Andreasen JO, Sundstrom B, Ravn JJ The effect of traumatic injuries to primary teeth on their permanent successors. I. A clinical and histological study of 117 injured permanent teeth. Scand J Dent Res. 1971; 79:219-283
Andreasen JO, Ravn JJ The effect of traumatic injuries to primary teeth on their permanent successors. II. A clinical and radiographic follow-up study of 213 teeth. Scand J Dent Res. 1971; 79:284-294
Andreasen JO, 3rd edn. In: Andreasen JO, Andreasen FM Copenhagen: Munksgaard; 1994
Howard RD The congenitally displaced maxillary incisor: a differential diagnosis. Dent Practit. 1969; 20:361-371
Stewart DJ Dilacerate unerupted maxillary central incisors. Br Dent J. 1978; 145:229-233
Kearns HPO Dilacerated incisors and congenitally displaced incisors: three case reports. Dent Update. 1998; 25:339-342
Smith DMH, Winter GB Root dilaceration of maxillary incisors. Br Dent J. 1981; 150:125-127
Filippi A, Pohl Y, Tekin U Transplantation of displaced and dilacerated anterior teeth. Endod Dent Traumatol. 1998; 14:93-98
Cozza P, Marino A, Condo R Orthodontic treatment of an impacted dilacerated maxillary incisor: a case report. J Clin Pediatr Dent. 2005; 30:93-98
Tsai TP Surgical repositioning of an impacted dilacerated incisor in mixed dentition. J Am Dent Assoc. 2002; 133:61-66
Kuroe K, Tomonari H, Soejima K, Maeda A Surgical repositioning of a developing maxillary permanent central incisor in a horizontal position: spontaneous eruption and root formation. Eur J Orthod. 2006; 28:206-209
Tanaka E, Hasegawa T, Hanaoka K Severe crowding and a dilacerated maxillary central incisor in an adolescent. Angle Orthod. 2006; 76:510-518
Kolokithas G, Karakasis D Orthodontic movement of dilacerated maxillary central incisor. Am J Orthod. 1979; 76:310-315
Uematsu S, Uematsu T, Furusawa K, Deguchi T, Kurihara S Orthodontic treatment of an impacted dilacerated maxillary central incisor combined with surgical exposure and apicoectomy. Angle Orthod. 2004; 74:132-136
McNamara T, Woolfe SN, McNamara CM Orthodontic management of a dilacerated maxillary central incisor with an unusual sequela. J Clin Orthod. 1998; 32:293-297
Singh GP, Sharma VP Eruption of an impacted maxillary central incisor with an unusual dilaceration. J Clin Orthod. 2006; 40:353-356
Davies PHJ, Lewis DH Dilaceration - a surgical/orthodontic solution. Br Dent J. 1984; 156:16-18
Machtei EE, Zyskind K, Ben-Yehouda A Periodontal considerations in the treatment of dilacerated maxillary incisors. Quintessence Int. 1990; 21:357-360
Rose JS, Cannell H Treatment of an inverted unerupted central incisor. Br Dent J. 1975; 138
Chew MT, Ong MM-A Orthodontic-surgical management of an impacted dilacerated maxillary central incisor: a clinical case report. Pediatr Dent. 2004; 26:341-344
Heaney TG, Atherton JD Periodontal problems associated with the surgical exposure of unerupted teeth. Br J Orthod. 1976; 3:79-85
Vermette ME, Kokich VG, Kennedy DB Uncovering labially impacted teeth: apically positioned flap and closed-eruption techniques. Angle Orthod. 1994; 65:23-34
Lin Y-TJ Treatment of an impacted dilacerated maxillary central incisor. Am J Orthod Dentofacial Orthop. 1999; 115:406-409
Becker A, 1st edn. London: Martin Dunitz; 1998
Brands WG The standard for the duty to inform patients about risks: from the responsible dentist to the reasonable patient. Br Dent J. 2006; 201:207-210
Labial fenestration of a ‘dilacerated’ maxillary central incisor apex: an orthodontic complication Robert AC Chate Denis T Falconer Orthodontic Update 2025 5:4, 118-121.
