Ando S, Aizaea K, Nakashima T, Sanka Y, Shimbo K, Kiyokawa K Transmigration process of impacted mandibular cuspid. J Nihon Univ Sch Dent. 1964; 6:66-71
Tarsitano JJ, Wooten JW, Burditt JT Transmigration of nonerupted mandibular canines: report of cases. J Am Dent Assoc. 1971; 82:1395-1397
Javid B Transmigration of impacted mandibular cuspids. Int J Oral Surg. 1985; 14:547-549
Joshi MR Transmigrant mandibular canines: a record of 28 cases and a retrospective review of the literature. Angle Orthod. 2001; 71:12-22
Alaejos-Algarra C, Berini-Aytés L, Gay-Escoda C Transmigration of mandibular canines: report of six cases and review of the literature. Quintessence Int. 1998; 29:395-398
Lagares DT, Ruiz RF, Cossío PI, Calderón MG, Gutiérrez Pérez JL Transmigration of impacted lower canine. Case report and review of literature. Med Oral Patol Oral Cir Bucal. 2006; 1:E171-E174
Shapira Y, Kuftinec M Intrabony migration of impacted teeth. Angle Orthod. 2003; 7:738-743
Shapira Y, Mischler WA, Kuftinec MM The displaced mandibular canine. ASDC J Dent Child. 1982; 49:362-364
Fiedler LD, Alling CC Malpositioned mandibular right canine: report of a case. J Oral Surg. 1968; 26:405-407
Howard RD The anomalous mandibular canine. Br J Orthod. 1976; 3:117-121
Greenberg S, Orlian A Ectopic movement of an unerupted mandibular canine. J Am Dent Assoc. 1976; 93:125-128
Vichi M, Franchi L, Bassarelli V Contributo clinico sulla transmigrazione del canino inferiore permanente. Minerva Stomatol. 1991; 40:579-589
Aydin U, Yilmaz HH Transmigration of impacted canines. Dentomaxillofac Radiol. 2003; 32:198-200
Costello J, Worth J, Jones A Transmigration of permanent mandibular canines. Br Dent J. 1996; 181:212-213
Caldwell JB Neurological anatomy associated with extreme malposition of the mandibular canine. Oral Surg Oral Med Oral Pathol. 1955; 8:484-487
Kuftinec MM, Shapira Y, Nahlieli O A case report: bilateral transmigration of impacted mandibular canines. J Am Dent Assoc. 1995; 126:1022-1024
Mupparapu M Patterns of intra-osseous transmigration and ectopic eruption of mandibular canines: review of literature and report of nine additional cases. Dentomaxillofac Radiol. 2002; 31:355-360
Thoma KH, 2nd edn. St Louis: CV Mosby; 1952
Wertz RA Transmigrated mandibular canines. Am J Orthod Dentofacial Orthop. 1994; 106:419-427
Al-Waheidi E Transmigration of unerupted mandibular canines: a literature review and a report of five cases. Quintessence Int. 1996; 27:27-31
Bruszt P Neurological anomaly associated with extreme malposition of a mandibular canine. Oral Surg Oral Med Oral Pathol. 1958; 11:89-90
Taguchi Y, Kurol J, Kobayashi H, Noda T Eruption disturbances of mandibular permanent canines in Japanese children. Int J Paediatr Dent. 2001; 11:98-102
Joshi MR, Shetye SB Transmigration of mandibular canines - a review of the literature and report of two cases. Quintessence Int. 1994; 25:291-294
Mitchell L Displacement of a mandibular canine following fracture of the mandible. Br Dent J. 1993; 174:417-418
Marks SCJ, Schroeder HE Tooth eruption: theories and facts. Anat Rec. 1996; 245:374-393
Baccetti T A controlled study of associated dental anomalies. Angle Orthod. 1998; 68:267-274
Peck S On the phenomenon of intraosseous migration of non-erupting teeth. Am J Orthod Dentofacial Orthop. 1998; 113:515-517
Baykul T, Heybeli N, Oyar O, Doğru H Multiple huge osteomas of the mandible causing disfigurement related with Gardner's syndrome: case report. Auris Nasus Larynx. 2003; 30:447-451
Camileri S, Scerri E Transmigration of mandibular canines: a review of the literature and a report of five cases. Angle Orthod. 2003; 73:753-762
A review of the literature relating to transmigrating canines. An illustrated case report Gargi S Sarode Anuprita Patil Orthodontic Update 2025 4:2, 56-60.
