Abdelkarim A, Jerrold L. Risk management strategies in orthodontics. Part 2: Administrative considerations. Am J Orthod Dentofacial Orthop. 2015; 148:511-514
Benson PE, Shah AA, Millett DT, Dyer F, Parkin N, Vine RS. Fluorides, orthodontics and demineralisation: a systematic review. J Orthod. 2005; 32:102-114
Chang HS, Walsh LJ, Freer TJ. Enamel demineralisation during orthodontic treatment. Aetiology and prevention. Aust Dent J. 1997; 42:322-327
Chapman JA, Roberts WE, Eckert GJ, Kula KS, González-Cabezas C. Risk factors for incidence and severity of white spot lesions during treatment with fixed orthodontic appliances. Am J Orthod Dentofacial Orthop. 2010; 138:188-194
Lundström F, Krasse B. Streptococcus mutans and lactobacilli frequency in orthodontic patients; the effect of chlorhexidine treatments. Eur J Orthod. 1987; 9:109-116
Hadler-Olsen S, Sandvik K, El-Agroudi MA, Ogaard B. The incidence of caries and white spot lesions in orthodontically treated adolescents with a comprehensive caries prophylactic regimen – a prospective study. Eur J Orthod. 2012; 34:633-639
Richter AE, Arruda AO, Peters MC, Sohn W. Incidence of caries lesions among patients. Am J Orthod Dentofacial Orthop. 2011; 13:657-664
Enaia M, Bock N, Ruf S. White-spot lesions during multibracket appliance treatment: a challenge for clinical excellence. Am J Orthod Dentofacial Orthop. 2011; 140:17-24
Mandall NA, Matthew S, Fox D, Wright J, Conboy FM, O'Brien KD. Prediction of compliance and completion of orthodontic treatment: are quality of life measures important?. Eur J Orthod. 2008; 30:40-45
Moss JP, Williams DW, Cohen AM. Experience in providing orthodontic treatment in England. Eur J Orthod. 1981; 3:135-139
Cohen AM, Moss JP, Williams DW. Oral hygiene instruction prior to orthodontic treatment. Br Dent J. 1983; 155:277-278
London: Public Health England; 2014
Sjögren K, Birkhed D, Rangmar B. Effect of a modified toothpaste technique on approximal caries in preschool children. Caries Res. 1995; 29:435-441
Deery C, Heanue M, Deacon S The effectiveness of manual versus powered toothbrushes for dental health: a systematic review. J Dent. 2004; 32:197-211
Leeds, UK: Health and Social Care Information Centre; 2015
Eppright M, Shroff B, Best AM, Barcoma E, Lindauer SJ. Influence of active reminders on oral hygiene compliance in orthodontic patients. Angle Orthod. 2014; 84:208-213
Feil PH, Grauer JS, Gadbury-Amyot CC, Kula K, McCunniff MD. Intentional use of the Hawthorne effect to improve oral hygiene compliance in orthodontic patients. J Dent Educ. 2002; 66:1129-1135
Gray D, McIntyre G. Does oral health promotion influence the oral hygiene and gingival health of patients undergoing fixed orthodontic treatment? A systematic literature review. J Orthod. 2008; 35:262-269
Harris R, Gamboa A, Dailey Y, Ashcroft A. One-to-one dietary interventions undertaken in a dental setting to change dietary behaviour. Cochrane Database Syst Rev. 2012; 3 https://doi.org/10.1002/14651858.CD006540.pub2
Benson PE, Parkin N, Dyer F, Millett DT, Furness S, Germain P. Fluorides for the prevention of early tooth decay (demineralised white lesions) during fixed brace treatment. Cochrane Database Syst Rev. 2013; 12 https://doi.org/10.1002/14651858.CD003809.pub3
Stechksén-Blicks C, Renfors G, Oscarson ND, Bergstrand F, Twetman S. Caries-preventive effectiveness of fluoride varnish: a randomized controlled trial in adolescents with fixed orthodontic appliances. Caries Res. 2007; 41:544-549
Øgaard B, Alm AA, Larsson E, Adolfsson U. A prospective, randomized clinical study on the effects of an amine fluoride/stannous fluoride toothpaste/mouthrinse on plaque, gingivitis and initial caries lesion development in orthodontic patients. Eur J Orthod. 2006; 28:8-12
