Nunn JH, Carter NE, Gillgrass TJ, Hobson RS, Jepson NJ, Meechan JG, Nohl FS. The interdisciplinary management of hypodontia: background and role of paediatric dentistry. Br Dent J. 2003; 194:245-251
McNamara C, Foley T, McNamara CM. Multidisciplinary management of hypodontia in adolescents: case report. J Can Dent Assoc. 2006; 72:(8)740-746
Brook AH. Dental anomalies of number, form and size: their prevalence in British schoolchildren. J Int Assoc Dent Child. 1974; 5:37-53
Hobkirk JA, Brook AH. The management of patients with severe hypodontia. J Oral Rehabil. 1980; 7:289-298
Gungor AY, Turkkahraman H. Tooth sizes in nonsyndromic hypodontia patients. Angle Orthod. 2013; 83:(1)16-21
Parkin N, Elcock C, Smith RN, Griffin RC, Brook AH. The aetiology of hypodontia: the prevalence, severity and location of hypodontia within families. Arch Oral Biol. 2009; 54:S52-S56
Militi D, Militi A, Cutrupi MC, Portelli M, Rigoli L, Matarese G, Salpietro DC. Genetic basis of non syndromic hypodontia: a DNA investigation performed on three couples of monozygotic twins about PAX9 mutation. Eur J Paed Dent. 2011; 12:21-24
Moller P, Ruud AF, Kvien TK. Variable expression of familial hypodontia in monozygotic triplets. Eur J Oral Sci. 1981; 89:16-18
Hekmatfar S, Jafari K, Meshki R, Badakhsh S. Dental management of ectodermal dysplasia: two clinical case reports. J Dent Res Dent Clin Dent Prospects. 2012; 6:(3)108-112
Suri S, Tompson BD, Atenafu E. Prevalence and patterns of permanent tooth agenesis in Down syndrome and their association with craniofacial morphology. Angle Orthod. 2011; 81:(2)260-269
Cahuana A, Palma C, Gonzales W, Gean E. Oral manifestations in Ellis-van Creveld syndrome: report of five cases. Pediatr Dent. 2004; 26:(3)277-282
Tereza GP, Carrara CF, Costa B. Tooth abnormalities of number and position in the permanent dentition of patients with complete bilateral cleft lip and palate. Cleft Palate Craniofac J. 2010; 47:(3)247-252
Meaney S, Anweigi L, Ziada H The impact of hypodontia: a qualitative study on the experience of patients. Eur J Orthod. 2012; 34:(5)547-552
Gill DS, Jones S, Hobkirk J, Bassi S, Hemmings K, Goodman J. Counselling patients with hypodontia. Dent Update. 2008; 35:344-352
Pjetursson BE, Tan WC, Tan K, Brägger U, Zwahlen M, Lang NP. A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin Oral Implants Res. 2008; 19:(2)131-141
This article describes the multidisciplinary management of a 9-year-old boy who presented with severe hypodontia. Treatment included preventive dentistry and early treatment to address his concerns regarding the poor aesthetic appearance of his anterior teeth. This included composite resin restoration of his upper permanent central incisors and a pre-adjusted edgewise appliance to close the diastema. A unique restorative technique was used to retain the closed diastema and restore the spaces of the missing lateral incisors.
Clinical Relevance: To illustrate the importance of multidisciplinary dental care in the treatment of patients with severe hypodontia.
