How can we improve orthodontic care for patients with autism and/or learning disabilities? Pamela E Ellis Sarah Silverton Lorna Hollingsworth Orthodontic Update 2025 9:1, 15-22.
Authors
Pamela EEllis
BDS(Hons), FDS RCS, MSc, MOrth RCS, FDS(Orth) RCS
Consultant Orthodontist, Dorset County Hospital NHS Foundation Trust, Williams Avenue, Dorchester, Dorset, UK
Sedation and Pain Management PG Cert, MSc, Associate Clinical Director/Specialist Special Care Dentistry, Somerset Partnership NHS Foundation Trust, Bristol Road, Bridgwater TA6 4RN, UK
Receiving orthodontic care can be challenging for our patients with autism and/or learning disabilities; being in new places, meeting new people and having treatment can be overwhelming. In this article the authors have worked with carers to understand better the challenges patients with autism and/or learning disabilities face and identify reasonable adjustments which can be made to improve their experience. It is hoped that other orthodontists may adopt these changes in their own services or find similar ways to improve the care of this patient group.
Clinical Relevance: Orthodontists encounter patients with autism and/or learning disabilities in their day-to-day practice. This paper outlines reasonable adjustments they can make to improve the experience of these patients.
Article
In a previous project using an experience-based design (ebd) approach to measure patients' experiences, the authors were surprised at the high numbers of patients who experience negative emotions at their orthodontic consultation appointment; 39% of patients attending a consultation appointment felt nervous, anxious or unwelcome at some point in their journey.1 Whilst carrying out this work the authors became aware that, in particular, patients with autism and/or learning disabilities can find attending orthodontic appointments challenging; being in new places and meeting new people can be overwhelming and some patients find this so difficult that they are unable to come to what we perceive as a ‘routine’ orthodontic assessment. Others, although they manage to attend clinics, find it difficult to cope with the sights, sounds, smells, lights and colours within surgeries, or the tastes and textures of the instruments, materials and appliances used in their mouths.
Autism affects how a person communicates with, and relates to, other people. It is a spectrum disorder which means that, while all people with autism share certain difficulties, their condition will affect them in different ways.2 Autism is also often associated with learning disabilities and, according to NHS Information Centre statistics, approximately 1% of the population has an autistic spectrum condition and 60–70% of people who have an autistic spectrum condition will also have a learning disability.3 A learning disability is a significantly reduced ability to understand new or complex information, to learn new skills and the reduced ability to cope independently.4 Patients with autism alone, learning disabilities alone, or a combination of autism and learning disabilities, all face challenges when receiving orthodontic care, whether this is in communicating with the orthodontist and other members of the team, understanding treatment, or tolerating care and, for this reason, all three groups were included in this project.
There has been an increase in recognition of autism in recent years (in 2009–2010 the number of children known to schools with autism in England was 7 per 1000 of the population but this had risen to 9.1 per 1000 in 2013–2014).5 Similarly, the number of people recognized with learning disabilities is also rising (it is estimated that there are 286,000 children age 0–17 years in the UK with a learning disability).5 Consequently, with this increased recognition within the general population, orthodontists are likely to encounter greater numbers of patients with these conditions in their day-to-day working. This can be difficult as most orthodontists see a high volume of patients and the additional time and adjustments for these patients can be disruptive to clinics. However, it is a statutory requirement under the Equality Act 2010 that public sector agencies make ‘reasonable adjustments’ to their practices that will make them as accessible and effective for people with as without disabilities. Reasonable adjustments include removing physical barriers to accessing health services but, importantly, also include making whatever alterations are necessary to policies, procedures, staff training and service delivery to ensure that they work equally well for people with autism and/or learning disabilities.
For some patients their autism and/or learning disabilities may be so severe that they would be unable to wear and care for orthodontic appliances. For some of these patients the orthodontist can still provide useful advice in the planning of elective extraction of primary or permanent teeth with the aim of improving dental health and aesthetics. Here reasonable adjustments can focus on improving the user-friendliness of a consultation. For other patients with less severe autism and/or learning disabilities, reasonable adjustments can focus around the delivery of treatment.