Luther F, Tobin M, Robertson AJ, Toumba KJ. Fluoride releasing glass beads in orthodontic treatment to reduce decay: a randomized, controlled clinical trial. Wld J Orthod. 2005; 6:166-167
Tatsi C, Toumba KJ. Private communication. 2016;
Attin R, Schwestka-Polly R, Wiechmann D. Caries outcomes after orthodontic treatment with fixed appliances: do lingual brackets make a difference?. Eur J Oral Sci. 2010; 118:298-303
Wiechmann D, Klang E, Helms HJ, Knösel M. Lingual appliances reduce the incidence of white spot lesions during orthodontic multi-bracket treatment. J Orthod Dentofacial Orthop. 2015; 14:414-422
Sonis AL, Snell W. An evaluation of a fluoride-releasing, visible light-activated bonding system for orthodontic bracket placement. Am J Orthod Dentofacial Orthop. 1989; 95:306-311
Tüfekçi E, Pennella DR, Mitchell JC, Best AM, Lindauer SJ. Efficacy of a fluoride-releasing orthodontic primer in reducing demineralisation around brackets: an in-vivo study. Am J Orthod Dentofacial Orthop. 2014; 146:207-214
Twetman S, McWilliam JS, Hallgren A, Oliveby A. Cariostatic effect of glass ionomer retained orthodontic appliances. An in vivo study. Swed Dent J. 1997; 21:169-175
Marcusson A, Norevall LI, Persson M. White spot reduction when using glass ionomer cement for bonding in orthodontics: a longitudinal and comparative study. Eur J Orthod. 1997; 19:233-242
Chung CK, Millett DT, Creanor SL, Gilmour WH, Foye RH. Fluoride release and cariostatic ability of a compomer and a resin-modified glass ionomer cement used for orthodontic bonding. J Dent. 1998; 26:533-538
Gorton J, Featherstone JD. In vivo inhibition of demineralisation around orthodontic brackets. Am J Orthod Dentofacial Orthop. 2003; 123:10-14
Pascotto RC, Navarro MF, Capelozza Filho L, Cury JA. In vivo effect of a resin-modified glass ionomer cement on enamel demineralisation around orthodontic brackets. Am J Orthod Dentofacial Orthop. 2004; 125:36-41
Czochrowska E, Ogaard B, Duschner H, Ruben J, Arends J. Cariostatic effect of a light-cured, resin reinforced glass-ionomer for bonding orthodontic brackets in vivo. A combined study using microradiography and confocal laser scanning microscopy. J Orofac Orthop. 1998; 59:265-273
Millett DT, McCluskey LA, McAuley F, Creanor SL, Newell J, Love J. A comparative clinical trial of a compomer and a resin adhesive for orthodontic bonding. Angle Orthod. 2000; 70:233-240
Gillgrass TJ, Benington PC, Millett DT, Newell J, Gilmour WH. Modified composite or conventional glass ionomer for band cementation? A comparative clinical trial. Am J Orthod Dentofacial Orthop. 2001; 120:49-53
Benham AW, Campbell PM, Buschang PH. Effectiveness of pit and fissure sealants in reducing white spot lesions during orthodontic treatment. Angle Orthod. 2009; 79:338-345
The prevalence of demineralization, or enamel caries which is the first clinically recognizable stage of caries, has been reported to be as high as 73% during fixed appliance treatment. It is recognized that wearing an orthodontic appliance increases the caries risk of the individual. The orthodontist can effectively reduce demineralization by applying fluoride varnish at each visit. Selecting patients on their oral hygiene clearly is one factor which can prevent patients suffering from demineralization. Excellent home care with optimal use of fluoride will also help prevent the condition. There is little evidence that fluoride-releasing materials used for bonding orthodontic appliances offer protection from demineralization. The first of these two papers describes the aetiology, prevalence and prevention of demineralization associated with orthodontic care. The second paper will describe the treatments available to manage caries focusing on demineralization post orthodontic treatment.
CPD/Clinical Relevance: Demineralization is the most common complication of orthodontic care. The clinician should understand how to prevent this.
