Michi K, Yamashita Y, Imai S, Suzuki N, Yoshida H. Role of visual feedback treatment for defective/s/sounds in patients with cleft palate. J Speech Hear Res. 1993; 36:277-285
Whitehall TL, Stokes SF, Man YHY. Electropalatography treatment in an adult with late repair of cleft palate. Cleft Palate-Cran J. 1996; 33:160-168
Carter P, Edwards S. EPG therapy for children with long-standing speech disorders: predictions and outcomes. Clin Linguist Phonet. 2004; 18:359-372
Mercer N, Pigott R. Assessment and surgical management of velopharyngeal dysfunction. In: Watson A, Sell D, Grunwell P (eds). London and Philadelphia: Whurr; 2001
Hardcastle WJ, Morgan BRA, Clark CJ. Articulatory and voicing characteristics of adult dysarthric and verbal dyspraxic speakers: an instrumental study. Br J Disord Commun. 1985; 20:249-270
Rahilly G, Price N. Current products and practice. J Orthod. 2003; 30:171-174
Ireland A, McDonald F.Oxford, UK: Oxford University Press; 2003
Kelly S, Main A, Manley G, McLean C. Electropalatography and the linguagraph system. Med Eng Phys. 2000; 22:47-58
Murdoch BE, Goozeé JV, Veidt M, Scott DH, Meyers IA. Introducing the pressure-sensing palatograph – the next frontier in electropalatography. Clin Linguist Phonet. 2004; 18:433-435
Murdoch BE. Physiological investigation of dysarthria: recent advances. Int J Speech-Lang Pathol. 2011; 13:28-35
Lohmander A, Henriksson C, Havstam C. Electropalatography in home training of retracted articulation in Swedish child with cleft palate: effect on articulation pattern and speech. Int J Speech-Lang Pathol. 2010; 12:483-496
Nordberg A, Carlsson G, Lohmander A. Electropalatography in the description and treatment of speech disorders in five children with cerebral palsy. Clin Linguist Phonet. 2011; 25:831-852
Cleland J, Timmins C, Wood SE, Hardcastle WJ, Wishart JG. Electropalatographic therapy for children and young people with Down's syndrome. Clin Linguist Phonet. 2009; 23:926-939
Hartelius L, Theodoros D, Murdoch B. Use of electropalatography in the treatment of disordered articulation following traumatic brain injury: a case study. J Med Speech-Lang Pathol. 2005; 13:189-204
Howard S, Varley R EPG in therapy: using electropalatography to treat severe acquired apraxia of speech. Eur J Disorder Comm. 1995; 30:246-255
Goldstein P, Ziegler W, Vogel M, Hoole P. Combined palatal-lift and EPG-feedback therapy in dysarthria: a case study. Clin Linguist Phonet. 1994; 8:201-218
Lee AS-Y, Law J, Gibbon FE. Electropalatography for articulation disorders associated with cleft palate. Cochrane Database of Systematic Reviews. 2009; (3) https://doi.org/10.1002/14651858.CD006854.pub2
Improving speech disorders using electropalatography: applications, technical aspects and manufacture of the appliance Renny Talbot Dirk Bister Orthodontic Update 2025 6:2, 47-50.
Authors
RennyTalbot
City and Guilds Certificate in Dental Technology, Advanced Orthodontic Certificate, Advanced Max-fac Certificate, Outpatient Department, Addenbrooke's Hospital, Cambridge, London, UK
This paper describes applications of electropalatography (EPG) and the stages of laboratory construction. EPG is thought to be useful for improving speech of cleft lip and palate patients because it gives a direct visual feedback of tongue-to-palate contact allowing patients to alter tongue position, ideally leading to an improvement of their speech.
Clinical Relevance: Electropalatography is a clinical technique utilized to improve speech in cleft lip and palate patients. It allows patients and speech and language therapists to visualize the placement of the tongue within the oral cavity. This technique helps to correct abnormal articulations by adopting normal patterns for consonants or vowels that patients find difficult to pronounce.