Authors
Gargi SSarode
MDS
Senior Lecturer, Department of Oral Pathology and Microbiology
Canine impaction is not an uncommon finding in the dental literature, but transmigration of mandibular canines is a rare phenomenon, and some of them are far more extreme than others. We report an extremely rare case of bilateral transmigration of impacted permanent canines crossing the midline of the mandible.
Clinical Relevance: To understand the role of early interception so that the patient can be treated before canines transmigrate in order to avoid surgical extraction, as well as complex orthodontic and restorative therapies.
Article
Transmigration is the movement of an impacted tooth across the midline. Several terms have been used, such as anomalous, malpositioned or displaced tooth, although in 1964, Ando et al1 were the first to use the more widely accepted term, ‘transmigration’, which is perhaps the most appropriate term. In 1971, Tarsitano et al2 used the term ‘transmigration’ to describe the displacement and migration of an impacted tooth across the midline to the opposite side of the jaw. Later, Javid3 expanded the definition to include cases in which more than half of the tooth had passed through the midline. However, Joshi4 felt that the tendency of a canine to cross the barrier of the mandibular midline suture is a more important consideration than the distance travelled. Moreover, the stage of transmigration of the tooth at the time of examination is a determining factor in the distance travelled. Such displacement may occur spontaneously, or as a result of a localized pathological lesion.
Studies have suggested that transmigration of canines is a rare phenomenon, with an incidence of 0.31%.5 The incidence of transmigrated canines is normally higher in females than in males, with a ratio of 2:1. However, according to some reviews, this difference is less.6 The mandibular left quadrant is affected more than the right quadrant.7 Patients presenting transmigration range between the ages of 8 and 62 years old.6
The mandibular permanent canine is the only tooth in the dental arch reported to migrate across the symphyseal midline to the contralateral side. Dental literature includes several case reports of unilateral transmigration of impacted mandibular canines,2,3,8,9,10,11,12,13 some more severe than others. However, bilateral transmigration of impacted mandibular canines across the midline and along the lower border of the mandible is extremely rare.3,14,15,16,17 The authors report a rare case of bilateral transmigration of canines with a comprehensive review of the literature.