Article
Orthodontic care involves the practitioner in an assessment of a number of risks and benefits. It would be inappropriate to continue treatment when unexpected complications, poor patient compliance or behaviour leads to detrimental effects for the patient as a result of orthodontic treatment.1 One of the most commonly recognized complications of orthodontic care is demineralization due to poor oral hygiene. Demineralization is enamel caries and is the first clinically recognizable stage of caries. Although such lesions can develop irrespective of orthodontic treatment, it has been shown to be a recognized complication of orthodontic treatment.2
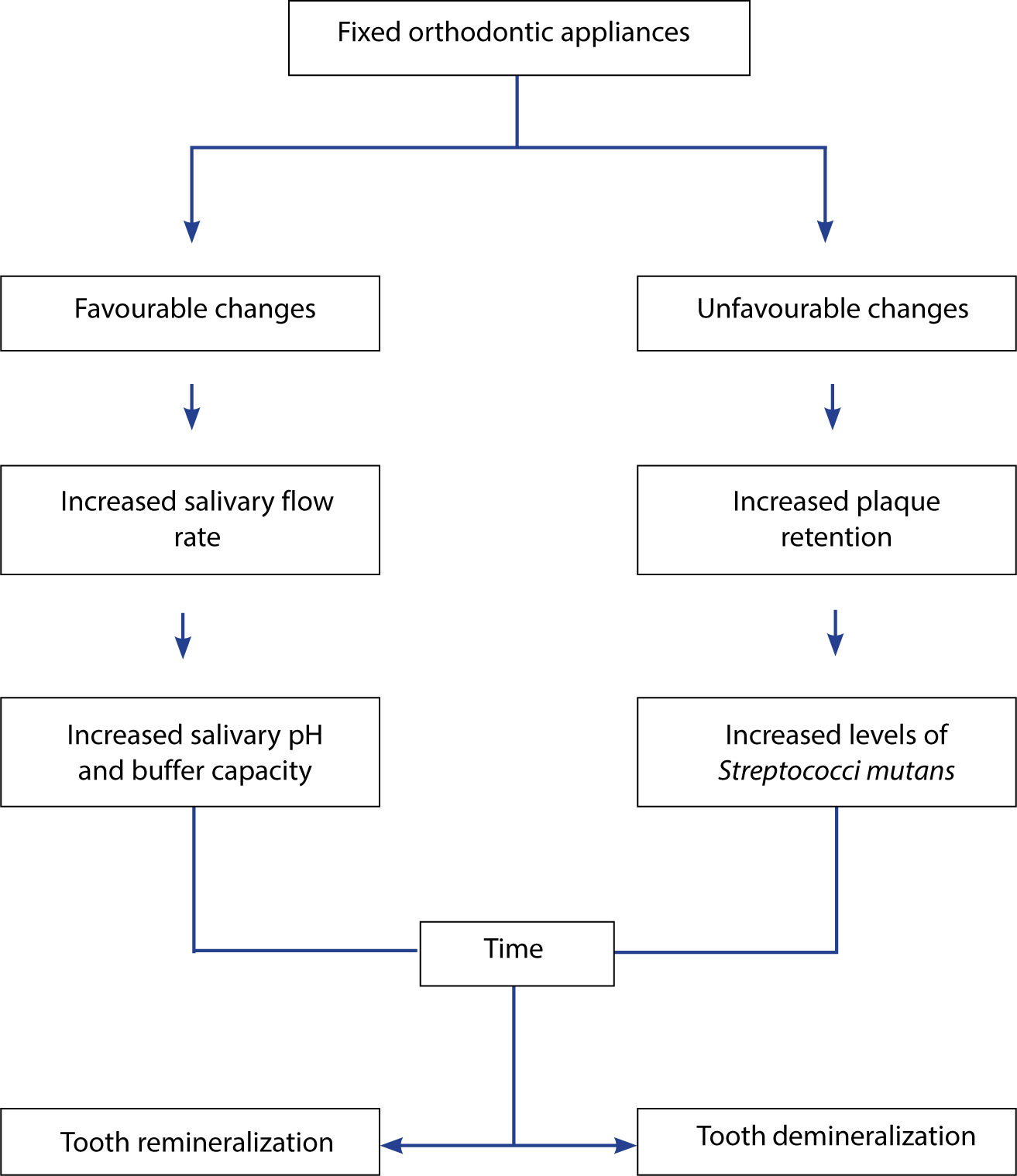
Introducing fixed or removable orthodontic appliances to the oral environment alters the ecology of the mouth by adding another variable to the system. Figure 1 shows a proposed hypothesis suggested by Chang et al of the influences orthodontic appliances may have on the process of enamel demineralization.3
Figure 1. A hypothesis of the influences orthodontic appliances can have on the process of enamel demineralization. (after Chang et al3)
The practitioner will wish to avoid iatrogenic damage by identifying patients at risk of caries before commencing care. For example, male patients at a pre-adolescent age at the time of treatment, patients with fair or poor pre-treatment oral hygiene, a higher number of treatment appointments and white ancestry have all been shown to be associated with a greater incidence and severity of white spot lesions during orthodontic care.4
Increased levels of Streptococcus mutans and lactobacilli, among other members of the oral biofilm, are linked with greater caries risk and activity. Salivary levels of S. mutans and lactobacilli increase significantly during the first six months of active orthodontic treatment in spite of oral hygiene and dietary advice instruction.5
Demineralization of enamel adjacent to orthodontic brackets is generally caused by poor oral hygiene and diet, compared to carious lesions found beneath orthodontic bands, which is more likely as a result of improper band cementation, loosening of the orthodontic band and unrestored cavities. Fixed orthodontic appliances increase the number of plaque retentive sites on teeth and increase the caries predilection sites that are usually less susceptible to caries development and make conventional oral hygiene methods even more challenging.3Figure 2 shows a fixed appliance with associated plaque accumulation because of poor oral hygiene.
