Ahmad S, Bister D, Cobourne MT The clinical features and aetiological basis of primary eruption failure. Eur J Orthod. 2006; 28:535-540
Decker E, Stellzig-Eisenhauer A, Fiebeg B PTHR1 loss of function mutations in familial nonsyndromic primary failure of tooth eruption. Am J Human Genet. 2008; 83:781-786
Proffit WR, Vig KWL Primary failure of eruption: a possible cause of posterior open-bite. Am J Orthod. 1981; 80:(2)173-190
Dibiase AT, Leggat TG Primary failure of eruption in the permanent dentition of siblings. Int J Paed Dent. 2000; 10:153-157
Raghoebar GM, Boerimg G, Vissink A, Stegenga B Eruption disturbances of permanent molars: a review. J Oral Pathol Med. 1991; 20:159-166
Fujiyama K, Yamashiro T, Fukunaga T, Balam T, Zheng L, Takano-Yamamoto T Denervation resulting in dento alveolar ankylosis associated with decreased malassez epithelium. J Dental Res. 2004; 83
Nielsen SH, Becktor KB, Kjaer I Primary retention of first permanent mandibular molars in 29 subjects. Eur J Orthod. 2006; 28:529-534
This case series highlights four clinical cases which presented at a dental hospital with atypical features of primary eruption failure. These patients demonstrate the heterogeneous nature of cases that can present with features of primary eruption failure. These cases are presented with a view to introducing a new classification system as an alternative to the encompassing term ‘primary failure of eruption’.
Clinical Relevance: The aetiology of primary eruption failure is poorly understood and can present the clinician with a diagnostic challenge, being based mainly on a diagnosis of exclusion. This case series presents four cases of primary eruption failure that do not conform to the classical clinical description. A new classification system is proposed that groups cases with common clinical features and may aid diagnosis and management.
Article
Tooth eruption is defined as a process whereby the forming tooth migrates from its intra-osseous location in the jaw to its functional position within the oral cavity.1 A tooth may have undergone successful growth and calcification, however, if it fails to erupt it is functionless. There are many theories of eruption as tooth eruption is a complex process which relies on poorly understood timed interactions between cells of the dental follicle and the surrounding alveolus.2 The different theories of tooth eruption include:1
Growth of the root;
Growth of dentine and pulpal constriction;
Growth of periodontal tissues;
Pressure from muscular action on the alveolar process;
Resorption of alveolar bone;
Pressure from cellular proliferation;
Pressure from vascular bed in pulp and periapical tissues.
Although many theories of eruption exist, there is little evidence to support these theories and the eruption process is still an intriguing process which requires further research.
Disturbances in tooth eruption have a multifactorial aetiology, including failure as a result of a mechanical obstruction, syndromes, pathology or disruption of the eruptive mechanism. There are a number of syndromes that demonstrate eruption failure as part of their clinical presentation. There is therefore a clear, known genetic origin to eruption failure related to a small number of syndromes including:
Research is ongoing to identify the gene responsible for non-syndromic eruption failure and there is a suggestion from recent work that parathyroid hormone receptor 1 (PTHR1) gene mutations may be responsible for non-syndromic eruption failure.4
Primary failure of eruption is a poorly understood condition which is defined as the eruption failure of non-ankylosed teeth due to an abnormality in the eruption mechanism of the tooth where there is no obvious impediment to eruption or systemic cause.5,6 Local factors which can impede a tooth's eruption include:
Supernumerary teeth;
Dilacerated roots following trauma;
Crowding;
Early loss of deciduous teeth;
Muscle attachments;
Thick fibrous gingivae and necking of the alveolar bone.
Primary failure of eruption can present with the following features, making the diagnosis difficult:3,5
Posterior teeth are more commonly affected than anterior teeth;
Primary and secondary dentition can be affected;
Involvement may be unilateral or bilateral;
Teeth distal to the first affected tooth are almost always affected;
Application of orthodontic forces induces ankylosis;
Teeth may erupt initially before ceasing to erupt further;
Occurs in isolation, other family members not usually affected.
This clinical condition can have two separate clinical presentations. Where there is a complete failure of tooth eruption, this is known as ‘primary retention’ and the second clinical presentation presents with the tooth penetrating the oral mucosa before undergoing an unexplained cessation of further tooth eruption, known as ‘secondary retention’.7 As mentioned previously, the diagnosis of this condition presents the clinician with a challenge and a diagnosis may be made retrospectively only after the application of orthodontic appliances have failed to extrude the teeth in question.
A recent review of the literature showed that the most common teeth affected were first and second molars, although incisors, canines and premolars were also affected but with a reduced occurrence. It was also highlighted that, in 50% of the cases, there was a family history of eruption failure and there was also a higher level of hypodontia compared to the population norm in the study, therefore suggesting that there is a genetic component to the aetiology of primary failure of eruption.3 This most recent review of the literature highlights the strong tendency towards a positive family history, which differs from the original work by Proffit and Vig.5 It has also been suggested that there is a link between innervation and eruption of teeth and an in vitro study has shown that disturbances to the inferior alveolar nerve can cause disturbances in tooth eruption thought to be due to the denervation.8,9
This paper presents interesting clinical cases which show atypical primary failure of eruption and do not conform to the above encompassing umbrella term of ‘primary failure of eruption’. In light of these observations, a new classification of eruption failure is proposed in this paper.