The aims of this project are to explore the challenges that patients with autism and/or learning disabilities face in receiving orthodontic care; then working with patients and carers to identify reasonable adjustments that can be made to improve their experience of care.
An experience-based design (ebd) approach was used as a framework to structure this qualitative project.6 The ebd approach uses co-design between staff, patients and carers for service improvement in a continuous cycle of capture, understand, improve and measure. It differs from traditional patient satisfaction surveys in that a patient's journey through a service is mapped (eg seeing the orthodontist for the first time, having x-rays taken, attending for treatment, etc). The patient's emotions are captured at each of these contact points. By then examining why the patient felt the way he/she did at each part of the journey, ways to improve the service can be identified. Finally, by interviewing patients and carers after the service improvements had been made, their effectiveness could be evaluated. The ebd approach was chosen as it has already been used successfully to improve patient experience in an orthodontic service.1
Method
The ebd questionnaire
The first step of the ebd approach was to capture patient experience. This was done by developing questionnaires for patients with autism and/or learning disabilities and their carers. Because of the low number of patients with autism and/or learning disabilities accessing the service at that time, the questionnaires were supplemented with carer stories. Carer stories are semi-structured interviews with carers which are a rich source of qualitative data. On the advice of carers, interviews with patients were not conducted because patients with autism and/or learning disabilities would have found it too challenging to take part in a one-to-one interview by themselves. The interview guide from the ebd approach guide and tools was