Article
Hypodontia is the term used to describe the developmental absence of one or more teeth, excluding the third permanent molars. Oligodontia describes the developmental absence of six or more permanent teeth (excluding third permanent molar teeth) and anodontia refers to the complete absence of teeth.1 The prevalence of hypodontia in the primary dentition ranges from 0.1% to 0.9% with no specific gender predilection.1,2 In the permanent dentition, the prevalence is reported to be from 3.5% to 6.5% with a female preponderance of 3:2.2,3 The most commonly affected tooth (excluding third permanent molars) is the mandibular second premolar tooth, followed by the maxillary permanent lateral tooth and the maxillary second premolar tooth.1 Oligodontia or severe hypodontia is much less common, with a reported prevalence of 0.19%, and may involve teeth that are rarely absent, such as permanent canine and molar teeth.4 Teeth that are present may be conical in shape, or taper towards the incisal edge. An association between hypodontia and microdontia has been established in the literature. Gungor and Turkkahraman examined dental casts of patients with hypodontia, and found that teeth were significantly smaller than controls. Primary teeth may be retained in excess of normal lifespan in the absence of permanent successors.5
The aetiology of hypodontia involves both genetic and environmental factors.6 Mutations in the Pax9 gene have been linked to the autosomal dominant form of hypodontia.7 A multifactorial aetiology, involving polygenic inheritance with environmental influence was suggested by Brook.3 Environmental influence is suggested by the variability of expression in monozygotic twins.8
Hypodontia may occur in isolation, or in association with syndromes such as ectodermal dysplasia, Down syndrome, Ellis van Crevald syndrome, as well as conditions such as cleft lip and palate.9,10,11,12
Hypodontia can lead to psychological problems as a result of poor aesthetics.13 This condition may also have educational implications, with time taken out of school to attend multiple dental appointments. Changes to commissioning arrangements may lead to variability in the dental treatment funded by different regions, possibly leading to an increased financial burden for these patients.14
It is crucial that child patients with hypodontia are managed by an interdisciplinary team, including both the orthodontist and paediatric dentist. Effective communication between all professionals involved is necessary to achieve a successful outcome.1
Case history
A 9-year-old boy was referred from a specialist orthodontist to a consultant led paediatric dental service, regarding severe hypodontia and microdontia. The patient was unhappy regarding the aesthetics of his anterior teeth, in particular his midline diastema. Family history was negative for hypodontia. Medical history was remarkable only for a history of keratosis pilaris.
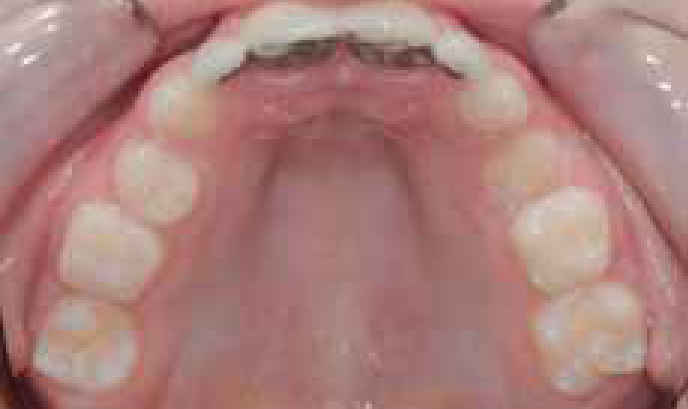
Extra-oral examination revealed erythematous, dry skin adjacent to the vermillion of the patient's upper and lower lips, consistent with a lip-sucking habit. The patient had blonde hair of normal thickness (Figure 1). Intra-orally, the patient presented with a late mixed dentition, with a high caries rate affecting the primary dentition. Disto-occlusal cavities were present in the upper right second primary molar tooth and the lower right first primary molar tooth. Oral hygiene was good. From an orthodontic point of view, a bilateral Class I molar relationship was noted, with a 7 mm median diastema. The upper left first primary molar was infraoccluded. The patient presented with severe hypodontia and multiple clinically absent permanent teeth. The upper permanent central incisor teeth showed microdontia and were abnormally tapered towards the incisal edges (Figures 2–4).
Figure 1. Extra-oral view of patient showing dry facial skin and blonde hair of normal thickness.Figure 2. Intra-oral view showing hypodontia and microdontia.Figure 3. Intra-oral view of upper arch showing hypodontia, microdontia and dental caries URE.Figure 4. Intra-oral view of the lower arch showing hypodontia, microdontia and dental caries LRD.