Case 1
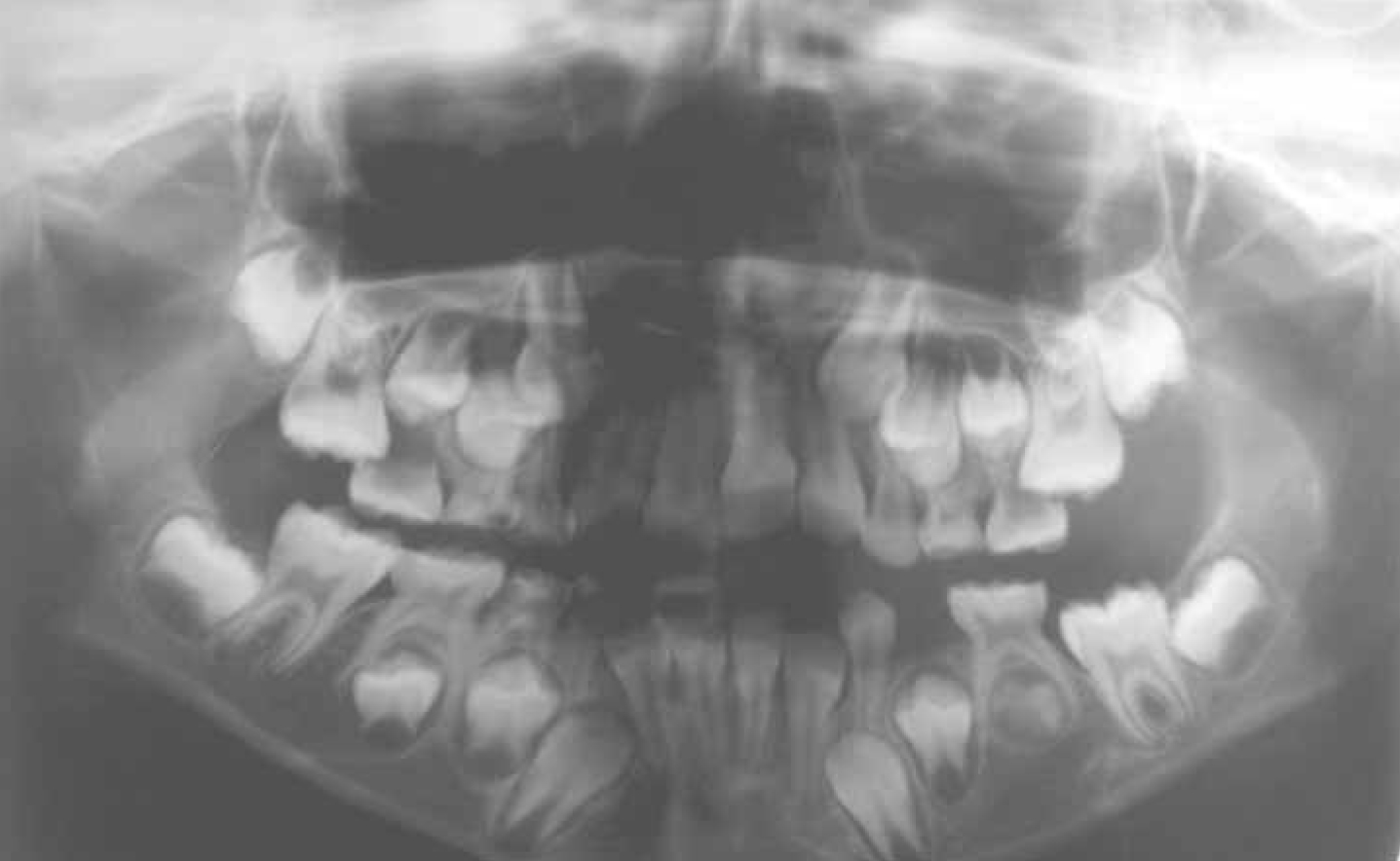
This case is of a 17-year-old female patient. RM has well-controlled asthma and is otherwise fit and well with no family history of primary failure of eruption. RM was initially referred to Glasgow Dental Hospital Orthodontic Department in 2002 by her GDP who was concerned that her upper left central incisor (UL1) was delayed in its eruption compared to the contralateral upper right central incisor (UR1). RM was first seen for an assessment at 9 years of age in the mixed dentition. RM has Class I incisors on a Class I skeletal base with average facial proportions. After a full history, examination and radiographic assessment, it was concluded that there was no supernumerary tooth present in the region of UL1, or any other local factor impeding the eruption of UL1, and all other permanent teeth were erupting/developing normally at this time. The treatment plan at this stage was to review the patient again in 6 months' time and reassess the eruption of UL1, as it was visible through the mucosa and there was adequate space for the central incisor to erupt (Figure 1).
Figure 1. Case 1 (RM): OPT taken in 2002 showing the unerupted UL1 and all other teeth are erupting/developing normally at this stage.