followed.6 Although the NHSIII has now closed, guidance and toolkits can still be found on their website (www.institute.nhs.uk) and, in future, on The National Archives website (www.nationalarchives.gov.uk/) The authors explored with the carers their experience and the patients' experience of orthodontic care. This enabled them to express what had been challenges and what had been successes in the orthodontic care, from the perspective of both the carer and the patient, particularly relating to the feelings and emotions that they had.
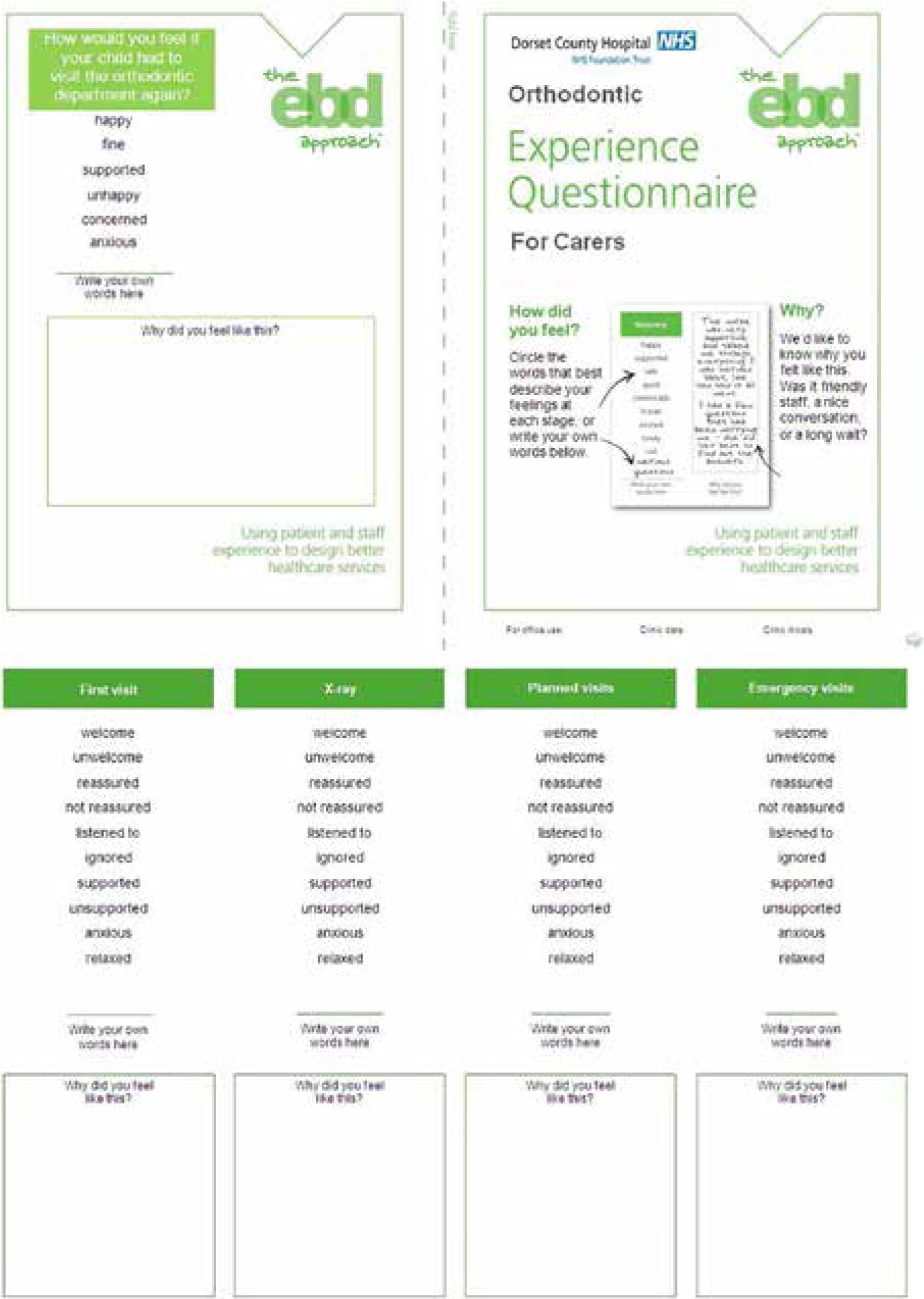
The ebd questionnaire for carers was created by mapping the journey of orthodontic care (first visit, x-ray, planned visits and emergency visits) and then identifying emotions appropriate to the carers of patients with autism and/or learning disabilities. These emotions were identified by asking members of a local learning disabilities support group to complete a poll. The emotions voted most applicable were welcome/unwelcome, reassured/not reassured, listened to/ignored, supported/unsupported, anxious/relaxed (Figure 1).
Figure 1. The ebd approach questionnaire adapted for carers of orthodontic patients with autism and/or learning disabilities.
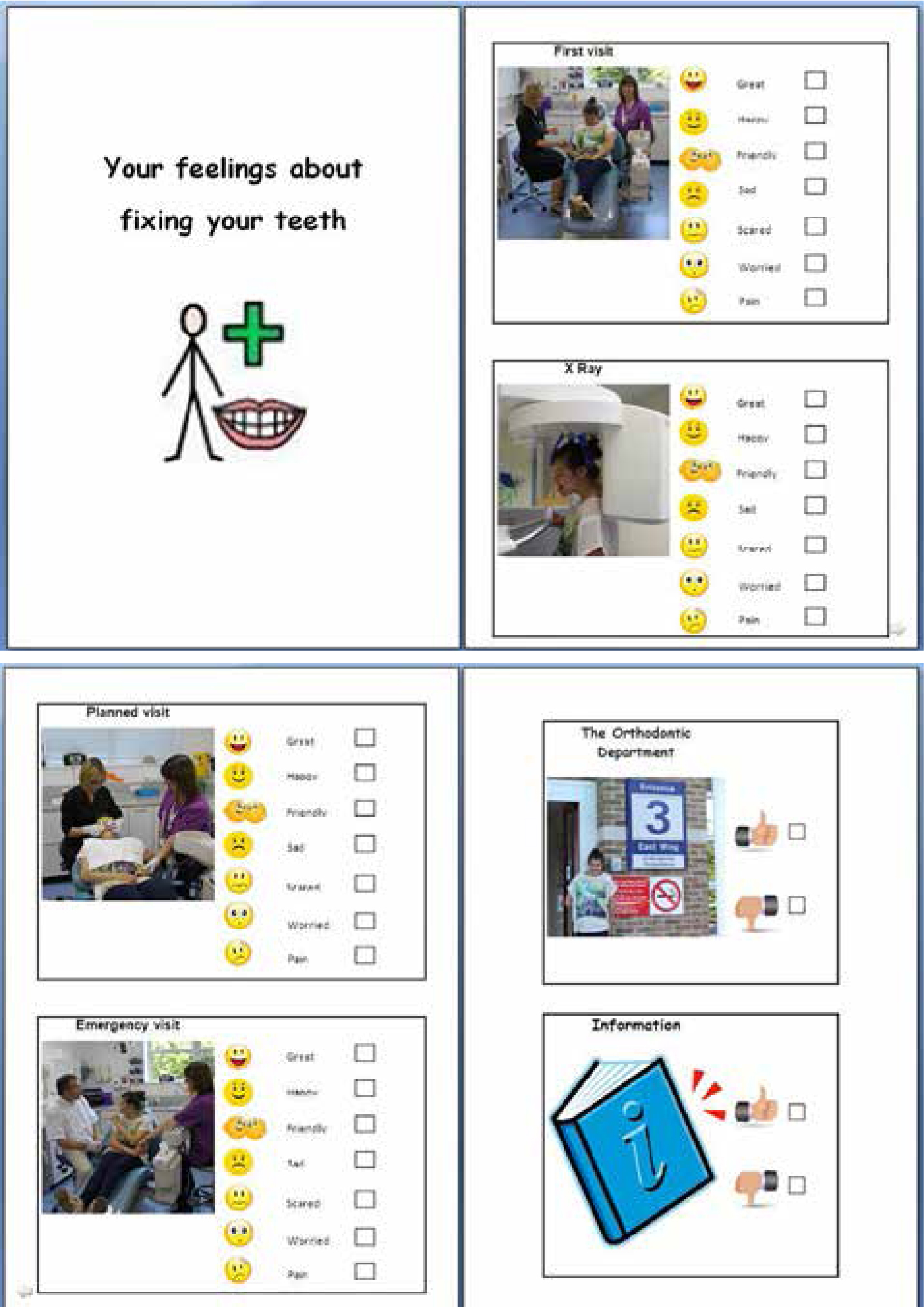
The questionnaire for patients with autism and/or learning disabilities echoed the patient journey used in the carer questionnaire. It was then modified to include pictures taken in the department of our staff and a volunteer patient and carer. Emoticons were used in addition to a written list of emotions (Figure 2). The questionnaires were distributed to 15 patients and 15 carers in June 2014.
Figure 2. Questionnaire adapted for orthodontic patients with autism and/or learning disabilities.
Understanding the patient experience