Article
The benefits of EPG have been well documented in the past.1,2,3 Speech is produced by complex co-ordination of multiple muscular systems and multiple components in the head and neck region. The nose, lips, tongue, larynx and pharynx all contribute to good speech articulation. Speech disorders are usually multifactorial and the causes are usually divided into developmental or acquired, neurological and physical. In cleft lip and palate (CLP) patients physical and developmental factors are the main causes and velopharyngeal insufficiency (VPI) is a common presenting feature.4
Articulation and quality of speech are usually assessed separately by speech and language therapists (SLTs), however, intra-oral assessment of the tongue-to-palate contact during active speech can be difficult, hence the use of EPG.
Dysarthria is not specific to CLP but can also be a presenting feature in Down's syndrome, patients with hearing impairments and cerebral palsy. In all these instances, EPG can be applied with positive outcomes. Equally, in adults it can be used for patients who experience traumatic brain injuries (TBI) or suffer from Parkinson's disease.
The aim of this article is to:
Raise awareness of this highly sophisticated technique;
Describe the laboratory procedures involved;
Review the existing evidence in the literature of its effectiveness;
Electropalatography
An EPG is an orthodontic/electronic device which is coupled with a portable display portraying the spatial positioning of the tongue against the palate for phonetic articulation. It can also be used to document positional changes of their special relationships, following assessment and training by a SLT.
The appliance, which is usually made by a qualified maxillofacial technician, consists of an orthodontic appliance, in which electrodes are embedded, that act as sensors to detect the motion of the tongue during speech.5 The electrodes relay the information to a portable electronic display unit which graphically demonstrates the area of tongue in contact with the palate.
The appliance is made of acrylic and extends just anterior to the junction between the hard and soft palate. Retention is tooth- and tissue-borne, including clasps and suction from the palate.
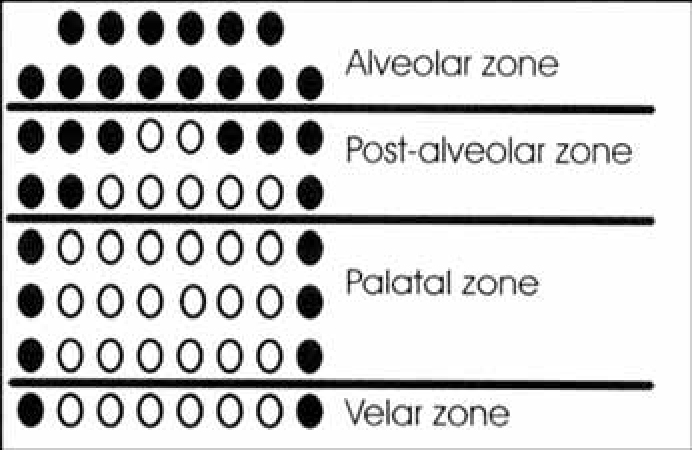
A typical diagrammatic representation on the visual display unit is shown in Figure 1. It is divided into four zones in order to facilitate localization of tongue-to-palate contact. This enhances the assessment by the SLT in order to direct the patient to make appropriate changes in position.
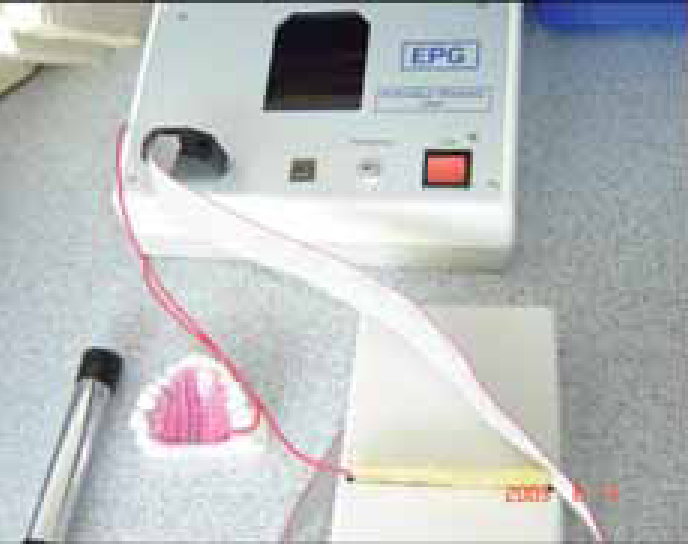
Figure 2 is an actual image of the electronic display on the control unit, displaying activity.
