Berger JL Self-ligation in the year 2000. J Clin Orthod. 2000; 34:(2)74-81
Damon DH The Damon low friction bracket: a biologically compatible straight-wire system. J Clin Orthod. 1998; 32:(11)670-680
Rinchuse DJ, Miles PG Self-ligating brackets: present and future. Am J Orthod Dentofacial Orthop. 2007; 132:(2)216-222
Nikolaos P, Argy P, Theodore E Self-ligating vs conventional brackets in the treatment of mandibular crowding: a prospective clinical trial of treatment duration and dental effects. Am J Orthod Dentofacial Orthop. 2007; 132:(2)208-215
Burrow SJ To extract or not to extract: a diagnostic decision, not a marketing decision. Am J Orthod Dentofacial Orthop. 2008; 133:341-342
Clinical efficacy of the damon (self-ligation) system in a borderline case Jigar R Doshi Kalyani Trivedi Tarulatha Shyagali Orthodontic Update 2025 8:1, 28-32.
For many years, orthodontists have ligated brackets with wire or elastomeric ties. Much of our treatment planning and mechanics have been dictated by a mechanical system incorporating significant amounts of friction. This article will present a nearly friction free system using high-tech brackets and wires, which is claimed to reduce the need for auxiliary expanders significantly.
Clinical Relevance: Self-ligation systems have the advantage of low friction mechanics; this may produce significant expansion in the premolar and molar regions. In addition, very low forces for orthodontic tooth movement are applied when compared to conventional brackets.
Article
Jigar R Doshi
The first self-ligating brackets were introduced by Dr Jacob Stolzenberg in the early 1930s in the form of the Russell attachment.1 The advantage of all self-ligating brackets involves the reduction in ligation time by non-usage of materials such as elastomeric modules or steel ligatures. This leads to reduced friction when using sliding mechanics and low magnitude forces, resulting in fewer side-effects.2,3 For example, the Damon SL bracket has a second generation self-ligating archwire cover which slides vertically in an occlusal direction in the upper arch and in a gingival direction in the lower arch. When the cover is closed the slot is converted into a rectangular edgewise slot through which the archwire passes. The Damon system uses light forces to transmit archwire energy to the bracket without modification or binding by ligatures; it treats a significant number of cases by non-extraction when biologically possible and is compatible with dental and facial treatment goals.2
The Damon archform does not distinguish between upper and lower archforms. This archform provides expansion in the premolar and molar regions but not in the intercanine region. Customization of the archform cannot obviously take place until the working archwires stage.3 This article presents a clinical case report in which self-ligating brackets are used to correct crowding in both upper and lower arches without resorting to extractions.
Case report
The patient presented as a girl of 15 years of age with a severely crowded malocclusion of dento-alveolar origin. She was 5'3” tall and weighed 45 kg. The patient had experienced recent rapid growth and was believed to be in the declining phase of the pubertal growth spurt. The patient was in good general health and had no significant past medical history. There was a genetic component to her malocclusion.
Diagnosis
On clinical examination and cephalometric evaluation, she was diagnosed as a skeletal Class I growth pattern with an Angle's Class I dento-alveolar malocclusion with severe crowding in both arches in the anterior region. The profile was convex with acceptable vertical proportions. The overbite was increased to 3 mm. Maxillary midline was shifted 1 mm to the left of the facial midline (Figure 1). The panoramic radiograph showed that the maxillary right canine was impacted just below the cemento-enamel junction (CEJ) of the lateral incisor crown. Intra-oral examination suggested that the impacted canine was positioned buccally. Cephalometric analysis is represented in Table 1.
Figure 1. Pre-treatment photographs.