The second step of the ebd approach is to understand patient experience. A ‘listening event’ was organized where patients, carers, staff and commissioners met to explore these key issues identified in the carer stories and questionnaires and suggested ways to improve the experience of all concerned. Following the listening event the authors were able to map the key issues and the reasonable adjustments that could be made to the patient's journey; this is summarized in Table 1.
Issue
Suggested solution(s)
Before Coming
We don't know which of our patients have autism and/or learning disabilities
Ask the referring dentists to tell us this in their referral letter
Add a paragraph to our initial appointment letter asking the carer to get in touch
We don't know what specific issues or needs the patient has
Phone carer before appointment
Use the Trust's care passport
Arriving
Being in new places is stressful
Arrange visit beforehand at quiet time
Develop social stories which will include photos of waiting areas, surgeries and equipment
Encourage carers to come in and take their own pictures if this helps
Develop a ‘sound gallery’ with sounds like the suction or the drill and make this available on our website
Seeing new people is stressful
Display photos of staff in our waiting area and on our website
Customize the social stories with pictures of the clinician and nurse that they will see
Develop a ‘Hello from staff’ video for YouTube
Waiting
Not being seen on time can be very stressful
Give patients the first appointment slot in the morning or after lunch
Suggest carers tell children that their appointment time is 30 minutes later (in case clinic is running behind)
Keep patients and carers updated if clinics are running behind. Offer to phone them on their mobile when the clinician is free
Music playing in the waiting area can be too much
Reception staff to turn off the music if needed
It can be difficult to wait with other people
Identify a quiet area to wait and make carers aware that this is available
Being Seen
Carers sometimes don't want to discuss issues in front of their children