Case report
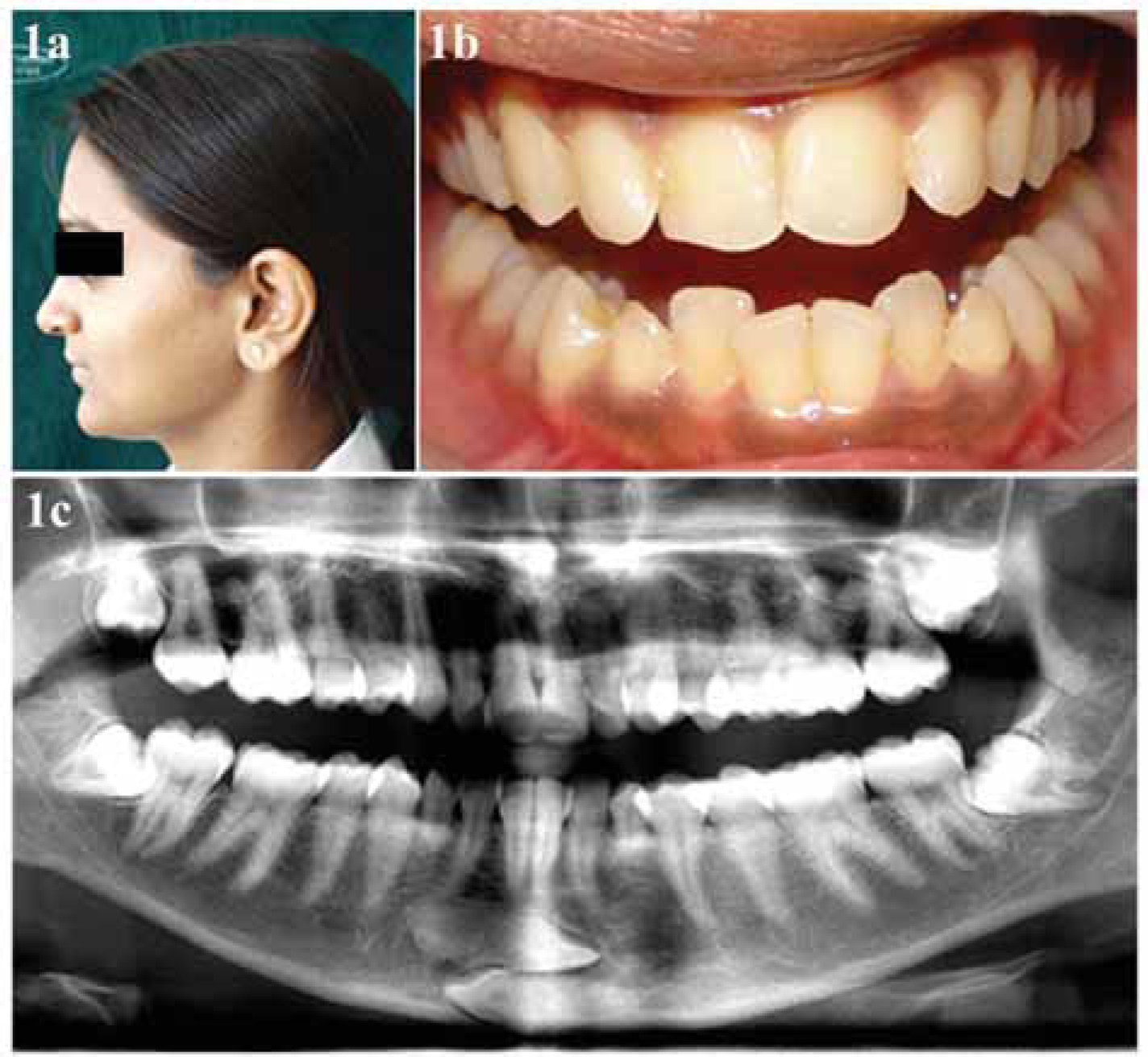
A 21-year-old female reported for a routine dental check-up. On intra-oral examination there were bilaterally retained mandibular deciduous canines (Figure 1 a, b). Further investigation of the panoramic radiograph showed both the permanent canines lying horizontally, one above the other, at the lower border of mandible, crossing the symphyseal midline. The left canine was lying above the right one, which was adjacent to the lower border of the mandible (Figure 1c). Both canines seemed to be rotated with their lingual surfaces facing occlusally, and both were situated anterior to the incisor roots. The diagnosis of transmigrated canines was made. The patient was not willing to undergo any surgical treatment and was kept under observation.
The occurrence of impacted mandibular canines is rarer than maxillary canines, with a ratio of 1:20,4 and even rarer when such an impacted mandibular canine migrates to the other side of the mandible, crossing the mandibular midline.
One reason given for the higher frequency of mandibular canine transmigration may be the larger cross-sectional area of the anterior mandible compared with the anterior maxilla.18 Transmigration of maxillary canines is uncommon owing to the shorter distance between the roots of maxillary incisors and the floor of the nasal fossa, and restriction of the path of tooth movement by the roots of adjacent teeth, the maxillary sinus and the mid-palatal suture, which act as barriers.19 Mandibular structure, however, consists of spongy bone inbetween two cortical plates, and explains why the mandibular canine transmigrates while the maxillary does not, because of the dense palatine bone. In doing so, the mandibular canine usually travels along the labial side of the incisor roots. It has been found to migrate as far as the roots of the first molar on the opposite side.20 As with previously reported cases of bilateral transmigration,14,15 our case shows impacted canines crossing the midline one above the other. It appears that they are impeded and unable to migrate past the lateral incisor roots on the opposite side, possibly owing to the limited space available on the curve between the anterior and posterior regions of the mandible.21 There are very few reported cases of bilateral transmigration in which canines have moved to contralateral sides, with their crown tips distal to the lateral incisor roots region, as seen in the present case.