Figure 2. A fixed appliance with associated plaque accumulation due to poor oral hygiene.
Prevalence
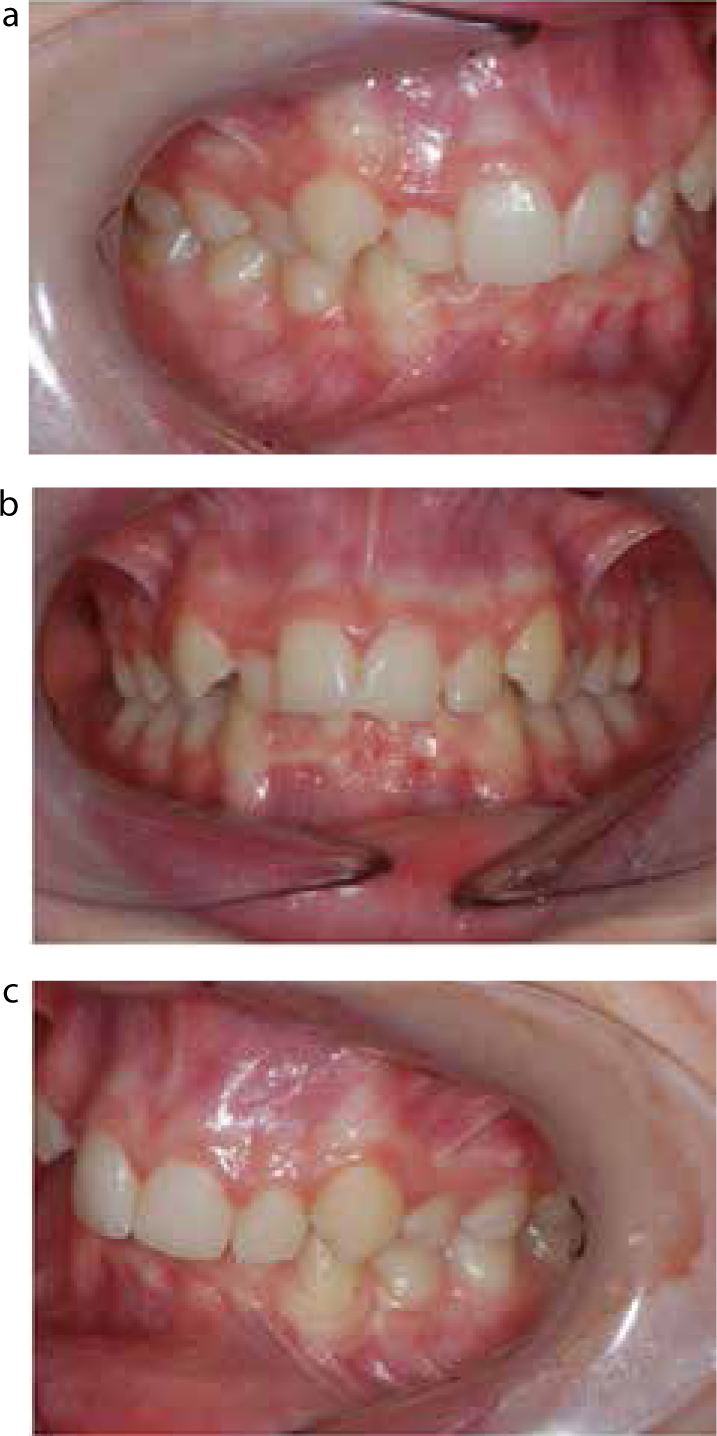
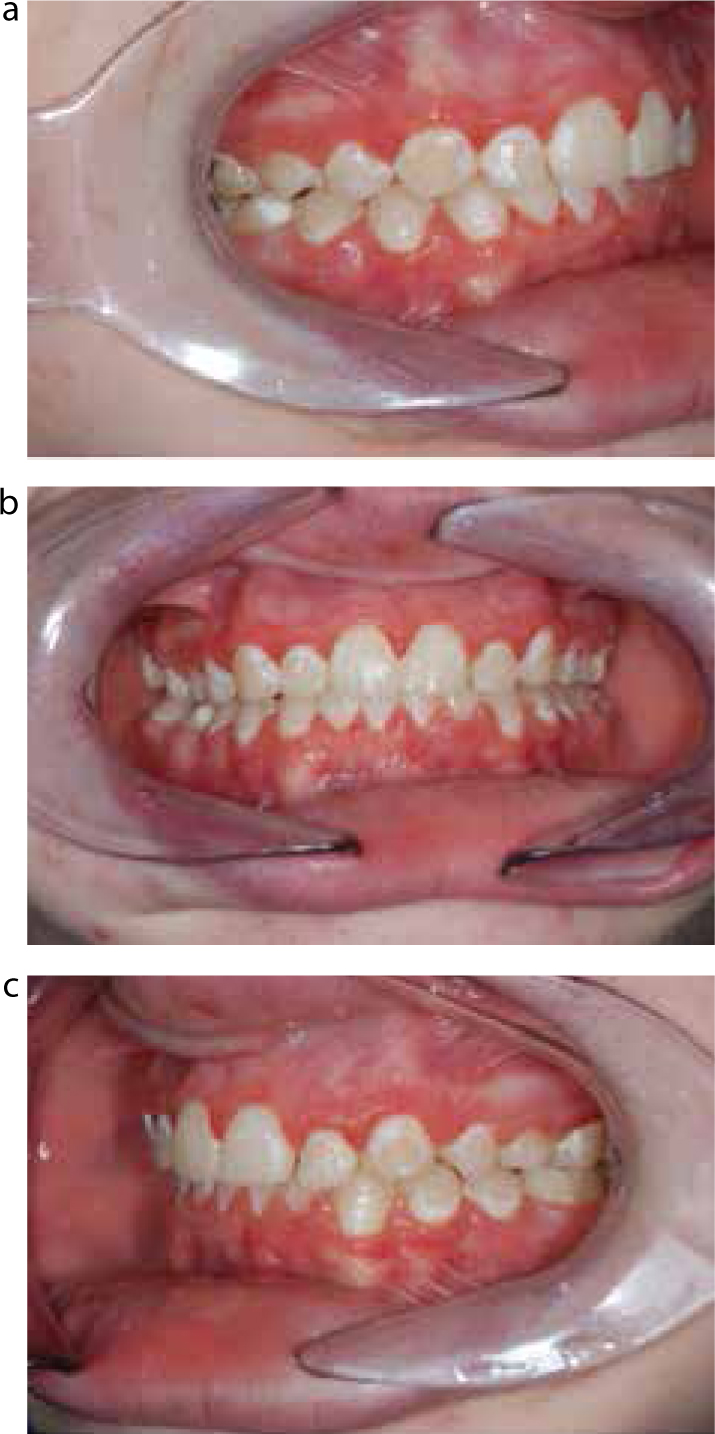
Demineralization of enamel and occasional dentine caries with cavitation is a recognized risk factor of orthodontic treatment. Figures 3 and 4 show dentinal caries in two patients who were wearing a removable appliance. Figure 5 shows a patient prior to fixed orthodontic care and Figure 6 shows demineralization in the same patient after debonding. Figure 7 is an example of more advanced dentinal and enamel caries as a result of wearing a fixed appliance together with poor oral hygiene and probably a cariogenic diet.
Figure 3. Palatal caries in a patient wearing a removable appliance, with an anterior bite plane.Figure 4. Buccal caries associated with the Adam's Clasp of a removable appliance.Figure 5.
(a, b) A patient prior to fixed orthodontic care. (c) Visible food debris is visible on the left-hand side.Figure 6.
(a–c) Demineralization in the same patient as in Figure 5 after debonding of the appliance.Figure 7. Enamel and dentine caries associated with the wearing of a fixed appliance.