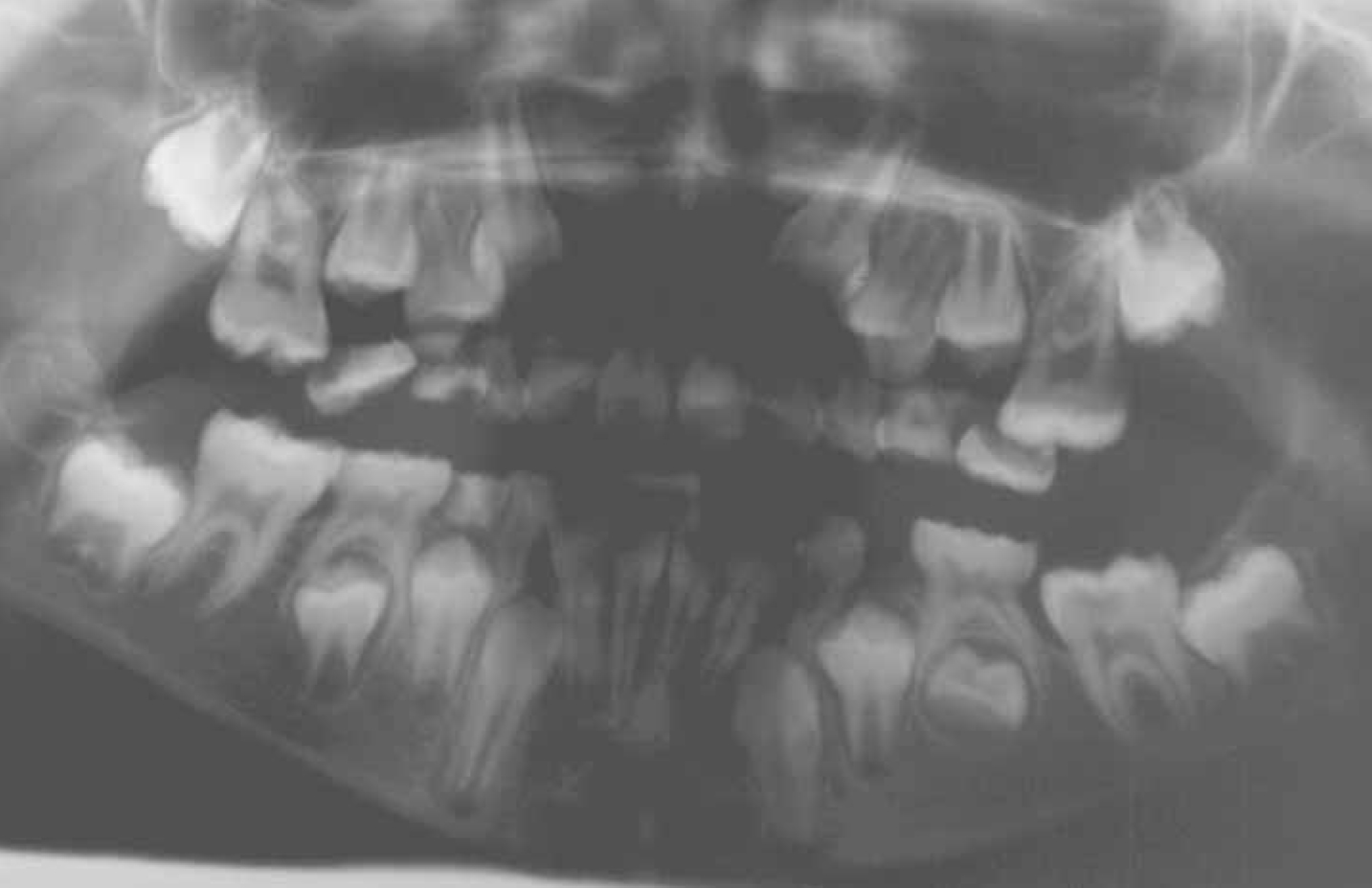
RM was reviewed 6 months later in the Orthodontic Department and UL1 was erupting well. It was noted at this visit that the patient had potential crowding in both arches and RM was therefore placed on an annual recall to await eruption of premolar units before further assessment. At a review in 2004, it was noted at this visit that the lower left first permanent molar (LL6) was carious and infra-occluded and it was decided that the prognosis was poor for this tooth. RM gave consent for surgical removal of LL6. It was also brought to the attention of the patient at this time the doubtful prognosis of further eruption of units distal to the LL6 (Figure 2).
Figure 2. Case 1 (RM): OPT taken in 2004 showing infra-occluded carious LL6.
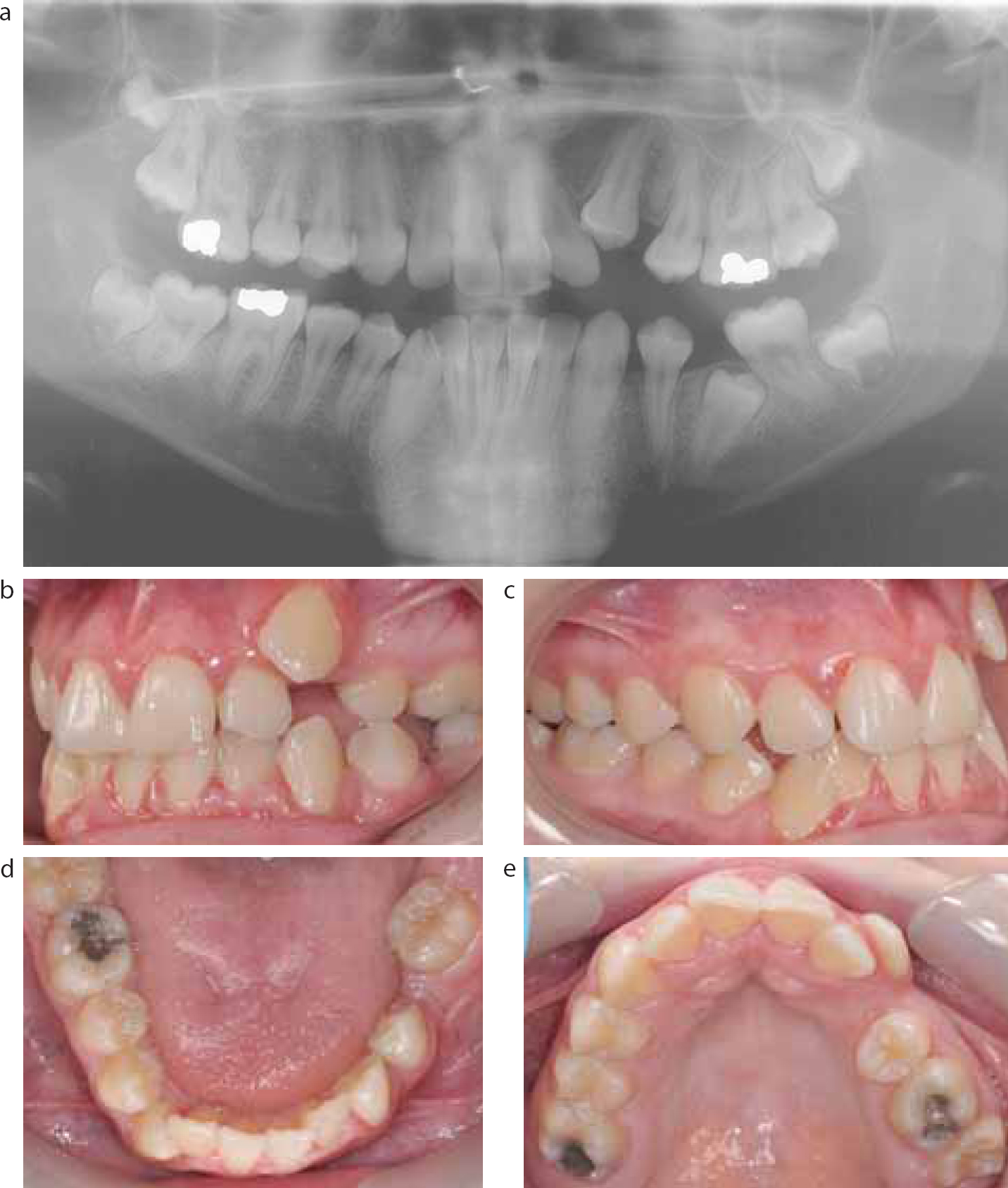
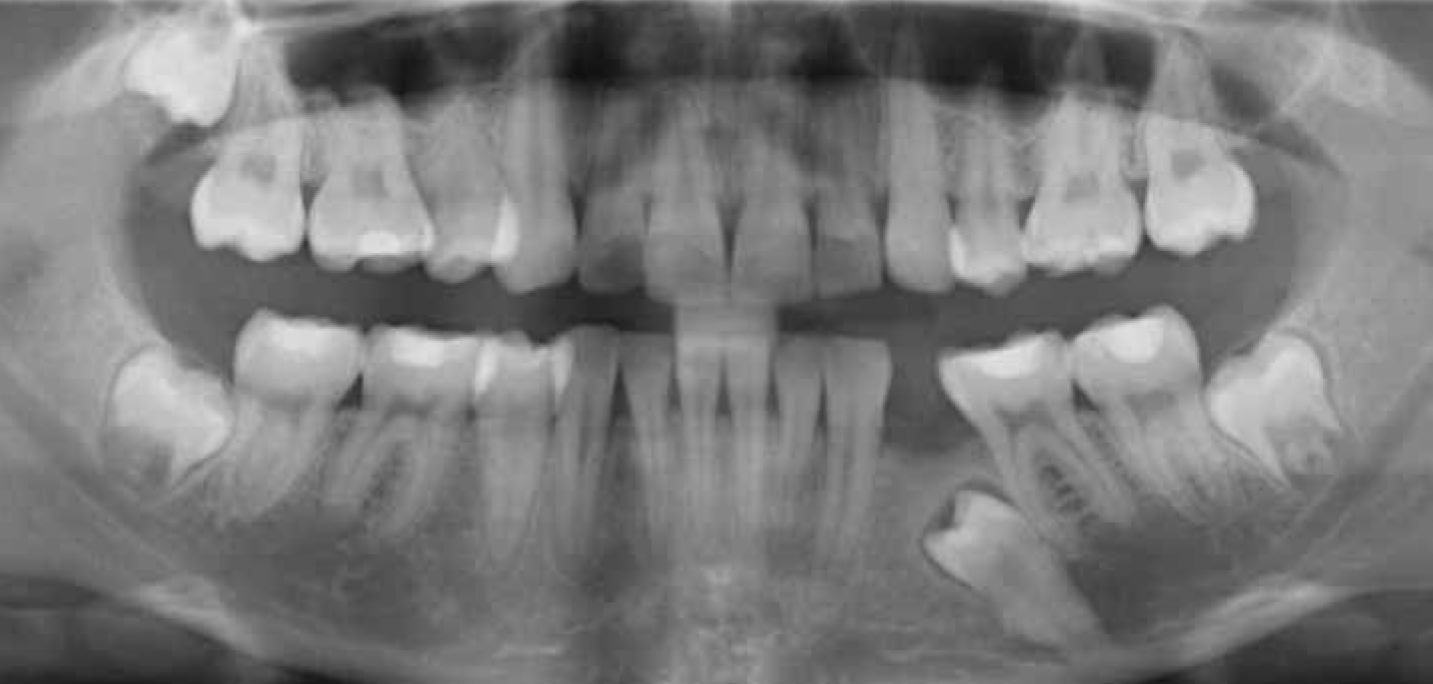
The patient was kept under close review awaiting eruption of all permanent teeth. RM started URA treatment in February 2009, along with extraction of the upper left first premolar (UL4) and the lower left second deciduous molar (LLE) (Figure 3). The patient lost contact with the department for 11 months and when she finally presented back in the department she had not been wearing her URA for the previous 5 months. At her most recent presentation, RM was expressing concerns regarding the aesthetics of her front teeth and expressed an interest in continuing with orthodontic treatment. It was noted at this visit that the lower left second premolar (LL5) was still unerupted, however, the lower left second permanent molar was erupted (LL7), which was surprising as LL6 had exhibited features of secondary retention. It had been explained to the patient that there was little chance of teeth distal to LL6 erupting. An OPT radiograph was taken at this visit which confirmed that LL5 was impacted and had full root formation. Other features of note on this OPT radiograph were a retained fragment of UL4 root and impacted upper left and right second molars (UL7, UR7) (Figure 4).