Classification
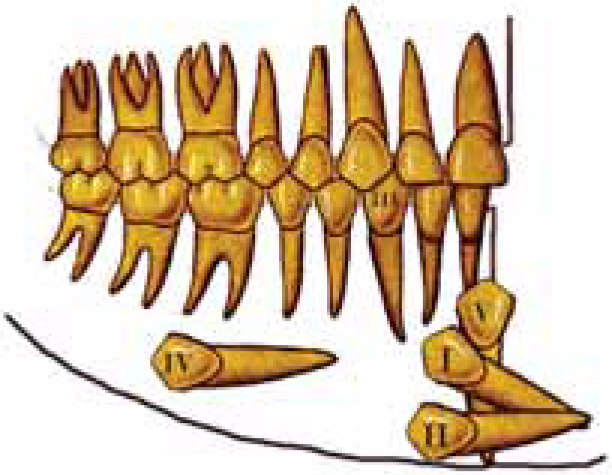
According to Mupparapu,22 transmigrated mandibular canines can be classified and summarized as follows (Figure 2):
Type 1: The impacted canine is mesioangularly crossing the midline, labial or lingual to the anterior teeth, with the crown portion of the tooth crossing the midline.
Type 2: The canine is horizontally impacted near the inferior border of the mandible below the apices of the incisors.
Type 3: The canine has erupted either mesial or distal to the opposite canine.
Type 4: The canine is horizontally impacted near the inferior border of the mandible below the apices of either premolars or molars on the opposite side.
Type 5: The canine is positioned vertically in the midline with the long axis of the tooth crossing the midline.
Figure 2. Mupparapu's classification of transmigrated mandibular canines.22
Mupparapu's classification consists of single transmigrated canines. In the case presented here, there are bilateral impacted canines in a horizontal position located in the midline near the inferior border of the mandible below the apices of the incisors. This is in accordance with Type 2. Mupparapu's Type 1, followed by Type 2, is the most frequently occurring pattern. Type 4 (incidence is 1.5%) and Type 3 occur less frequently, while Type 5 is the least frequently occurring type.22
Aetiopathogenesis
The cause of such rare behaviour is not yet known and there are many hypotheses surrounding it. Many pathological conditions have been proposed as aetiological factors for the canine transmigration (Table 1), but it is not possible to postulate if they are responsible for the transmigration or they occur after the canine is migrated.
Authors
Proposed Aetiological Factors
Thoma23; Fiedler and Alling9; Greenberg and Orlian11; Wertz24; Al-Waheidi25
Obstruction for eruption; Extreme length of crown; Labial inclination of lower incisors; Osteodental discrepancy; Endocrinopathy; Trauma
Camileri and Scerri34 described a development pattern of transmigration as follows:
Development and eruption initially appear normal.
The tooth deviates from its path for no apparent reason.
Transmigration: the greatest amount of the movement occurs during the pubertal age and the movement is usually in a mesial direction.
Occlusal movement of the tooth ceases. A mesial and apical path of movement is established, which worsens with time. The tooth becomes progressively buried as alveolar growth continues. The canine movement was more rapid before the root formation was completed.
Ando et al1, Camileri and Scerri,34 Stafne35 and Sutton36 observed that the migration is rapid before the root formation is completed. It has been pointed out that the tooth always moves in the crown direction. Dhooria et al37 noted that the tooth movement was more rapid (3 to 4 mm per year) after the complete root formation. Howard10 suggested that the older the patient, the more distant is the canine from the midline, because the age increases the available time for the migration. Some authors suggested that the canine germ originates remote from the normal site of eruption; however, all the available evidence shows that the germ develops on the typical side and then migrates to an ectopic position. Transmigration of the mandibular canine is associated with an increased prevalence of other inherited dental anomalies, supporting Peck's opinion that the aetiology of ectopic man dibular canines is genetic.