Variable
Pre-Treatment
Post-Treatment
SNA
77°
77°
SNB
76°
76°
ANB
1°
1°
Wits Appraisal
1 mm
2 mm
Dental Base Relationship:
Upper Incisor to NA (mm/deg)
36°/11 mm
32°/11 mm
Lower Incisor to NB (mm/deg)
26°/8 mm
32°/8 mm
Upper Incisor to SN Plane
113°
109°
Lower Incisor to Mandibular Plane Angle (IMPA)
97°
100°
Inter-Incisal Angle
145°
132°
Lower Incisor to APo Line
28°/5 mm
32°/8 mm
Overbite
4 mm
2 mm
Overjet
5 mm
2 mm
Vertical Skeletal Relationships:
Maxillary - Mandibular Planes Angle
32°
30°
SN Plane - Mandibular Plane
32°
32°
Jarabak Ratio
63.04%
66.66%
Maxillary Length
98 mm
98 mm
Mandibular Length - Effective (McNamara)
128 mm
129 mm
Soft Tissues:
Nasolabial Angle
100°
102°
Specific objective of treatment
After analysis, the treatment objectives for this patient were to achieve optimal axial inclination of maxillary and mandibular teeth with corrected overbite and overjet, together with maximum functional intercuspation by correction of the severe crowding in upper and lower arches and to obtain a well-balanced facial profile.
Treatment plan
The treatment plan was a non-extraction approach using the 0.022” Damon self-ligation appliance. Since the impacted canine was positioned at a level just below the crown of the lateral incisors, the treatment plan included surgical exposure and guided eruption of this tooth.
Conventional treatment planning would suggest that four first premolars be extracted, but treatment was begun with a non-extraction protocol using the 0.022” Damon self-ligation appliance from first molar to first molar in the upper arch, second molar to second molar in the lower arch.
Treatment progress
At the start of the treatment, the upper arch was bonded with banding in both upper first molars. The impacted left canine was surgically exposed with the help of electro-cautery; just after exposure a canine bracket was bonded to the tooth. Levelling was undertaken using 0.014” Damon copper Ni-Ti wire in the upper arch (Figure 2).
Figure 2. Intra-oral photographs with initiation of orthodontic treatment by using 0.014” Damon copper Ni-Ti wire in the upper arch.
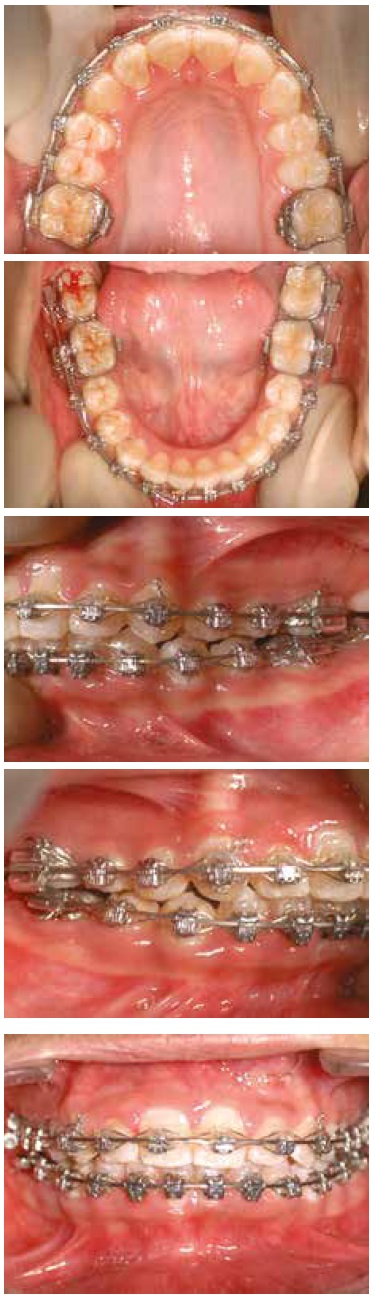
Two months later, the lower arch was bonded from 2nd molar to 2nd molar and a 0.014” Damon copper Ni-Ti wire was placed, while a 0.016” Damon copper Ni-Ti was placed in the upper arch. The action of the small round archwire in the large lumen of the Damon system tube appliance produces an arch-widening effect posteriorly with usually minimal change in lower incisor position. Orbicularis oris and mentalis muscles may also create a lip bumper effect, which minimizes anterior movement of the incisors (Figure 3).