Figure 3. Case 1 (RM): (a–c) Patient ready to commence URA treatment 2009.Figure 4. Case 1 (RM): (a) OPT showing unerupted LL5 and retained root fragment UL4 and (b–e) clinical photographs showing presentation of malocclusion following failed URA treatment 2010.
It was decided to manage RM by providing her with upper and lower fixed appliances with extraction of the lower right first permanent molar (LR6) and the upper right first permanent molar (UR6), along with surgical exposure of LL5 and surgical removal of the retained UL4 root fragment. Initially space would be created for the impacted LL5 before applying any orthodontic forces. The patient was made aware that this tooth may not be able to be aligned. Treatment is still ongoing.
Case 2
This case is a 19-year-old fit and healthy female (CA) who presents with Class II division 2 incisors on a Class II skeletal base with severe upper and lower arch crowding. An OPT radiograph taken prior to commencing orthodontic treatment showed the presence of all permanent teeth. However, the lower left second premolar (LL5) was impacted and the treatment plan was confirmed as extraction of all first premolars (UL4, UR4, LL4 and LR4), upper and lower fixed appliances, and long term retention with Essix type retainers (Figure 5).
Figure 5. Case 2 (CA): OPT at initial presentation prior to removal of four first premolar units.
The patient commenced treatment, however, LL5 failed to erupt as expected into the space created from the extraction of LL4. The patient was therefore referred to Glasgow Dental Hospital for a consultation with regard to surgical exposure and alignment of LL5. After an oral surgery consultation, she decided that she no longer wanted to proceed with the surgery to expose and align LL5. Follow-up radiographs of LL5 show that it was submerging from its original position, however, there was no pathology associated with this tooth or damage to any adjacent structures (Figure 6). The patient continued with her orthodontic treatment and accepted the space in the lower left premolar region. CA has now finished active treatment and is currently in retention with upper and lower Essix type retainers. The unerupted LL5 is being kept under observation and further radiographs will be taken if it becomes symptomatic.
Figure 6. Case 2 (CA): OPT showing failed eruption of LL5 and progression of submergence.
Case 3
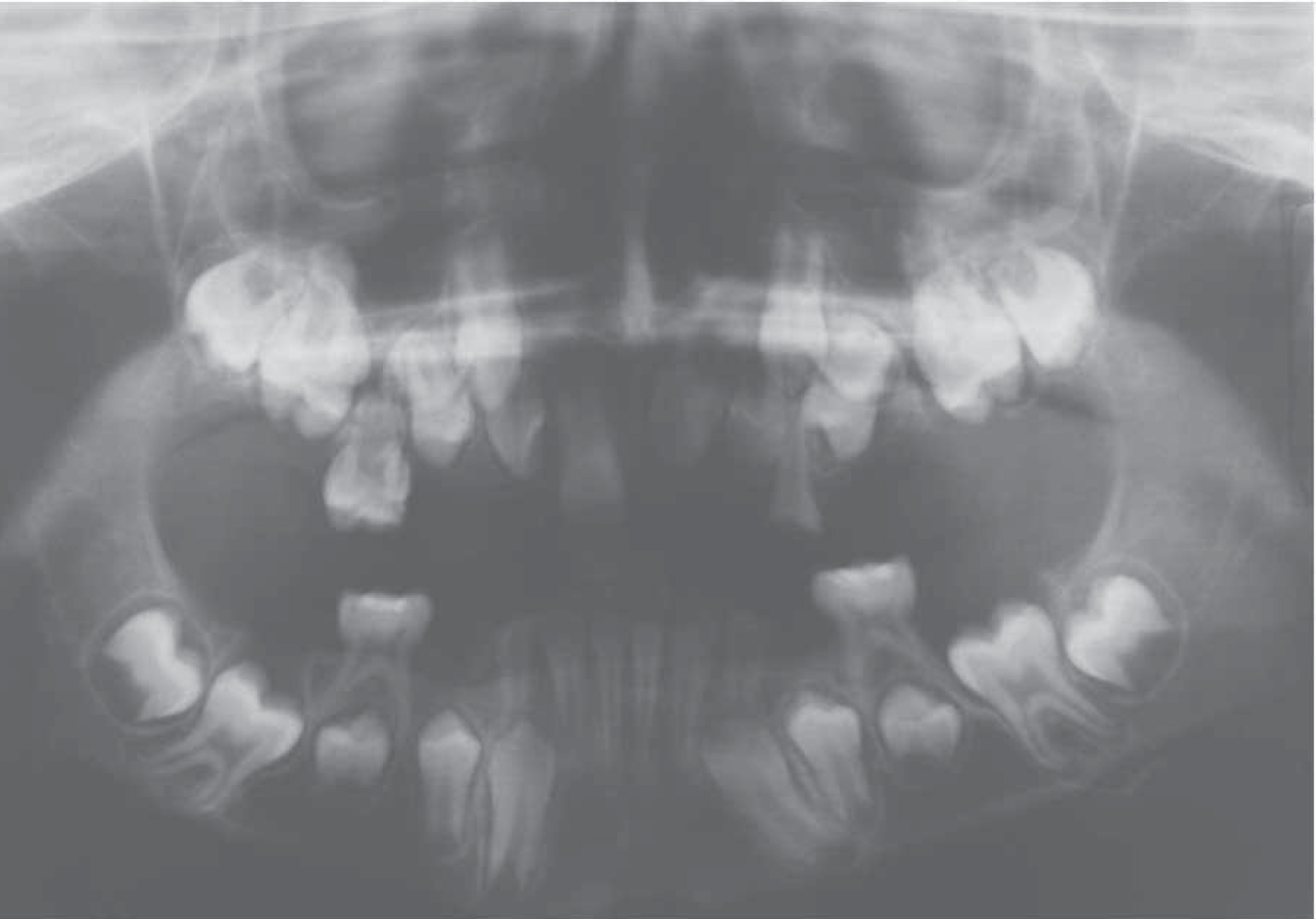
This clinical case is of a male patient (NM) who first presented at Glasgow Dental Hospital Orthodontic Department at the age of 12 years. NM presented with a Class II division 1 incisor relationship on a Class II skeletal base. At his initial presentation, at age 12, the only permanent teeth erupted were the upper right central incisor, lower right central incisor, lower right lateral incisor, lower left central incisor and lower left lateral incisor (UR1, LR1, LR2, LL1 and LL2) (Figure 7). This OPT radiograph was taken in 2002 at the patient's initial presentation and shows delayed eruption of the permanent dentition. There was a positive family history of eruption failure affecting the patient's father and the father's sister.