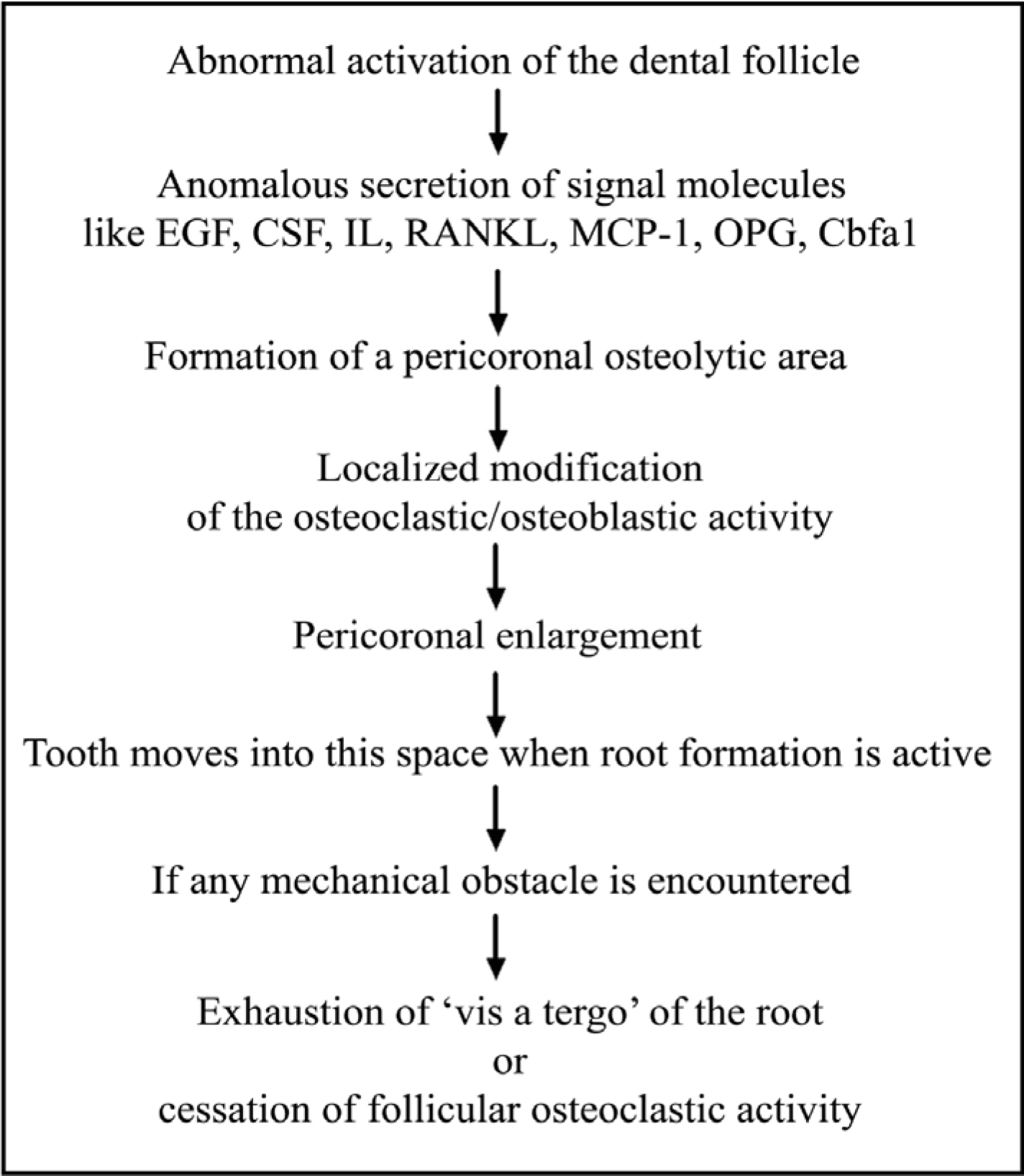
A proposed pathogenetic theory about the intraosseous migration of canines is shown in Figure 3.38
Figure 3. Pathogenetic theory of transmigration of canine proposed by Pippi and Kaitsas.38
Two different and contemporary factors are necessary to justify tooth movement:
A strong and extended ‘vis a tergo’, caused by a lasting root formation.
