Chadwick SM, Banks PA, Wright J The use of myofunctional appliances in the UK: a survey of British orthodontists. Dent Update. 1998; 25:302-308
Clark WJ The twin block traction technique. Eur J Orthod. 1982; 4:129-138
Bainbridge M An audit of lower incisor proclination using a modified twin block appliance. Br Ortho Soc Clin Effect Bull. 2010; 25:9-11
Allwork J An Audit into Lower Twin Block Design and Fractures: 2004.
Dixon M, Jones Y, Mackie IE, Derwent SK Mandibular incisal edge demineralization and caries associated with Twin Block appliance design. Br J Orthod. 2005; 32:3-10
Stecksén-Blicks C, Renfors G, Oscarson ND, Bergstrand F, Twetman S Caries-preventive effectiveness of a fluoride varnish: a randomized controlled trial in adolescents with fixed orthodontic appliances. Caries Res. 2007; 41:455-459
Kinirons MJ, Stewart C Adolescents' knowledge of common foods and drinks and the importance of the pattern of consumption: a study undertaken in an area of high dental needs. Community Dent Health. 1998; 15:175-178
Westman JC The impact of divorce on teenagers. Clin Pediatrics. 1983; 22:(10)692-697
Extensive decalcification of the permanent dentition following long-term, unmonitored, functional appliance wear: case report William Fitzpatrick Elizabeth O'Sullivan Orthodontic Update 2025 5:3, 90-92.
Authors
WilliamFitzpatrick
BChD(Leeds), MFDS RCSEd, DDHS LM FGDP(UK)
SHO in Maxillofacial Surgery, Hull Royal Infirmary
We present the case of a healthy 14-year-old female who was referred urgently by her general dental practitioner (GDP) to a consultant paediatric dentist regarding extensive decalcification of her permanent dentition. The patient had commenced orthodontic treatment 18 months earlier with a twin block appliance. She had worn this appliance unremittingly, despite failing to return for follow-up treatment.
Clinical Relevance: The importance of regular dental review and early detection of decalcification in patients undergoing functional appliance therapy is discussed.
Article
The twin block appliance is now the most frequently used myofunctional orthodontic appliance in the UK.1 The mechanism of action involves inducing a functional mandibular displacement, in order to produce an intermaxillary reaction.2 This appliance is usually fabricated from an acrylic base-plate material, which sometimes incorporates lower incisor capping, which has the benefit of reducing the appliance's lingual bulk and visibility, whilst eliminating retention clasps which are prone to fracture.3,4 Recent literature demonstrates the detrimental influence of incisal capping with concomitant regular intake of carbonated soft drinks.5
Functional appliance therapy
The majority of practitioners advise the full-time wear of a twin block appliance to maximize benefit. However, a twin block design can have detrimental effects on the dentition. It remains in direct contact with the dental tissues for prolonged periods of time, potentially increasing plaque retention and the risk of demineralization by reducing the self-cleansing and neutralizing actions of saliva. It is therefore important that the orthodontic team examines the dentition at each visit for signs of demineralization. At the first sign of demineralization, tooth-brushing and dietary instruction should be reinforced, a daily fluoride mouthwash prescribed and topical fluoride varnish applied.6 This may help to arrest demineralization and encourage remineralization.
Case history
A 14-year-old girl was referred urgently from her GDP regarding extensive decalcification of her permanent dentition (Figures 1 and 2). The patient had commenced orthodontic treatment 18 months earlier, but failed to attend following her first two orthodontic reviews. Medical history was non-contributory with no history of vomiting or gastric reflux. History did not elicit a dietary reason for the presentation. In this instance, the patient's parents had separated following commencement of her orthodontic treatment, resulting in confusion over which parent took responsibility for orthodontic follow-up appointments.
Figure 1. Demonstrating decalcification at initial presentation.Figure 2. Extensive decalcification of lower incisors.
The patient had initially noted that her teeth were becoming ‘brown’ and was concerned. However, she had continued to wear the appliance. This was instrumental in the development of widespread demineralization of her permanent dentition (Figure 3). Lack of dental or orthodontic review contributed to this rapid deterioration. The appearance of her permanent dentition was a cause of great distress, but the patient was reluctant to seek help, owing to anxiety regarding the severity of her condition. She finally confided in her mother when she became symptomatic with pain.
Figure 3. Decalcification of upper incisors and stomatitis.