Offer to chat to carers on their own. Arrange to call the carer before the initial appointment if this is of value
Too many instructions are overwhelming
Keep instructions short and clear. Make one point at a time
Instructions/discussions can be confusing
Talk literally, say exactly what you mean. ‘Sit down’ rather than ‘come and take the weight off your feet’
Having to talk to others can be overwhelming
Find out the patients' preferences. They may prefer all discussions to be carried out with the carer only
Routine Visits
Often need more time for appointments
Book longer appointment slots
Even routine procedures can be stressful
Develop social stories for each procedure, eg impression-taking, photographs, fitting braces, removing braces
Explain what is happening. Agree stop signals. Use action prompts, eg thumbs up/thumbs down
Explain what will happen next time. Prepare them for the next visit, for example allow them to take an impression tray away
Seeing different staff can be stressful and at worst impossible
Find out patients' preferences and highlight in notes. It may be better to delay an appointment when a clinician is unavailable rather than to squeeze a patient in with someone else
Carers don't want to feel they are bothering us
Make ourselves available to chat
Use kind words and show understanding
Other Actions
Organize training for staff in how to communicate effectively with patients with autism and/or learning disabilities
Improving services
The third step in the ebd approach is to improve services. The orthodontic team met to review the issues listed in Table 1 and to plan how the adjustments could be implemented by the team. Many of the adjustments required little or no resource and could be immediately implemented. Examples include: booking longer appointment slots and offering the first appointment of the morning or afternoon; turning off the music if this was too disturbing or directing patients to a quiet waiting area when required.
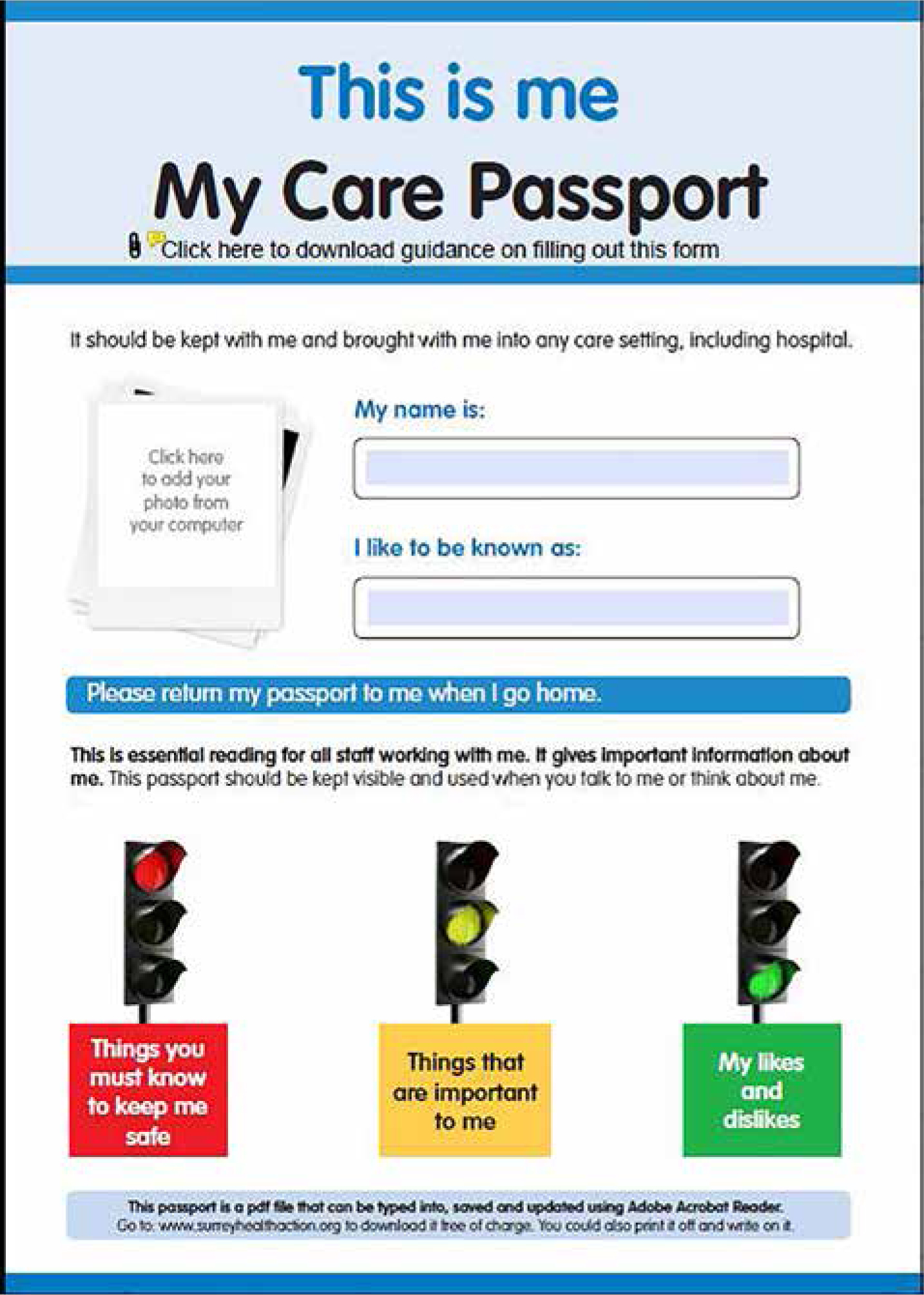