A pericoronal osteolitic area, owing to a widening follicular space.
Such movements are facilitated by a voluminous mandibular symphysis, buccal inclination of the lower incisors, and the typical conical shape of the canine root and crown.
A consensus on the exact mechanism of transmigration has not been reached in the literature. As a consequence, further studies may include genetic research.
Treatment
The presence of transmigration must be suspected if:
The lower canine is absent from the arch;
If the canine has not erupted more than a year after the normal age of eruption; or
If there is deviation from the midline.
In some cases, agenesis of the lateral incisors and lower premolars has been detected.
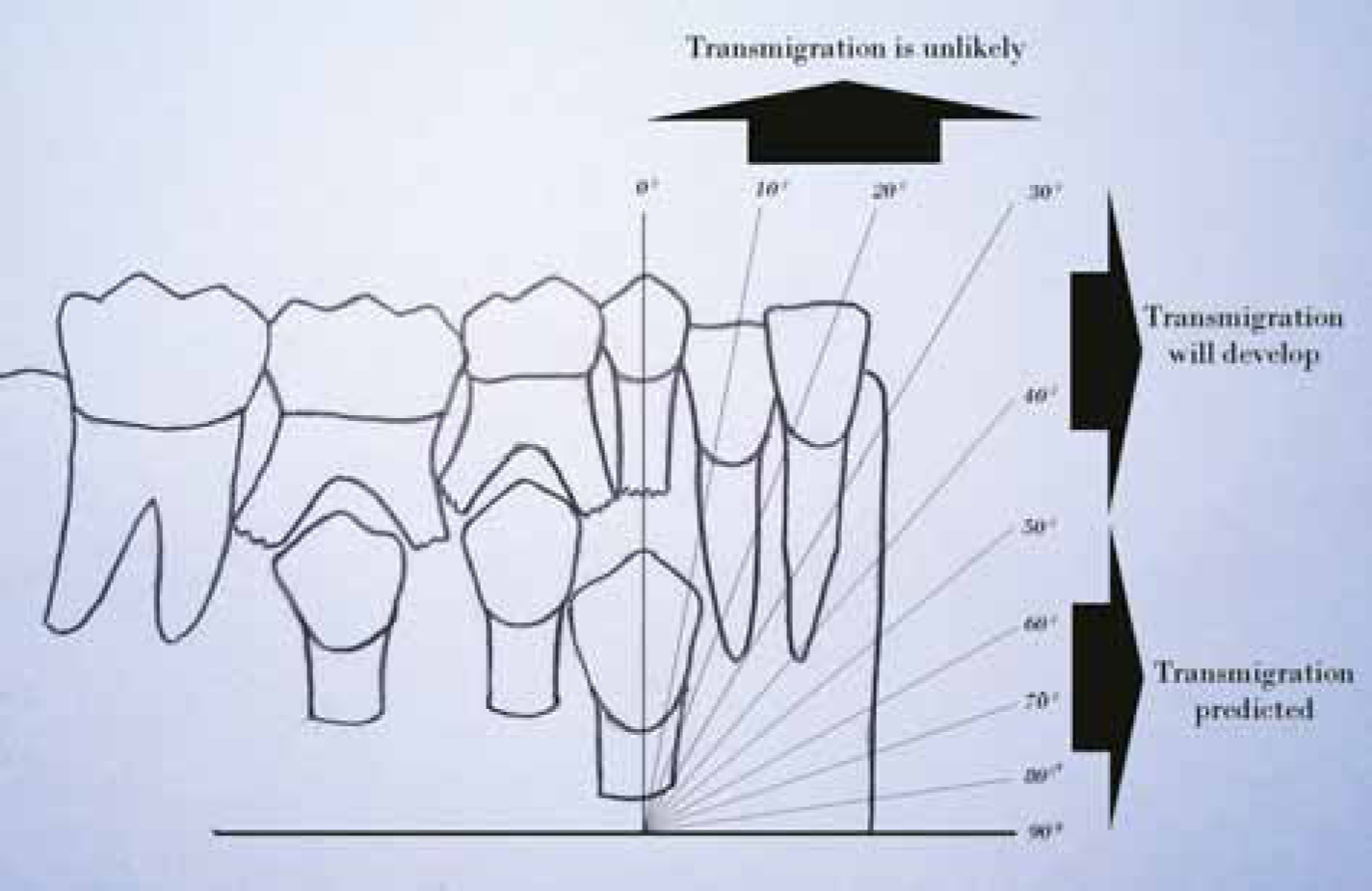
With respect to the treatment of transmigrated canines, interceptive treatment should be carried out, although it is extremely difficult, if not impossible, to predict the occurrence of this anomaly. There is often a difference of some years between a normal orthopantomograph and another in which transmigration of the canine is established. For Joshi4, predicting the appearance of the profile depends on the inclination that the canine tooth germ presents. If the angle formed by the mid-sagittal plane and the dental axis exceeds 50°, transmigration is predictable; if an angle between 30°–50° is formed, it is possible that transmigration will develop, and transmigration is unlikely if it does not exceed 30° (Figure 4).4
Figure 4. Prediction of transmigration of mandibular canine based on inclination of its tooth germ.4
With regard to interception, it is best to detect the patient's presenting characteristics, most related to transmigration, when he/she is between 8 and 9 years old, and these patients should undergo a clinical radiology examination so that urgent action can be taken.4 This ensures a significantly greater number of treatment options, the most suitable being remedial surgery through surgical repositioning, autotransplantation or surgical/orthodontic treatment, after assessing the individual characteristics of the patient, location and inclination of the tooth.10 Mixed dentition radiographs might help to predict the chances of the transmigration of a canine, taking into consideration the eruption pattern of the adjacent teeth. Prevention is better than cure. Hence, if any adjacent teeth cause obstruction, then they should be extracted to assist the correct eruption of the canine.