Figure 7. Case 3: NM aged 12 years at initial presentation showing delayed eruption of the permanent dentition 2002.
The proposed treatment plan for NM after consulting with our paediatric colleagues was to plan for a surgical exposure and placement of a gold chain to the upper left central incisor (UL1). However, at the patient's next review appointment in 2003, now aged 13 years of age, the UL1 had started to erupt and it was therefore decided to delay any surgical intervention and review the patient again in 6 months' time (Figure 8).
Figure 8. Case 3: NM showing spontaneous improvement in UL1.
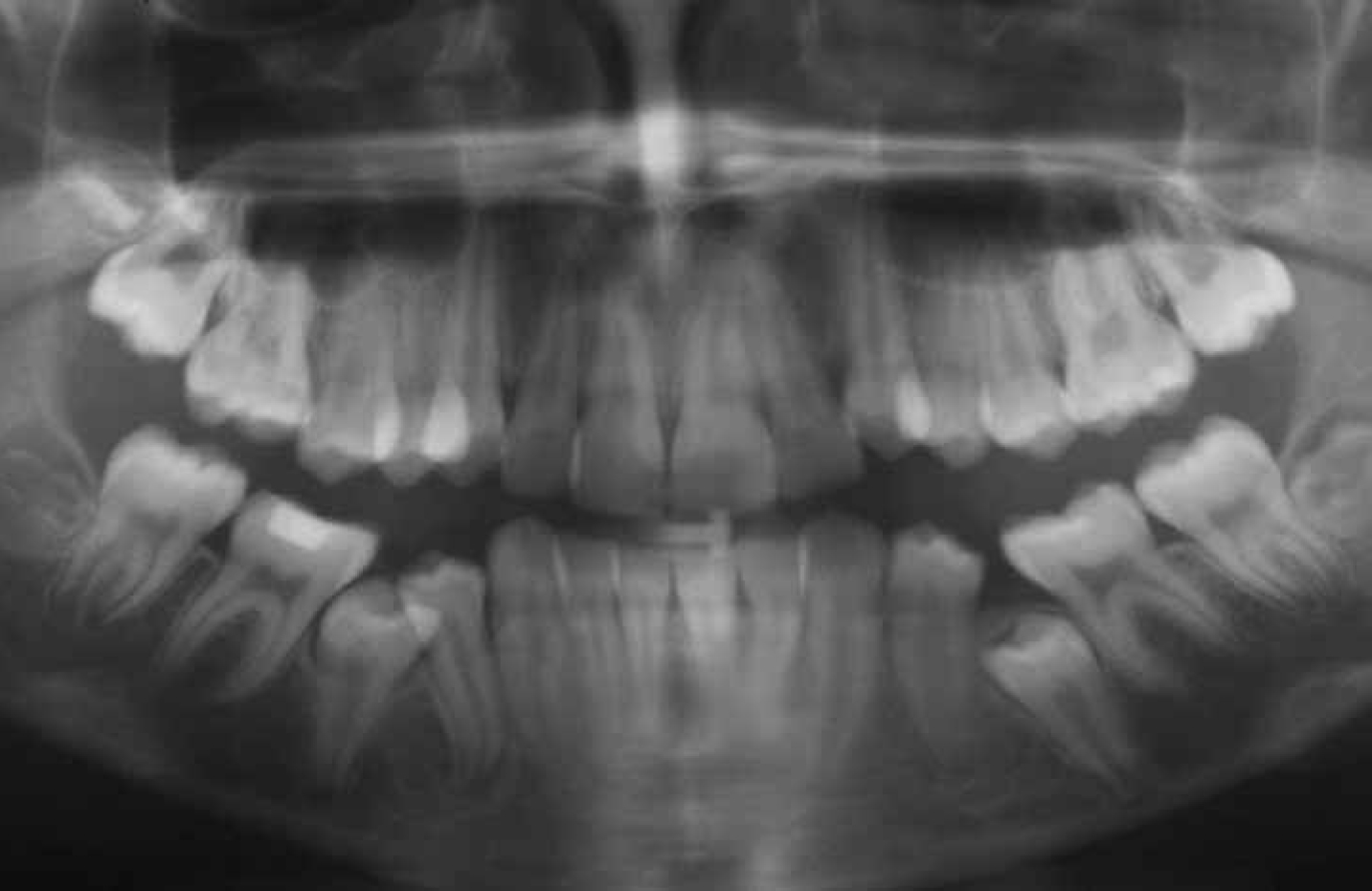
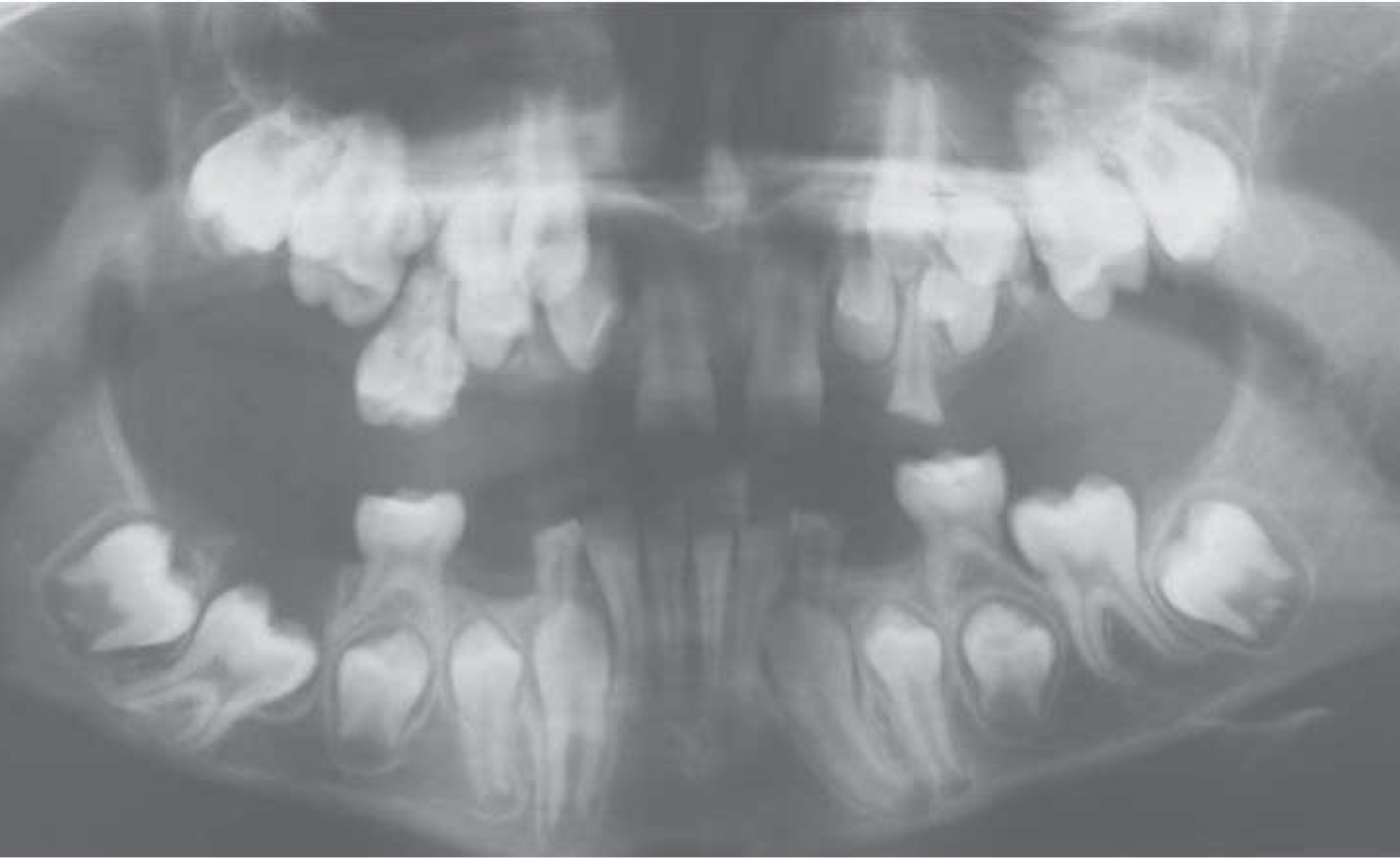
An OPT was taken in 2004 with NM now 14-years-old (Figure 9). This radiograph shows that there has been an improvement in the position of LL6 compared to the previous OPT taken 2 years earlier. By this stage, both of the upper central incisors had erupted and the patient had a midline diastema present. It was decided to close this orthodontically and retain with an upper bonded retainer on UL1, UR1. There was further discussion with our paediatric colleagues and it was planned to arrange surgical repositioning of the upper lateral incisors. However, during orthodontic closure of the midline diastema, the upper left lateral incisor, lower left first permanent molar and the lower right canine (UL2, LL6, LR3) all began to erupt. By the age of 15, NM had the following permanent teeth erupted: UR6, UR2, UR1, UL1, UL2, UL6, LL6, LL3, LL2, LL1, LR1, LR2, LR3 (Figure 10).