It has been shown that patients undergoing fixed orthodontic treatment are at a higher risk of developing white spot lesions when compared to patients without. A study comparing 40 adolescents receiving fixed appliances with 40 matched controls showed a resultant mean increase of white spot lesions of 1.9 in the orthodontic group compared to 0.4 in the control.6 The increase in dentine caries in both groups were similar, with a mean increase of 0.5 in the orthodontic group compared with 0.7 lesions in the control. Studies have shown the incidence of developing white spot lesions during fixed appliance treatment to be as high as 73%, with 2.3% of patients developing cavities.7
A study looking into the incidence of white spot lesions in 400 patients wearing multi-bracket appliances for at least one year and with a retention period of at least one year showed that, after treatment, 73% had lesions on the labial surface of their upper incisors. Of these, 63.3% had mild demineralized lesions, 26.9% had severe lesions and 9.9% had resultant cavities. It is interesting to note that the incidence of cavities was higher than reported in the aforementioned study. Following the retention phase of treatment, 57.1% showed improvement in the white spot lesions, however, 16.7% had deteriorated further.8
There is a significantly high incidence of white spot lesions therefore developing as a result of orthodontic treatment, and the clinician and patient must be aware of this risk. Prevention pre-operatively, as well as during fixed orthodontic appliance treatment, is paramount.