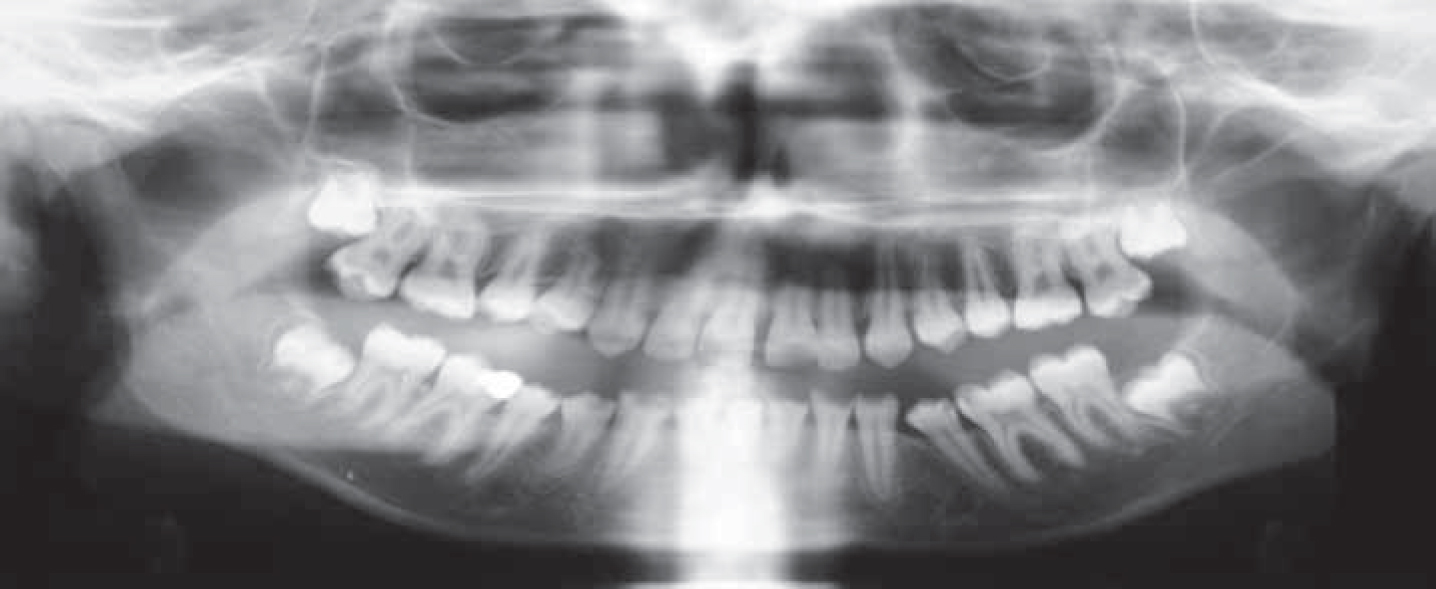
Examination revealed extensive demineralization of the permanent dentition, particularly in the lower arch. Oral hygiene was poor, with generalized plaque retention and gingival inflammation. A panoramic radiograph was taken which demonstrated no evidence of root resorption or apical pathology, as well as the presence of all permanent teeth, including third permanent molars (Figure 4).
Figure 4. OPT radiograph.
Initial treatment involved the immediate cessation of functional appliance therapy with intensive prevention. High fluoride toothpaste and a fluoride mouthwash were prescribed, with the regular application of fluoride varnish. Oral hygiene instruction and dietary advice were reinforced. The patient was reviewed three months later and all non-carious premolar and molar teeth were fissure sealed. Bitewing radiographs revealed multiple carious permanent premolar and molar teeth (Figure 5). These teeth were subsequently restored using composite resin, with concomitant preventive advice and the regular application of fluoride varnish.
Figure 5. Bitewing radiographs.
Long-term composite restorations and, where necessary, porcelain crowns will be considered for restorable anterior teeth. Endodontic therapy or extraction may be required for one or more of these teeth. If necessary, a removable partial denture or adhesive bridge will be considered.
Unfortunately in this case, the continued wear of a functional appliance combined with poor oral hygiene contributed to rampant demineralization of the permanent dentition. This was compounded by the patient's failure to attend for follow-up treatment, and her reluctance to seek help when she realized the extent of her dental problems.
Discussion
Our case demonstrates the importance of regular follow-up once orthodontic appliances have been fitted. Examining the reasons behind such a rapid deterioration in oral health can be challenging, particularly when oral hygiene was deemed adequate prior to the patient's orthodontic treatment. Adolescence is a time of rapid physical development. It is also a time of newly found independence and deep emotional changes. Eating patterns alter as appetites increase, and can result in snacking between meals, often with a high proportion of sugary foods and drinks.7
The psychological effects of divorce can exacerbate an adolescent's confusion at this already difficult time.8 From the point of view of teenagers, divorce is a stressful experience, with disruption of the home and routine of family life.
The advice given in the functional advice leaflet produced by the British Orthodontic Society9 includes advice regarding the avoidance of carbonated drinks and sweets, particularly toffees. It mentions the importance of good oral hygiene, as well as routine dental review. Whilst it does recommend regular orthodontic visits for brace adjustment, it does not have any advice regarding those patients who do not attend for follow-up appointments. It would be appropriate to include clear guidance in this leaflet regarding the importance of follow-up orthodontic care for those wearing orthodontic appliances, and the cessation of appliance wear for those who do not attend for orthodontic review.
Conclusion
Our report highlights the inherent risks of dental decalcification during orthodontic treatment and emphasizes the need for regular dental review to ensure there are no concerns developing. From the moment treatment has been agreed, the orthodontic team are in a strategic position to counsel teenagers, and it is incumbent upon them to act as patient advocate, whilst ensuring continuity of care for the patient.