Figure 9. Case 3 (NM): OPT showing vertical development and root development of LL6 2004.Figure 10. Case 3: (a–d) NM aged 15 years after orthodontic alignment of UL1, UR1. Bonded retainer in situ.
At NM's most recent review, now aged 20 years, he presented complaining of being unhappy with the appearance of his teeth. On examination, he had the following teeth erupted: UR6, UR4, UR3, UR2, UR1, UL1, UL2, UL3, UL4, UL6, UL7, LL1, LL2, LL3, LL4, LL6, LR1, LR2, LR3, LR4, LR6. This case is interesting as it shows an atypical presentation of tooth eruption, approximately 8 years delayed compared to eruption norms. We would like to introduce the term ‘significant delayed eruption’ (SDE) as a diagnosis. NM has significantly delayed eruption of his permanent dentition and, at the age of 20 years, he still has unerupted premolar units with UR4 partially erupted. An OPT radiograph taken at the last review appointment shows the following features of note (Figure 11):
Dilacerated root LR4;
Ectopic and impacted UR5, UL5;
Unerupted LL5, LR5;
Unerupted LL7, LR7;
Atypical root form of UR6, UL6.
Figure 11. Case 3: NM aged 20 years. (a) OPT 2011 showing ectopic premolar units, impacted second premolars. (b–f) Clinical views showing current malocclusion.
NM malocclusion is complex and will involve multidisciplinary care with our oral surgery colleagues with regard to the impacted UR5, UL5 and, prior to any further active treatment, we plan to arrange a CBCT to check the position of UR5, UL5 prior to removal and to check for any root resorption of UL6, UR6. NM is keen to pursue active treatment and we hope we can provide treatment for NM to improve the appearance of his teeth.