A case is presented of a ‘dilacerated’ central incisor whose apex perforated the labial alveolus following orthodontic traction subsequent to its surgical exposure, which then necessitated endodontic treatment and an apicoectomy. The literature is reviewed regarding the aetiology and terminology of this complication and the implications for informed consent in such cases are discussed.
Clinical Relevance: This article will clearly differentiate between the two types of incisor root deflections that may occur during development. That is, those with true incisor palatal root dilacerations and those with pseudo-dilacerations which are actually incisors with vestibular root angulations.
The surgical and orthodontic recovery of an unerupted central incisor with a vestibular root angulation is outlined, in particular the management of the manifestation of one of the risks associated with this procedure, namely that of inducing an alveolar fenestration with the apex of the tooth during the process.
Article
Dilaceration is the presence of an angulation between the crown and the root of a maxillary incisor tooth. It only applies to an incisor that has had its crown deflected palatal to the long axis of the tooth during development. In contrast, the term vestibular root angulation describes a case where the incisor crown has been deflected labially.1
Incidence and aetiology
True dilacerations have been estimated to occur in 3% of all forms of incisor injuries.2 The root of the deciduous predecessor, during an intrusive luxation or avulsion, can cause a palatal rotation of the permanent incisor crown around the vascular dental papilla. As Hertwig's sheath remains in position, root formation of the permanent incisor continues along the original long-axis, thus creating the angulation between crown and root. At about the age of two years,3 and for only a relatively short period of time,4,5,6 the developing permanent central incisor is palatal to the roots of its deciduous predecessor, during which time this type of injury can occur.
In contrast, vestibular root angulations or pseudo-dilacerations are developmental disturbances that result in marked curvatures that are confined to the roots of permanent maxillary incisors. They are considered to be the result of primary incisor intrusive luxation and avulsion injuries sustained between the ages of 2–5 years.3 By this time the permanent incisor crowns have moved labially to overlie the resorbing primary incisor roots.5 Once again, Hertwig's epithelial root sheath remains in position, despite the impact, but in these cases the fully formed incisor crown is pushed labially, creating the root curvature.3
Smith and Winter found that in 8 of their 11 cases with vestibular root angulation there was a definite history of trauma.7 However, in an earlier study of 29 patients this was not found to be the case by Stewart, who instead proposed an alternative hypothesis that vestibular root angulations were most likely the result of an ectopic development of the tooth germ.5
Histological features
There are clear histological differences between dilacerated incisors and those with vestibular root angulations. The palatal crown deflections of dilacerated incisors that leave the roots to continue to develop normally induce characteristic macroscopic and microscopic changes. On the facial side, the stretched inner enamel epithelium is unable to express new enamel formation and, consequently, a horizontal band of exposed dentine without enamel cover develops. On the palatal aspect, the displaced enamel epithelium forms a cone of hard tissue that projects into the pulp canal, forming an enamel-covered cusp at the cervical margin.2
In contrast, maxillary incisors with vestibular root angulations show no histological signs of coronal hard tissue damage, merely a thickening of cementum in the area of root angulation.3
Treatment options
Surgical removal is a common option chosen for managing unerupted dilacerated incisors,8 together with subsequent orthodontic treatment either to close the space or to re-open it for a prosthetic replacement.9
The alternatives of surgically repositioning the dilacerated tooth,10,11 or of undertaking a semi auto-alloplastic crown/pulp chamber titanium post transplant, are less common.8
In many instances, attempts have been made to recover, orthodontically, dilacerated incisors following either an open exposure,12,13,14 a closed exposure,9,15,16,17,18 or through one made with an apically repositioned flap.19,20
Nevertheless, each of these methods have inherent disadvantages that range from non-keratinized gingival crown attachments associated with open exposures,21 to increased clinical crown lengths, vertical gingival scars and the intrusive relapse of teeth that have been exposed through the use of apically repositioned flaps.22
Case report
DW, a male Caucasian, presented with a Skeletal 1 base and an Angle's Class I malocclusion. He had an unerupted upper left permanent central incisor that was potentially excluded from the line of the arch and palpable high up in the labial sulcus. As a consequence, the upper dental midline was displaced 5 mm to the left of the facial midline (Figures 1, 2).