Figure 2. A modern control unit showing that the tongue is in contact with the left half of the palate during speech.
Laboratory construction
The construction of the appliance starts after casting the alginate impression of the upper arch in plaster. Alginate has good replication qualities and is easy to use.6 The plaster model is made using ISO Standard for Dental Gypsum products Type III.7
The EPG plate consists of three layers:
The baseplate with the retention elements;
The intermediate layer with the electronic contacts and wires; and
The palatal layer of acrylic that contains the contacts on the tongue side.
The first step in the process is the fabrication of modified Adams clasps, usually using 0.7 mm stainless steel8 with an 18:8 chromium to nickel ratio. This formula gives the stainless steel enough rigidity whilst decreasing the likelihood of inducing an allergic reaction.9 The Adams clasp has the following features: a connecting bridge between the two arrowheads incorporating the undercuts of the two first permanent molars and a loop which is placed in the central region of this bridge. The clasp is double in size and spans the first permanent molar and second premolar (or second deciduous molar) on the ipsilateral side.
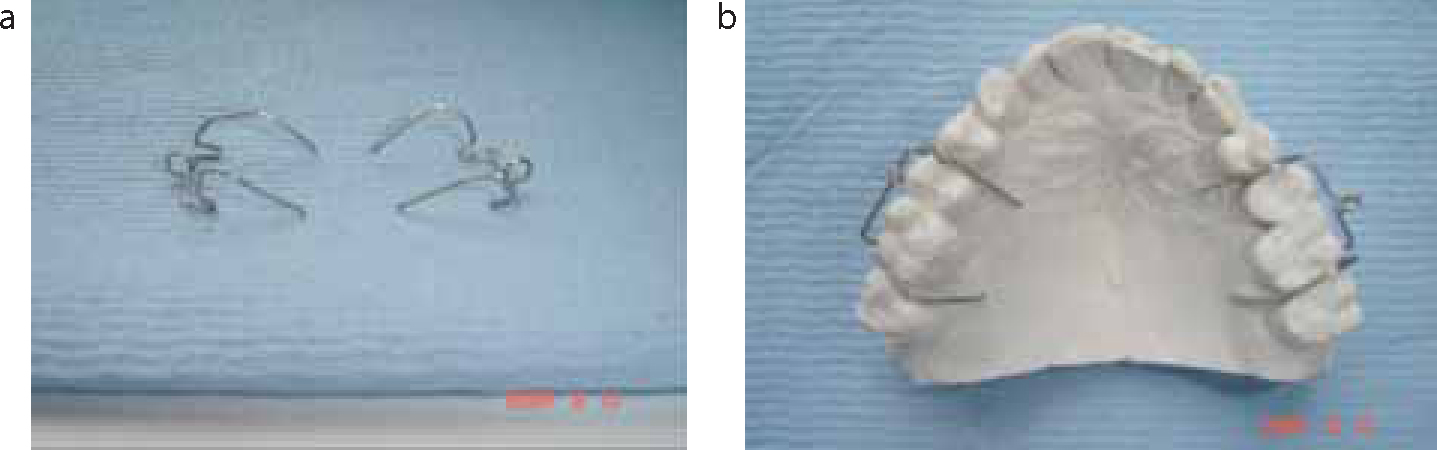
The clasps are checked for a precise fit and the tags extend approximately two-thirds of the depth of the palatal sulcus. The occlusal portion of the tags should lie as close as possible to the contact between the teeth (Figure 3).