Once transmigration is established, it is difficult to carry out remedial surgery or orthodontic repositioning (if the tooth has erupted), although this possibility should not be ruled out. However, in such situations, extracting the impacted tooth is the most favoured treatment. The tooth maintains its nervous innervation on the side where the germ is formed. This must be taken into account if the tooth is extracted under local anaesthesia.20
A final treatment option in these patients is observation and clinical check-ups, with radiographs taken periodically. In patients under 14 years old, before extracting the tooth, other options should be considered and the case should be carefully assessed. In patients over 14 years old, significant changes are not expected and extraction should only be considered if the patient rejects surgical treatment.20 Thus it can be concluded that early diagnosis with a timely orthodontic or surgical intervention can assist dentists to preserve the canines, which play an important role in both aesthetics and function.
The patient may, however, be unwilling for the surgical removal of the canines, as in the present case. This might lead to the following complications, which the patient should be made aware of:
Odontogenic cyst and tumour formation;
The mandible becomes prone to fracture;
Alteration in the facial profile – (aesthetic problems as seen in present case, Figure 1a);
The canine can further migrate towards the posterior region causing resorption of roots of adjacent teeth;
Lower lip parasthesia if the tooth impinges on the mental nerve.
If any pathology is seen on radiographs, treatment is strongly advised. If no pathology is observed, patient should be counselled and regular radiographic follow-up suggested, with any significant tooth movements noted.
Conclusion
Although the transmigration of mandibular canines is an unusual event, some cases are extreme. It is important to diagnose them in the earlier stages of migration or abnormality to prevent more complicated situations. Failure to detect such teeth, however, could lead to serious damage to the adjacent teeth and surrounding bone. From a genetic standpoint, many questions relating to the aetiology still remain unanswered and the detailed mechanism of the occurrence of transmigration is a subject of further genetic research.