Figure 1. Intra-oral frontal view of the unerupted upper left central incisor.Figure 2. Intra-oral occlusal view of the unerupted upper left central incisor.
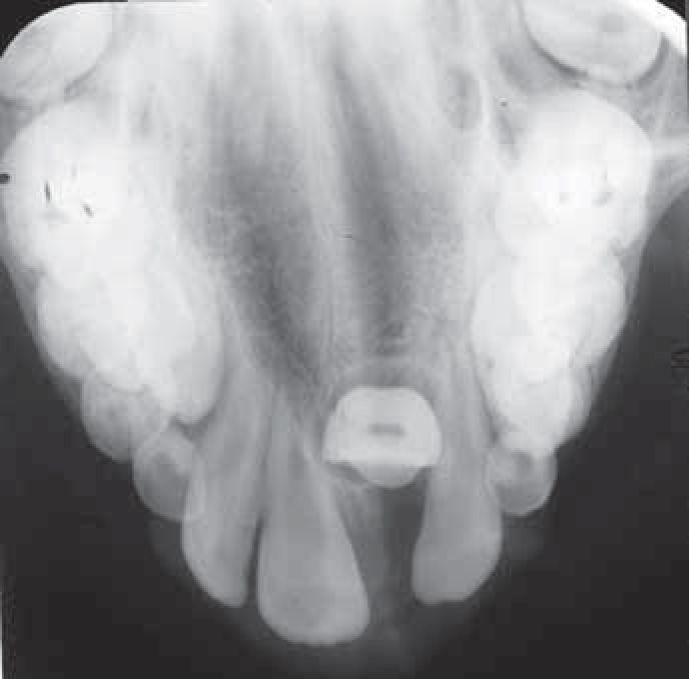
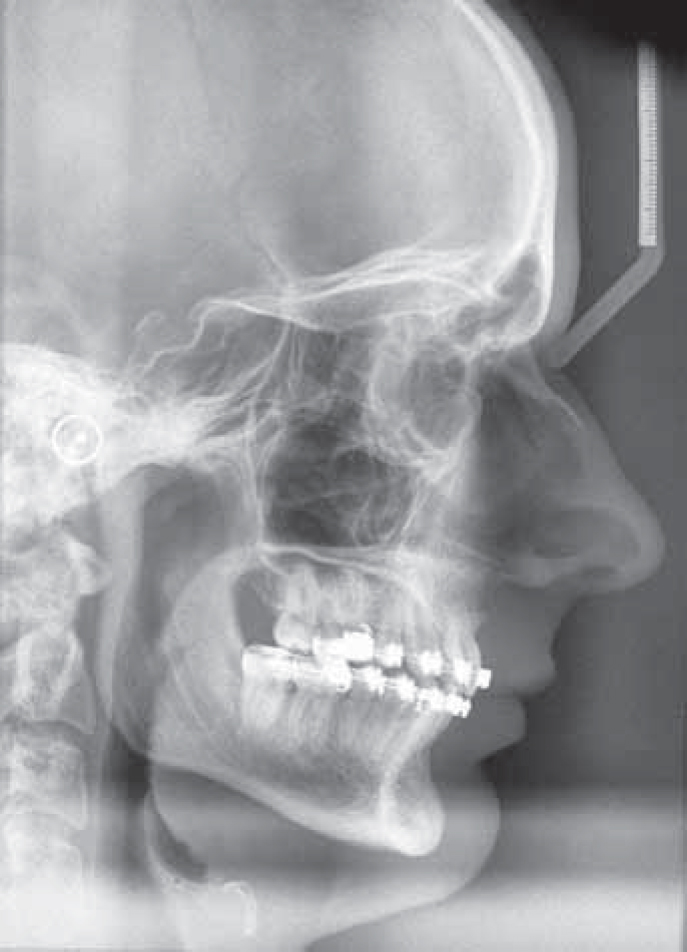
His medical history was unremarkable and neither he nor his mother could recall any episode of trauma to his upper deciduous incisors. A lateral cephalogram and an upper standard occlusal radiograph confirmed that the upper left central incisor had a vestibular root angulation (Figures 3, 4).