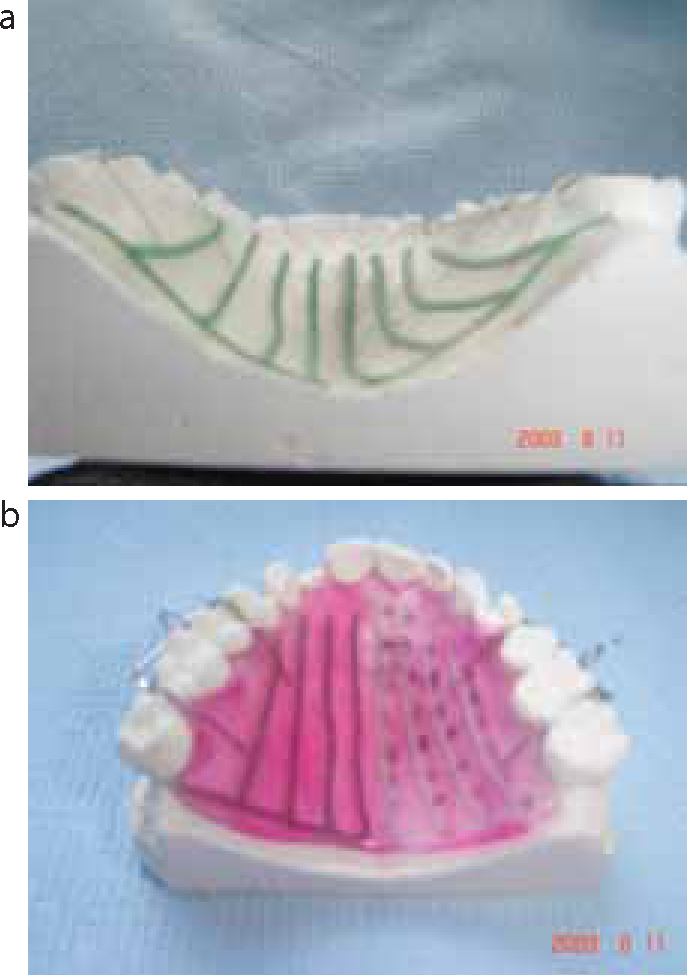
Figure 3.
(a, b) Modified double Adams clasps and plaster model.
A clear baseplate using cold-cure acrylic is manufactured using the ‘salt and pepper’ technique after clearly demarcating the antero-posterior extent on the plaster model. The baseplate should be approximately 1–1.5 mm thick (Figure 4). For polymerization, the appliance is placed in a hydroflask for approximately ten minutes at a temperature of 40–50°C. The pressure in the hydroflask is usually set to 130 kPa. These conditions reduce the number of voids in the acrylic and increase the strength of the appliance.10
Figure 4. Construction of upper removable appliance.
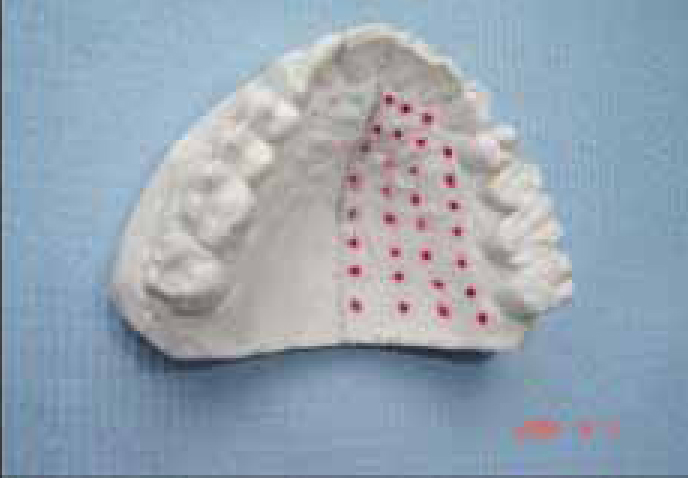
The plaster model is divided into left and right halves and is then marked for the placement of the electrodes using a pen which shows through the transparent hue of the acrylic (Figure 5).