Other actions required little resource but some planning was needed around implementation, for example ‘Care Passports’ (Figure 3) were already in use at our hospital but our challenge was to identify who would be responsible for giving these to the patient and how to find the time to review the care passport before seeing the patient.
Figure 3. A ‘Care Passport’ which documents the care requirements of patients with autism and/or learning disabilities.
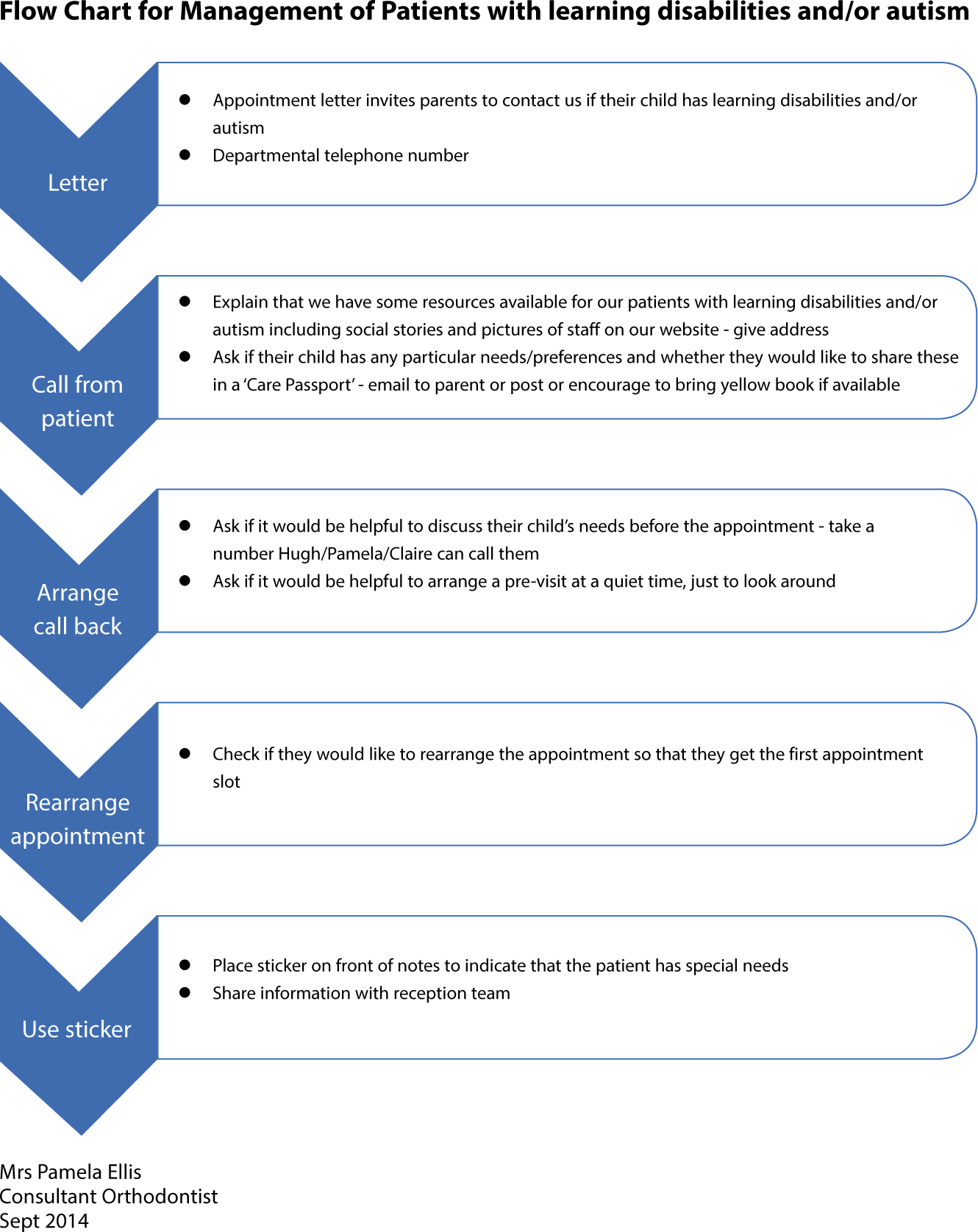
In order to implement this and other actions, like offering carers a telephone chat with the clinician, seeing patients before their first assessment, we developed a flow chart for our administrative team to follow (Figure 4).
Figure 4. Flow chart for our administrative team to follow.
Other adjustments required more time and resource to organize. An example of this was ‘social stories’ which showed patients, through pictures, simple text and symbols what the department looked like, who they would meet, what equipment would be used and what would happen at their appointment. The authors developed individual social stories for each clinician who carried out new patient consultations so that patients could familiarize themselves with people and places before their first visit. The authors have paper copies of these social stories (Figure 5) available to post out but, more commonly, patients access the information online before their appointment (www.dchft.nhs.uk/patients/departments-G-O/orthodontics).
Figure 5. An example of one of our ‘social stories’.
Another important action has been to set up an Orthodontic/Special Care Dentistry joint clinic. Staff felt that this clinic would be valuable in improving access to patients whose learning disabilities were too great to be able to cope with an orthodontic treatment, but who would benefit from an orthodontic opinion regarding extraction choices. We also perceived that this joint clinic may also