaken with the patient to determine patient expectations. If the prognosis of the resorbed incisor is poor, the patient must be made aware of the need for its prosthetic replacement in the long term. Thereafter the patient can provide informed consent to proceed with the treatment options. At this stage, joint treatment planning with restorative, paediatric and oral surgery specialties may also be beneficial. Different treatment options include:
Surgical exposure and orthodontic traction of canine;
Extraction of the resorbed incisor;
Extraction of the maxillary canine.
Surgical exposure and orthodontic traction of canine
This option should be considered if the canine is in a favourable position for alignment and if there is only mild to moderate resorption of the maxillary incisor roots. In such situations, orthodontic traction can help direct the canine away from the affected roots, therefore eliminating pressure leading to cessation of the resorptive stimulus.5 In the long term, the resorbed incisor can be maintained as a space maintainer until it is lost.9
Extraction of the resorbed incisor
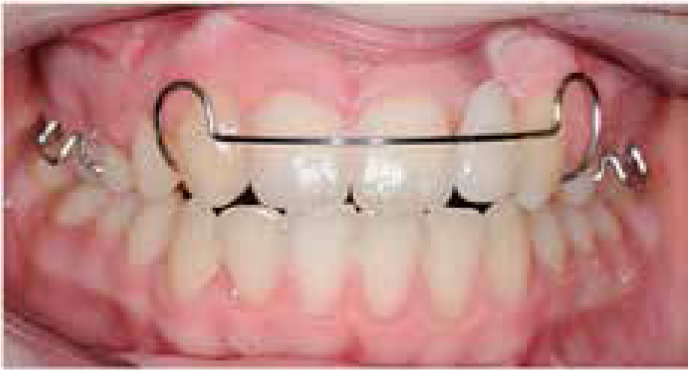
This should be considered should severe resorption (Figures 9,10,11,12) of an incisor root have occurred as a result of an impacted canine and subsequently the resorbed incisor has a poor prognosis which may lead to loss during or after treatment.8 It should also be considered if it is likely that any attempt to align the impacted canine may cause further resorption to the incisor root. In circumstances where there is a lack of space, it may be more beneficial to remove a resorbed lateral incisor rather than an intact premolar.3 The canine is subsequently disguised as a lateral incisor following eruption of the canine or a space maintainer is placed for future prosthesis (Figure 13). Ideally this decision can be made jointly with a restorative dentist. Figure 14 exhibits an upper left lateral incisor (previously shown in Figures 7 and 8) which was extracted due to its severe resorption, mobility and subsequent poor prognosis.
Figure 9. The upper right maxillary canine has caused significant resorption with pulpal involvement of the upper right lateral incisor.Figure 10. OPG radiograph shows extensive resorption of both upper lateral incisors from maxillary canines.Figure 11. Severe resorption of upper right lateral incisor.Figure 12. Severe resorption of upper left lateral incisor.Figure 13. Upper right canine disguised as a lateral incisor with space maintainer of the upper left lateral space.Figure 14. UL2 distal view of upper left lateral incisor with severe root resorption into the pulp chamber.
Extraction of the maxillary canine
This treatment option may be considered when the canine is in a poor position for alignment, or of poor morphology in terms of ease of camouflage as an incisor and there is mild resorption of the incisor. This may be judged by the appearance of the contralateral canine if it is erupted. This option can reduce orthodontic treatment time and prevent further damage to the maxillary central incisors. Monitoring of the health of the maxillary incisors prior to and during the orthodontic treatment is advisable.12
Conclusion
The clinical management of a resorbed maxillary incisor induced by an ectopic canine depends on a number of factors, such as an assessment of the overall malocclusion, the prognosis for alignment of the impacted canine, the space requirements in the arch, as well as the severity of resorption of the affected incisor. A systematic clinical and diagnostic approach in conjunction with a knowledge of literature should provide the basis for evidence-based practice for the appropriate management of resorbed maxillary incisors induced by ectopic canines.