Figure 5. Plaster model marked for future placement of electrodes.
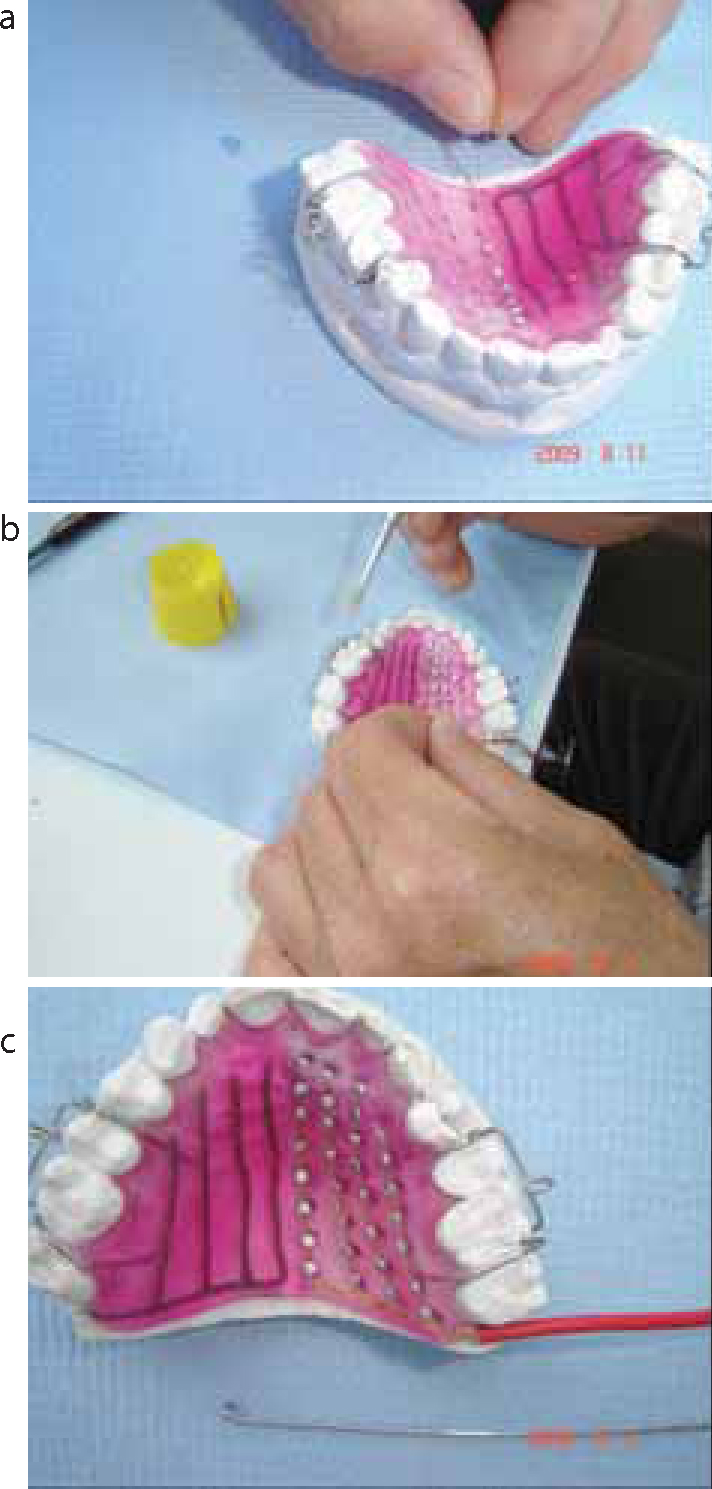
Wax wires 1 mm thick are added to the two halves of the model and connected posteriorly (Figure 6a). These wax wires will act as channelling ducts through which the electrodes will be passed later. A very thin layer of coloured cold-cure acrylic is then placed over the initial plate, adding acrylic in between the wax channels (Figure 6b on the left), leaving them exposed on the palatal aspect. Once the plate is polymerized, the wax is boiled out (Figure 6b on the right) and the grooves are left exposed for positioning of the electrodes. The electrodes are placed into the voids, allowing the wire connecting to them to be guided via the channels to the posterior border of the plate (Figure 7). The electrodes are fixed into position using a contact adhesive. At this stage the electrodes need to be tested and non-functional elements are replaced.