Case 4
This is a clinical case of a female patient aged 13 years. MK is fit and well and there is no family history of eruption failure. MK presents with a history of a submerging upper right first permanent molar (UR6); the submergence was progressive and UR6 was removed under general anaesthetic. It was noted in the theatre notes that there was occlusal caries affecting the UR6. This case presents with sporadic localized 2° retention of UR6. The OPTs show progression of the submergence of UR6 (Figure 12).
Figure 12. Case 4: MK at initial presentation. (a) OPT dated 2009 and (b) OPT dated 2011 showing all permanent teeth developing. Failure of eruption of UR6 with progressive infraocclusion of UR6 prior to removal.
Discussion
Eruption failure is defined as ‘the non eruption or non emergence of a tooth or teeth, which are not ankylosed, in the absence of any other pathological cause’.3,5,6
This case series presents four individual cases with atypical features of eruption failure. Case 1 is atypical from the classical classification of eruption failure as the LL6, which was affected by an eruptive failure, was removed and, atypically, the patient had normal eruption of the lower left second molar (LL7). This differs from the classical features as described by Proffit and Vig.5 Case 2 is also atypical in the presentation of the eruption failure as this case also presents with units distal from the tooth affected erupting. Case 3 is an extremely interesting case, which doesn't conform to the classical eruption failure features, as all teeth have been affected with a significant delay in their eruption and gradually, over time, the teeth have begun to erupt. Another interesting feature of this case is that there is a strong positive family history of eruption failure affecting the patient's father and his sister. Case 4 at present may be the more typical of the cases as it has classically had a permanent molar affected which, from the literature, appears to be the most commonly affected tooth,3,5 however, this patient is still under close observation as we cannot d predict the outcome for the second permanent molar at present.
In light of these cases, we propose a new classification system based on suspected aetiology and the clinical features of eruption failure (Table 1). First, the diagnosis of eruption failure should be made by taking a careful history and by clinical and radiographic observation over at least 12–24 months. This enables alternative diagnoses to become apparent and allows close observation of root development and slow eruptive movements over time. The classification system is based on aetiology before describing the clinical presentation. The aetiology can be either familial, or sporadic. If there is a familial history of eruption defects, this would suggest a strong genetic aetiology, however, if there is no positive familial link, then the eruption failure is classified as sporadic. The clinician then categorizes the clinical presentation of eruption failure into localized or generalized, depending on the number of teeth affected. Localized eruption failure is classified as one non-erupting tooth per quadrant, generalized eruption failure as more than one non-erupting tooth per quadrant. Similar to the IOTN score for hypodontia, this classification separates the milder cases, that may not require complex treatment, from the more difficult cases, which will require multidisciplinary management.
Aetiology
No. of Teeth Affected
Features of Retention
Familial
Sporadic
Up to one tooth missing per quadrant
>1 tooth per quadrant
1°
2°
SDE
The clinical presentation can then be divided into the presenting features of eruption failure described earlier as primary retention or secondary retention. In addition to the subdivisions of primary and secondary retention, we would like to introduce the term ‘significant delayed eruption’ (SDE) as an additional sub-classification. SDE has been demonstrated in Case 3, where the patient has a positive familial history of eruption failure. The patient was first seen in the orthodontic department when he was aged 11 years old and only had five permanent teeth erupted. The patient's teeth have gradually erupted over the years with no surgical intervention and now, aged 20 years, he has 20 permanent teeth erupted. This patient would be diagnosed with SDE of the permanent dentition as a subgroup of eruption failure.
We can apply the above classification system to the rest of the cases presented in this paper (Table 2). This new classification system provides the clinician with more information with regard to the individual cases than the original term of ‘primary failure of eruption’, which gives no indication if there is a familial link or the number of teeth that are affected.
Case No.
Aetiology
No. of Teeth Affected
Features of Retention
Overall Classification
Tx Provided
1RM
Sporadic
Localized
2°
SL2° Retention
XLA 36, align 35
2CA
Sporadic
Localized
1°
SL1° Retention
Observe 35
3NM
Familial
Generalized
1°
SDE
Ortho Tx, observe
4MK
Sporadic
Localized
1°
SL1° Retention
XGA 16
The management of patients with eruption failure depends on the diagnosis reached. All patients with suspected eruption failure require a thorough history, examination, radiographs and photographs as baseline records. If there is not an obvious local factor causing the eruption failure, then we suggest that the patient should be observed and a further radiograph of the same view should be repeated in 12 months' time.
If, on the follow-up radiograph, there is a suggestion of vertical eruption and root development has continued, the patient should continue to be monitored clinically and radiographically as he/she may have significant delayed eruption of the dentition.
If on the follow-up radiograph there is no improvement in the vertical development of the tooth, then eruption failure is likely and the classification system should be applied to provide the clinician with a detailed description of the eruption failure.
If the eruption failure is localized, management options available include observing and leaving the tooth/teeth in situ, removal of the tooth/teeth followed by prosthetic replacement or orthodontic space closure or, alternatively, a localized surgical reposition via a localized osteotomy.3 If the eruption failure is generalized, a multidisciplinary clinical approach will be required with orthodontic, paediatric and restorative colleagues best able to manage the more extensive cases. However, this will vary on a case by case basis.
Conclusion
Eruption failure of teeth would benefit from further research and investigation. The system proposed in this paper provides the clinician with greater diagnostic information related to the specific eruption failure presentation for each patient. In addition, we feel it would be advantageous to collect data nationally regarding eruption failure of teeth, allowing us to study and further understand this relatively common problem. Further research into this anomaly would allow for better management and care of patients.