Figure 3. Intra-oral photographs with upper 0.016” Damon copper Ni-Ti and lower 0.014” copper Ni-Ti wires.
After a further month, the lower left canine bracket was rebonded in the lower arch and 0.014” x 0.025” copper Ni-Ti was placed in the upper arch. Another month later, a 0.014” x 0.025” copper Ni-Ti was placed in the lower arch. With progression from round to rectangular copper Ni-Ti wires, rotations, which are present in the upper premolar and molar region, are efficiently corrected.
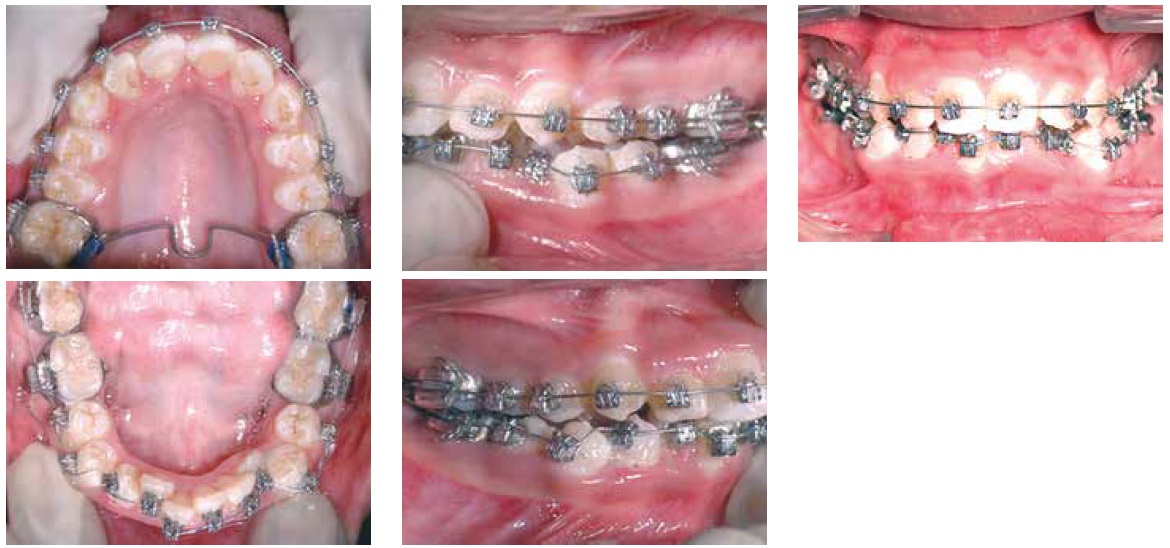
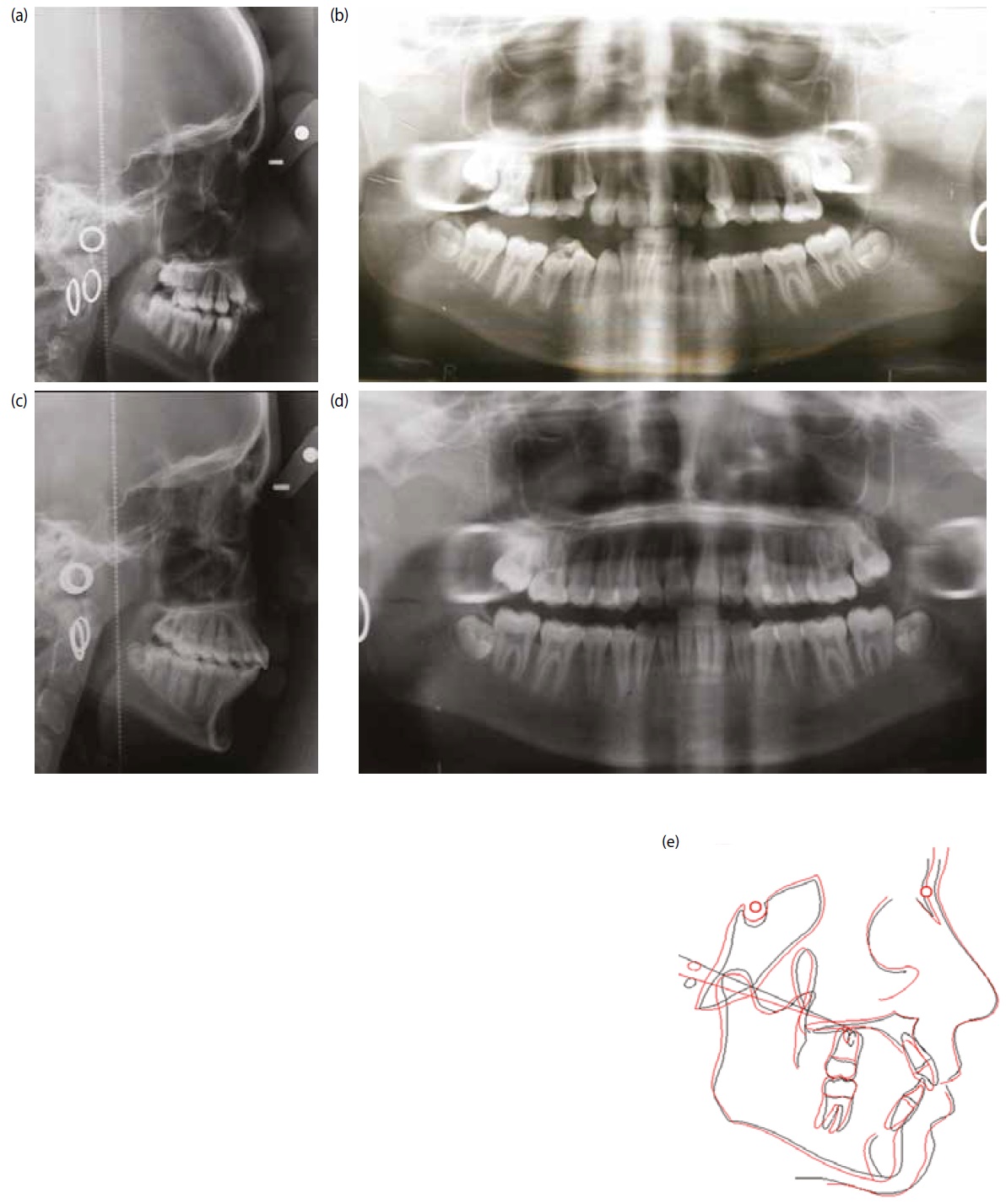
Two months later, axillary and mandibular 0.017” x 0.025” stainless steel archwires were placed and yellow (2.5 oz) Class II elastics placed to maintain the Class I canine and molar relation and, after a further two months, maxillary and mandibular 0.019” x 0.025” stainless steel archwires were placed and yellow Class II elastics were continued. Two months later, maxillary and mandibular 0.021” x 0.025” wires were placed for 2 months to allow torque expression (Figure 4). After another two months, 0.018” stainless steel wire was placed in upper and lower arches and red elastics (3/16” 3.5 oz) were placed in triangular and Class II mode for settling of buccal segments. Finally, a month later, debonding was done and a fixed orthodontic lingual retainer was bonded in upper and lower arches, along with upper and lower Hawley retainers (Figure 5). The pre-treatment and post-treatment lateral cephalogram and orthopantomograph (OPG) x-rays and superimposition are shown in Figure 6.
Figure 4. Intra-oral photographs with 0.021” x 0.025” upper and lower stainless steel wire.Figure 5. Post-treatment photographs after debonding the appliance.Figure 6.
(a, b) Pre-treatment x-rays. (c, d) Post-treatment x-rays. (e) Superimposition of pre-treatment and post-treatment x-ray tracings (superimposition on SN Plane and N Point).
Conclusion
With self-ligation, the combination of minimal friction, low forces and extended time between adjustment visits allow tooth movements to occur which, it can be argued, are technically not possible with conventional bracket systems. The orthodontist is thus able to treat many borderline cases more easily without resorting to the extractions that would have been required previously.