Figure 6.
(a) Channels of wax connected posteriorly and (b) placement of coloured acrylic.Figure 7.
(a-c) Positioning, securing and sleeving of electrodes.
The last step of the manufacture of the plate involves covering its palatal aspect, thereby filling the residual void of the grooves. The salt and pepper technique is used to add this final layer of the cold cure acrylic and great care has to be taken so that the electrodes are left exposed palatally, but not the wires. The palatal aspect of the plate is finally pumiced and polished and all the wires exiting the plate at the posterior border have been sleeved for both right- and left-hand sides. The sleeved wire is passed though the loop of the crib.
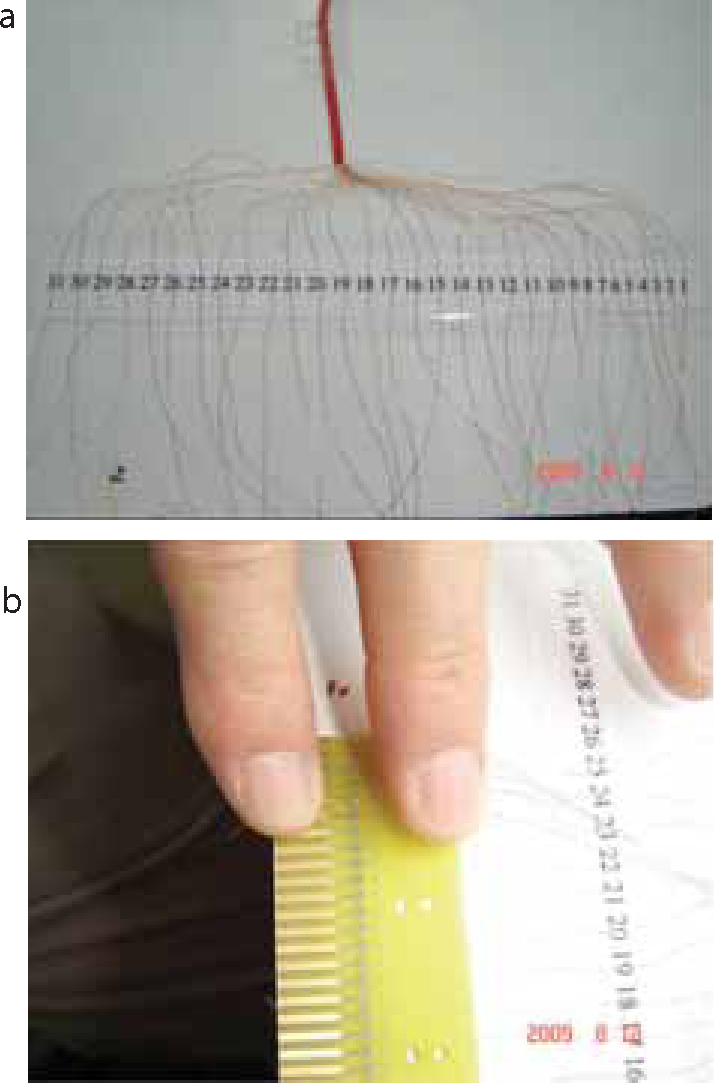
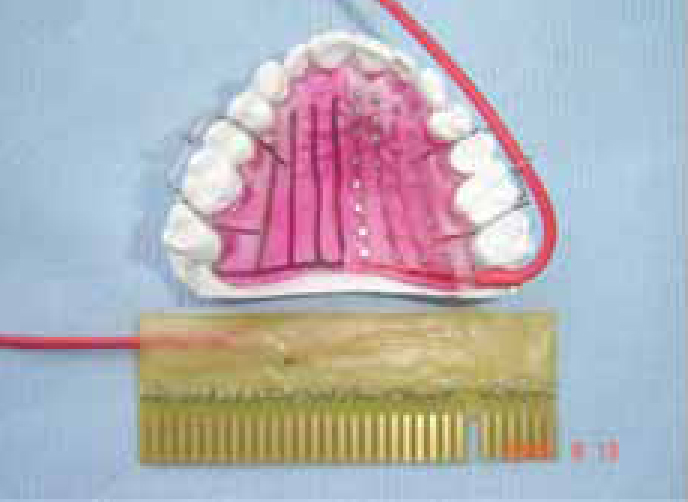
The distal ends of the wires emerging from the sleeve need to be long enough so that they can be soldered to the circuit board at the end of the manufacturing process (Figure 8). Also, the wires need to be identified correctly so that they are matched to their allocated number on the plate and circuit board. This is ensured by checking with the continuity electric tester. Figure 8a shows the allocation of each electrode prior to soldering the wires to the circuit board. There are 31 electrodes per side. A close-up photograph of a completed plate is shown in Figure 8b. Finally, the completed unit is connected to the portable unit and tested before clinical use (Figures 9 and 10).
Figure 8.
(a, b) Individual numbering of electrodes and soldering to the circuit board.Figure 9. The finished plate and circuit board.Figure 10. The completed EPG unit, connected to the portable unit.
Alternative techniques and evidence
Kelly et al provide extensive documentation of alternative techniques of EPG.11 Most of these are variations of the plate we have described above, and include the following:
Rion DP-01 Electropalatograph System;
Kay Palatometer System;
Reading System (EPG2, EPG3 and EPG4);
Linguagraph System.