Figure 3. Lateral cephalogram illustrating the vestibular root angulation.Figure 4. Upper standard occlusal radiograph illustrating the vestibular root angulation.
In the informed consent discussion, the risks, benefits and prognosis of the following treatment options were discussed:
To extract the upper left central incisor and restore the adjacent lateral incisor to look like the missing tooth;
To extract the upper left central incisor and the first permanent premolars followed by orthodontic fixed appliances to re-open the space so that a prosthetic central incisor could be inserted or, alternatively;
To expose the central incisor surgically and attempt to bring it into the line of the arch using orthodontic traction instead.
Despite the extremely guarded prognosis of the last option, this is the treatment that the patient chose. Treatment therefore began with the extraction of the first premolars, and a pre-adjusted edgewise fixed appliance. After nine adjustments over 13 months, sufficient space had been recreated to accommodate the tooth. Under a general anaesthetic, a labial flap was raised and a bracket with gold chain was bonded to the palatal aspect of the crown of the tooth. A month later orthodontic traction was applied using an elastic that passed through the gold chain, over the fixed appliance archwire and onto a palatal hook of an auxiliary upper removable appliance that provided additional vertical anchorage (Figures 5, 6). Thirteen months and 11 adjustments later, the crown of the central incisor had been brought into the line of the arch (Figure 7) and the mechanics to detail the occlusion and close the residual upper arch spacing then took a further 11 visits over 12 months to complete (Figure 8). In total, 31 adjustments had been undertaken over 41 months to dis-impact the tooth and correct the malocclusion.
Figure 5. Intra-oral view of the upper fixed appliance elastic traction at the stage of the incisor's emergence.Figure 6. Intra-oral occlusal view of the upper fixed and auxiliary removable appliance system of elastic traction.Figure 7. Intra-oral frontal view of the retrieved upper left central incisor.Figure 8. Intra-oral occlusal view of the upper arch space closure near the end of treatment.
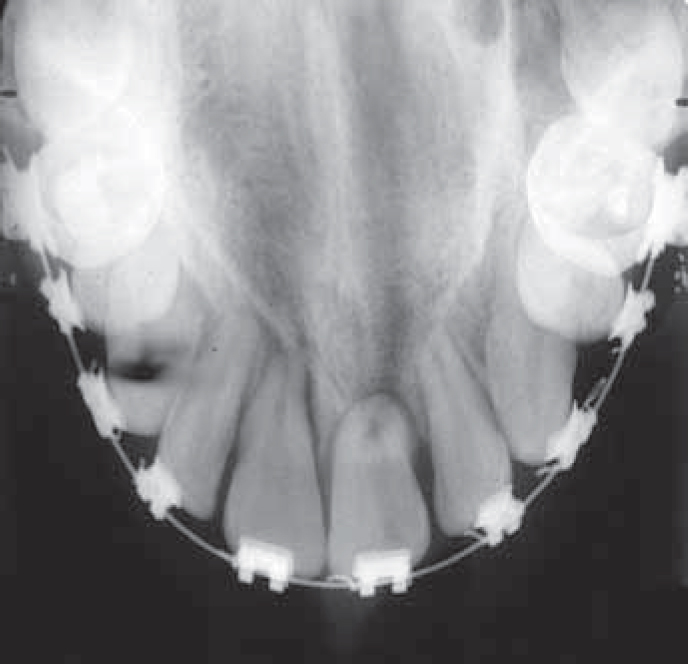
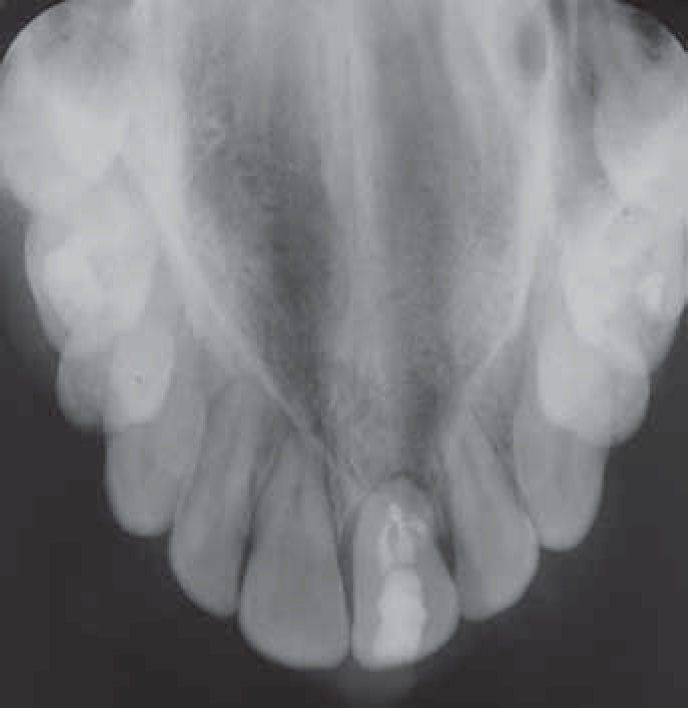
Prior to the removal of the fixed appliances, a fenestration of the labial gingiva by the apex of the central incisor was noted (Figure 9, 10). His general dental practitioner was requested to undertake an orthograde root filling (Figures 11, 12) and a month later the tooth had an apicoectomy and retrograde root filling that was performed through a semi-lunar incision in the unattached gingivae (Figure 13). Subsequent healing was uneventful, with the apex remaining covered by mucosa (Figure 14).