A panoramic radiograph was taken (Figure 5) which showed severe hypodontia and the following teeth were absent: UR8, 5, 4, 3, 2, UL2, 3, 4, 5, 8, LR8, 7, 5, 4, 3, 1, LL1, 2, 3, 5, 8.
The clinical presentation of severe hypodontia and the dermatological condition suggested a differential diagnosis of ectodermal dysplasia. The patient was referred to a consultant geneticist for assessment and results were equivocal. The geneticist felt that it could be argued that the patient presented with isolated hypodontia, and dry skin is common. On the other hand, she felt that he may have had a mild form of hydrotic ectodermal dysplasia. The geneticist could not make a definitive diagnosis of ectodermal dysplasia, as the patient did not have any hair or nail features of the condition.
Initial treatment involved intensive prevention, with oral hygiene instruction, dietary advice and the regular application of fluoride varnish. The first permanent molar teeth and the lower left first premolar tooth were fissure sealed. At this point, the patient was assessed on a joint orthodontic-paediatric dental clinic, and the following treatment plan was suggested to deal with the patient's concerns:
Upper permanent central incisor teeth to be restored with composite resin;
Orthodontic treatment with pre-adjusted edgewise appliances to close the diastema;
Close liaison between paediatric dentistry and orthodontics to provide restoration of the spaces of the missing lateral incisors and retention with a bonded retainer.
The upper permanent incisor teeth were restored using composite resin and a good aesthetic result was achieved (Figure 6). The median diastema was closed over a period of eight months using a sectional fixed appliance.
Figure 6. Upper permanent central incisors restored with composite resin.
The upper right second primary molar tooth was restored using composite resin, and the lower right first primary molar was extracted owing to its poor prognosis.
The upper left first primary molar tooth was monitored carefully with a plan to extract this tooth, should the infraocclusion progress. Otherwise, it was decided to leave it in situ, in order to preserve bone.
The options for restoration of the upper permanent lateral incisor spaces were discussed with the patient and his parents, including the fabrication of bilateral resin-bonded bridges, cantilevered from the permanent central incisors, or the provision of an upper removable partial denture. The patient was adamant that he did not wish to wear a denture. The disadvantages of providing resin-bonded bridges were explained, including the possibility of debonding and darkening of the central incisors. The patient and his parents opted to go ahead with resin-bonded bridges, and this raised the potential difficulty of placing a bonded orthodontic retainer palatal to the central incisor teeth.
A joint orthodontic-paediatric dental assessment was undertaken, with a laboratory technician in attendance. It was decided to fabricate the resin-bonded bridges with shortened wings, leaving space incisally for a bonded retainer. In the interim period, a bonded retainer was placed labial to the central incisor teeth.
Bilateral resin-bonded bridges were fabricated as planned, and cemented, with good aesthetic results (Figure 7). Following this, the bonded retainer was removed from the labial surfaces, and placed palatal to the central incisor teeth, in an incisal position to the resin-bonded bridge wings (Figures 8 and 9). The advantages of this treatment plan include the high success rate (87.7%) and low caries risk (1.5%) associated with resin-retained bridges.15 The incorporation of a separate retentive feature into the design ensures that failure of the resin-retained bridges will not compromise the orthodontic retention of the central incisors. The single cantilever design will not lead to plaque stagnation areas and subsequent caries should a single abutment fail.
Figure 7. Resin-bonded bridges have been placed, replacing UR2 and UL2, cantilevered from UR1 and UL1. Labial bonded retainer in situ.Figure 8. Bonded retainer placed in incisal position to the resin-bonded bridge wings.Figure 9. A bonded retainer has been placed palatal to the upper permanent central incisor teeth, in an incisal position to the wings of the resin-bonded bridges.
Conclusion
This case demonstrates the complexity of treatment planning for patients with severe hypodontia. Assessment by an interdisciplinary team was imperative to the successful outcome achieved. Close working between the orthodontic department, paediatric dental department and the dental laboratory allowed the provision of bilateral resin-bonded bridges, with the abutment teeth also utilized for bonded orthodontic retention.