Prevention
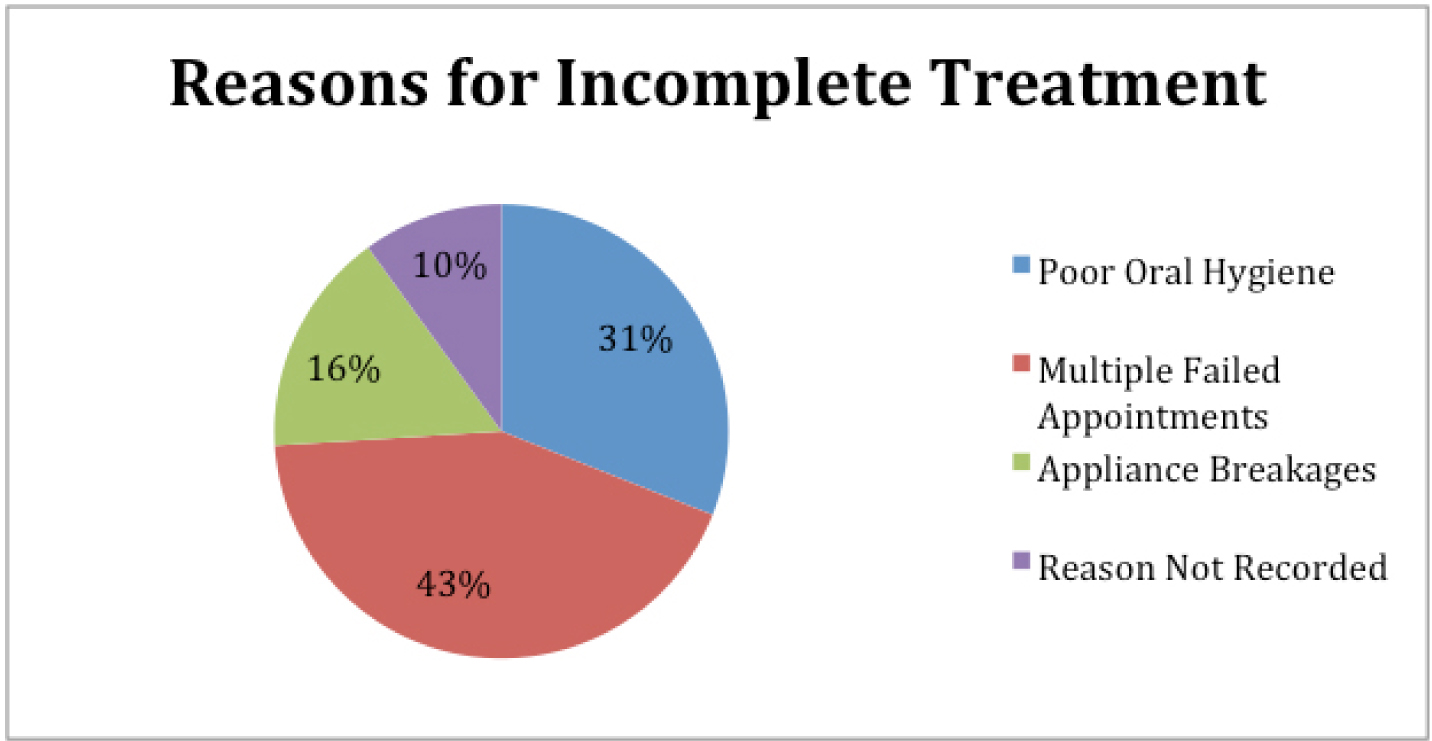
Unfortunately, for some the only preventive action is to discontinue treatment prematurely, however, it would clearly be better to avoid this if possible. Mandall et al measured compliance with orthodontic treatment together with the reason for non-completion.9 The reasons identified included poor oral hygiene, failed appointments and appliance breakages. This study incorporated 144 patients (aged 10–19 years), out of which a high number, 62 (43%), had their treatment abandoned. Figure 8 shows the categorization of the main reasons for incomplete treatment. Poor oral hygiene and multiple failed appointments are the main reasons for orthodontic treatment being left incomplete. Unfortunately, this study also reported that clinical treatment need (IOTN), baseline quality of life measures, age, gender or socio-economic status were not predictors of successful completion of treatment.
Figure 8. Reasons for abandonment of orthodontic treatment (n = 144) (after Mandall et al9).
A recent study by Chapman et al did identify risk factors for the development of demineralization during orthodontic treatment. These included:
Pre-adolescent children at the outset;
The number of times poor oral hygiene was documented throughout the course of treatment;
White ethnic groups; and
Inadequate oral hygiene at pre-treatment assessment appointments.4
Oral hygiene
Studies have shown that only permitting patients who achieve an adequate level of oral hygiene to commence active appliance therapy reduced the number of terminated treatments.10,11
As orthodontic patients are at a greater risk of developing caries, all patients should be educated and motivated to achieve excellent oral hygiene, implementing the use of high fluoridated toothpastes, fluoride mouthwashes and varnishes.