be of benefit as a first step in starting orthodontic care for patients with autism and/or less severe learning disabilities; seeing the orthodontist in a familiar environment (the Special Care Dentistry department) might ease the transition to attending the orthodontic department eventually. When we explored the possibility of a joint clinic at the listening event, patients and carers were unanimous in their support for this clinic as a positive step towards improving patient experience. This was an opportunity to use patient and carer input in the co-design of this clinic, taking on board patient and carer preferences for the location of the clinic, the length and timing of appointments and the structure of the joint consultation. This new clinic required both time and resources, but the feedback from the discussion groups at our listening event added weight to the business case to introduce this clinic.
Evaluating success
The response rate to the patient and carer questionnaire was low; only three patients and three carers returned their questionnaires. The authors therefore concentrated on carer stories to measure whether the adjustments that had been made had improved patient experience.
A common theme from the carer stories was the importance of scheduling appointments appropriately and being seen quickly. One carer explained that her son with autism ‘is not good at waiting and paces around’, so having an early appointment and being seen quickly reduced stress. Another carer commented that being seen quickly was important to the patient who had Asperger's Syndrome and expressed her gratitude for being seen quickly on arrival.
Identification of a quiet waiting area also improved experience. One carer explained that the patient ‘is not good with noises, high pitched sounds and, in particular, young children’. It improved their experience to have a quiet area where they could sit if necessary and they appreciated being seen quickly each time.