More recent modifications of these appliances include pressure-sensing EPG12 and visualization in 3-dimensions, such as 3D-EMA and 3D-EPG.13
The above systems try to overcome limitations of the 2-D displays of older systems. The latter allowed for misinterpretations of the tongue-to-palate contact; they did not account for variations in the anatomy of the palate, such as high-arched palatal vaults or increased distances between sensors and contact areas.
Another comprehensive review of the EPG literature between 1957 and 2005 is by Gibbons.14
There are numerous case reports confirming the efficacy of EPGs. Lohmander et al found an improvement in articulation after just eight hours of home training, utilizing a modern portable unit in a Swedish child with cleft palate.15 Similar findings were also reported in a Swedish case study of children with cerebral palsy.16 Cleland et al suggest that the benefits of this apparatus can also be applied to children and young people with Down's syndrome.17
Several studies also extend the benefits of EPG to adults with acquired speech disorders. Hartelius et al described a case report of a 30-year-old male with spastic-ataxic dysarthria improving in both the word and sentence intelligibility.18 Howard and Varley19 and Goldstein et al,20 similarly, demonstrated successful outcomes. In summary, EPG can be utilized to treat a multitude of speech disorders of different aetiologies and their use is not restricted to patients affected by cleft lip and palate alone.
In contrast to the numerous case reports describing good speech improvements utilizing EPG, a recent Cochrane review concluded that most of the existing evidence of their effectiveness is weak and that studies utilizing controls are needed to prove their efficacy.21
Conclusion
Managing dysarthria in CLP is complex and appropriate management requires the adoption of a multidisciplinary approach by a number of specialists. The use of EPG has been shown to be beneficial in case reports and it appears to be an effective tool in treating patients with dysarthria of numerous aetiologies.