The Delivering Better Oral Health toolkit advises that brushing should be carried out at least twice a day and indicates that the most beneficial time of day to brush teeth is at night before bed.12 Thorough cleaning takes at least two minutes and therefore three minutes brushing is what should be advised to patients.
Though the toolkit states that no particular technique of brushing has been shown to be superior to any others, emphasis should be made to clean all tooth surfaces in a systematic approach. Many orthodontists and hygienists recommend that patients use single tufted brushes to improve access around the appliance (Figure 9). It also advises that rinsing with water or mouthrinses immediately after toothbrushing will dilute the concentration of fluoride. Rinsing after brushing should therefore be discouraged and spitting out excess toothpaste instead should be advised. A modified fluoride toothpaste technique, where a ‘slurry rinse’ with toothpaste is carried out after brushing, has been shown to increase the efficacy of fluoridated toothpaste alone in young children.13 This has been suggested for orthodontic patients but there are no clinical trials to support its use.
Figure 9. Single-tufted brush to improve access for cleaning.
A Cochrane Systematic Review compared powered toothbrushes with manual brushes and reported powered brushes reduced plaque levels and gingivitis.14 The rotating oscillating design was the only design of powered brush to be statistically significantly superior at all time points. A previous iteration of this review attempted to identify if powered brushes had any benefit for patients wearing fixed appliances, and if these had any drawbacks such as increased breakages but, due to the small number of studies, was unable to draw conclusions.15
According to the Children's Dental Health Survey (2013), the proportion of children brushing their teeth twice a day has remained relatively stable since 2003.16
Compliance with oral hygiene regimens has been an ongoing battle for clinicians. However, modern technology offers new opportunities.17 In one study, the parents of 42 orthodontic patients received weekly text messages prompting oral hygiene. Oral hygiene significantly improved as measured by the Bleeding Index, Modified Gingival Index, Plaque Index and visual examination of white spot lesions, in those receiving the texts compared to the controls, who did not receive text messages.
Knowing that you are being observed has an influence on behaviour; this is known as the Hawthorne effect. In a recent study, 40 patients with a history of poor oral hygiene were randomized into two groups, one being given the impression that they were part of a research project and the other acting as a control.18 The experimental group believed that they were part of a research study because they were given consent forms, received toothpaste labelled ‘experimental’ and instructions to brush their teeth twice a day for 2 minutes. The control group received no intervention. In the experimental group, the plaque level significantly reduced from an initial 71% to 52% at 6 months, while plaque levels for the control group increased from 74% to 79%. Whether this approach is truly ethical or applicable to everyday practice is questionable.
Finally, a systematic review of oral hygiene advice in orthodontic patients identified only six small trials.19 They concluded that an oral hygiene promotion programme produces a short term, five month improvement in plaque level and gingival health.
Diet advice
Orthodontists advise patients about cariogenic diets and, to avoid breakages, the avoidance of sticky foodstuffs. It is important to recognize that honey, fruit smoothies, fresh fruit juices and dried fruits all contain cariogenic sugars and therefore advice should be given to patients to reduce the frequency of these, if present in their diet, as many patients consider these and other items ‘healthy choices’. It must be recognized that the evidence for the effectiveness of dietary advice in terms of sugar reduction is weak.20 However, it seems only sensible to advise a reduction both in the amount and frequency of consuming foods and drinks that contain non-milk extrinsic sugars.
Topical fluoride
Topical fluoride application on teeth has been a longstanding proven method of reducing the risk of dental caries, and therefore this form of treatment should protect patients from demineralized areas during their fixed orthodontic appliance treatment.
A Cochrane Systematic Review assessed the evidence for the effectiveness of fluoride in preventing dental caries during orthodontic treatment.21 Three studies with 458 participants were included in the review:
Fluoride varnish versus placebo varnish;
Different formulations of fluoride toothpaste and mouthwash;
Fluoride-releasing component attached to the braces versus mouthwash.
The most robust study (273 patients, aged 12–15 years) reduced the risk of demineralization by nearly 70%.22 This involved orthodontists placing fluoride varnish around the teeth and appliance each time the appliance was adjusted, whilst the control group had a placebo varnish placed. Figure 10 shows 5% sodium fluoride varnish being applied at a visit to adjust the appliance.