Taking extra time at each appointment was also successful. A carer explained that the patient ‘is very sensory orientated and needs to look, touch and feel things. The orthodontist took time to explain what she was going to do before she did anything. When he (the patient) had the mould he saw it and touched it and there were no problems with it’. Another carer commented ‘I believe they took her (the patient's) Asperger's into account and took time to explain her treatment. They treated her like a young adult and didn't talk down to her like a baby, which often happens when people know she has additional needs. They dealt with her clearly and factually and firmly when needed which is exactly what she needs’.
The value of providing information to prepare patients for each visit was also highlighted in the carer stories. Although none of the parents interviewed had accessed the social stories before the patient's appointment, they commented how valuable it had been when the orthodontist explained what would happen at the next appointment before they left.
Discussion
Although efforts were made to adapt an experience-based design questionnaire to patients with autism and/or learning disabilities (by including photographs of the actual department, emoticons and emotions selected by a learning disabilities support group), the low response rate to the questionnaires used at the beginning of this project demonstrates the difficulty in designing questionnaires for patients with spectrum disorders. One patient commented that the questionnaire was ‘babyish’ and he did not fill it in because it was not relevant to him. In addition, other patients and carers explained that they had not returned the questionnaire because they were happy with care. It could also be argued that asking an experience-based design approach, which focuses on emotions, may be inappropriate for autistic children who often have difficulty in expressing emotions. The authors therefore found carer stories a more valuable tool for capturing patient and carer experience. Carer stories were a rich source of information which allowed the authors to identify common themes and start to understand the areas of care where experience could be improved. The listening event allowed consolidation of this learning process and exploration of these areas further with a view to identifying reasonable adjustments that could be made.
A limitation of this project was that the issues and reasonable adjustments identified were based on a small number of patients and carers. However, because autism and learning disabilities are spectrum disorders, even a large sample of patients would not identify all of the issues and reasonable adjustments for this group. An important learning point is that orthodontists need to deliver person-centred care by identifying each individual's preferences early. By asking carers to make contact before the patient's initial assessment, and by using care passports, the reasonable adjustments which need to be made can be planned for each individual. The authors were pleased by the enthusiastic response from patients and particularly carers to this part of the project. On occasion carers were reduced to tears when describing their experience in other parts of the health service. Talking to the carers made the authors appreciate the considerable effort that they put into ensuring that patients attend appointments. This included preparations a week in advance using social stories; repeating information about going to see the orthodontist; time spent on the day of the appointment persuading and convincing the patient to attend. This made the authors consider as a department how much care was given to the carers, and how important this aspect of a patient's journey is. They were also pleased by the enthusiasm of staff for the project; both their ability to accept that the service provided was less than perfect and their willingness to adopt changes to improve the service.
The authors have found that the social stories they developed have been of value not only to their patients with autism and/or learning disabilities but also have been particularly useful to young or nervous patients using their service. Patients have commented on how knowing who they were going to see and exactly what would happen at their consultation appointment made this appointment easier.
Previous authors have outlined behavioural management techniques to aid orthodontic management of patients with autism. These include ‘tell-show-do’ storyboards (a type of social story) and use of symbols.7 The authors also advocate distraction techniques including head-mounted displays (audio-visual glasses). Although these have not been introduced, the authors have started to identify, through their care passports, those patients who use gaming devices (for example, iPads or Nintendo hand-held consoles), encouraging them to use these familiar devices to reduce anxiety whilst waiting.
The work the authors have carried out is transferable to orthodontic providers in both hospital-based services and specialist orthodontic practice. The issues outlined in Table 1 will be common to many other orthodontic providers. Although some of the actions or reasonable adjustments outlined in Table 1 are specific to this service, others could be adopted by other providers or adapted so that they work locally, for example, care passports are readily available; any orthodontist with access to a camera can develop social stories; we can all take a little extra time with carers and patients with autism or learning disabilities to reduce anxiety.
Conclusions
The experience-based design approach has been an effective tool in helping us capture, understand and improve patient care in a group of patients with autism and/or learning disabilities and their carers.
It is possible to make service improvements which improve the experience of orthodontic care with minimal financial resource.