Figure 9. Anterior intra-oral view of the labial fenestration of the upper left central incisor apex.Figure 10. Lateral cephalogram illustrating the perforation of the upper left central incisor apex through the labial alveolar bone.Figure 11. Pre-endodontic upper standard occlusal radiograph.Figure 12. Post-endodontic upper standard occlusal radiograph.Figure 13. Anterior intra-oral view of the apicoectomy and retrograde root filling of the upper left central incisor.Figure 14. Anterior intra-oral view of the post-operative healing.
Discussion
The potential for apices of permanent maxillary central incisors with vestibular root angulations either to impact against buccal plates of alveolar bone4 or to fenestrate labially during their orthodontic recovery has been acknowledged previously.8,9,13,16,23 Once an apex has perforated the buccal bone it can remain covered by the alveolar mucosa, either with14 or without a loss of tooth vitality.17,20 Alternatively, the apex can perforate the labial mucosa and become completely exposed in the mouth, necessitating a combination of orthograde endodontic treatment followed by an apicoectomy, retrograde root filling and closure of the mucosal fenestration defect.15,24
Although the incidence of this complication is rare, there is still a need to discuss it during the taking of informed consent. This is because the duty to inform a patient is not exclusively dependent on the likelihood of a risk, since the standard in case law has begun to shift from the perspective of what a responsible dentist considers is worth disclosing towards combining this with what a reasonable patient might also wish to know.25
In conclusion, it would therefore be good jurisprudence for clinicians who plan to manage similar cases to disclose all possible treatment options and complications in the process of gaining consent.
Summary
This case, of an incisor with a vestibular root angulation whose apex fenestrated the labial alveolar bone and mucosa during orthodontic treatment requiring an apicoectomy and retrograde root filling, would appear to be the fourth such case reported in the English language literature. However, while the incidence of this condition with its possible treatment consequence is quite small, this should not absolve clinicians from the need to discuss details about this potential complication during an informed consent process.