Figure 10. One of the most effective interventions to prevent demineralization: 5% sodium fluoride varnish being applied at a visit to adjust the appliance.22
Another study compared two patient groups receiving different formulations of fluoride. One group was allocated amine fluoride/stannous fluoride toothpaste and mouthrinse and the other sodium fluoride toothpaste and mouthrinse.23 This study found that there was an increase in the number of white spot lesions from baseline in the sodium fluoride group but not the amine fluoride group, suggesting that the amine fluoride/stannous fluoride combination is more effective. There was also a slightly larger increase in visible plaque and gingival bleeding index in the group prescribed sodium fluoride. However, the significance of these findings does need to be interpreted with caution as it was reported that caries increment was low, at 4.3% and 7.2%, respectively.
A smaller study, of only 37 patients, compared the use of fluoride-releasing glass beads attached to the braces versus daily fluoride mouthwashes.24 The experimental group received a carbonate-based bead containing 13.3% fluoride and the control group was asked to use a daily fluoride mouthrinse (0.05% NaF). The findings showed that the glass beads were very fragile and 18 were reported broken. As the study was small and assessed as having a high risk of bias, there was insufficient evidence to determine whether the beads were more or less effective than mouthrinses in reducing white spot lesions. The results of a recent, as yet unpublished, study with a redesigned version of the bead suggest that the problem with breakages has been overcome and the placement of these fluoride slow release devices is effective at preventing demineralization during fixed appliance therapy.25
Buccal surfaces of teeth are regarded as being more caries prone than lingual surfaces and therefore using lingual orthodontic brackets to inhibit white spot lesions can be considered as a viable option. A small (28 subjects) randomized control trial using a split-mouth approach looked into the incidence of white spot lesions, where subjects were randomly allocated into a group receiving buccal or lingual brackets on the maxillary teeth and the contrasting brackets on the mandibular teeth. The number of early enamel lesions that developed or progressed on buccal surfaces was found to be 4.8 times greater than the number that appeared on the lingual surfaces, as measured by quantitative, light-induced fluorescence.26,27
Fluoride-releasing materials
A Cochrane Systematic Review looked into the effect of using fluoride-containing materials. These included fluoride-releasing composite bonding materials; glass ionomer cements (GIC), compomers and resin-modified GICs. The majority of the studies were small and had other methodological limitations which meant that they were excluded from the subsequent review.21 The summaries below give a feel for these studies.
One split mouth controlled clinical trial with 22 patients compared a light-activated, fluoride-releasing composite with a conventional light-activated, non-fluoridated composite control.28 More decalcification was observed in the control group involving four patients, compared to no decalcification noted in the experimental group. However, a later trial of a fluoride-releasing primer versus a non-fluoride releasing primer demonstrated no difference.29
Six studies compared GIC (fluoride group) and composite (non-fluoride group) for their use in bonding brackets. Out of the six trials, half showed no significant difference between using GIC-containing fluoride and the composite control group in the level of demineralization. Three studies, all with minimal risk of bias, showed a significant increase in mineral loss in the composite control group in comparison to using GICs.30,31,32,33,34,35
No statistically significant difference in the degree of demineralization was found between two fluoride-releasing materials, GIC and compomer, nor were these materials found individually to be superior to resin in terms of reduced demineralization.32 When these materials were considered together, however, and when compared with the resin group, there was a significant benefit. This suggests that the trial was underpowered, as is the case with many of the trials looking at the effect of materials on demineralization.
Similar results were reported by Millett et al, who showed that the percentage of teeth affected by demineralization was significantly better for compomer than composite.36 However, a larger trial (98 subjects) conducted by Gillgrass et al, comparing conventional GIC with composite, found no statistically significant difference between the two cement groups.37
A trial that compared fluoridated modules with non-fluoridated ones, though the number of lesions were high (31 out of 49 in the fluoridated group and 33 out of 45 in the non-fluoridated elastics group), found no significant difference between the two, with the study being rated as having a high risk of bias.38
The application of resin sealant on the enamel surfaces surrounding orthodontic brackets should protect the enamel surface from demineralization. A randomized split mouth study with 60 adolescent patients aged between 11 and 16 years reported six lesions were identified on the teeth with sealants compared to 22 on the teeth without. This made the teeth without sealants almost four times more likely to develop white spot lesions.39
Conclusion
Despite recent advances in dental materials and methods to reduce the incidence of enamel demineralization, studies indicate that the development of white spot lesions continues to be a significant problem amongst orthodontic patients. The incidence of developing at least one white spot lesion during multi-bracket orthodontic treatment has been reported to be as high as 73%.7,8
The prevention of demineralization relies on selecting motivated patients with excellent oral hygiene at the outset. There is a benefit from the optimal use of fluoride, including mouthrinses in addition to toothbrushing. There is also evidence that fluoride varnish should be applied at each appliance adjustment visit.22
The second of these papers will discuss the management of white spot lesions when they do occur.