This paper presents five clinical cases demonstrating the use of the Upper Begg Lower Straight Wire (SWA) technique. It is a method for correcting Class II buccal segments but not involving the classic Begg technique. It frees the occlusion and tips the upper buccal segment teeth distally, and then a Nance button is used for anchorage reinforcement whilst the teeth are uprighted.
Clinical Relevance: This article outlines an alternative method for correcting Class II buccal segments without the need for extractions.
Article
The first real multi-bracketed system, the Ribbon arch bracket, was developed by EH Angle 100 years ago, although its description did not appear in print until 1916.1 Despite Angle's introduction of the ‘edgewise bracket’ in 1927, the use of the ‘ribbon arch’ continued until the 1960s, when the cost of gold/platinum brackets and archwires could not compete with stainless steel systems. BF Dewel has written a good description of this appliance.2
PR Begg was a student at Angle's School of Orthodontia in 1924–25 and may have been the first to use the ‘edgewise bracket’, which was then under development. However, after returning to Australia, he abandoned the ‘edgewise bracket’ and modified the ‘ribbon arch’ appliance. In collaboration with the metallurgist AJ Wilcock, he developed the Light Arch Wire Differential Force Technique in 1961.3 This appliance used a stainless steel version of the ribbon arch bracket, turned upside down. This allowed third order movements to be produced by torquing auxiliaries made of highly resilient stainless steel wires.
Later described as the Begg theory, there were three important features:
Light forces were used for initial alignment and overjet reduction and heavy forces were used where it was required to protract the buccal segments. This was a theory know as differential anchorage.
The teeth were tipped into the correct position and then uprighted.
Extractions were a feature. This followed from Begg's doctorate (University of Adelaide 1935), ‘Some Aspects of the Aetiology of Irregularity of Teeth’. It was later published in the AJO as ‘Stone Age Man's Dentition’.4 This justified the extraction of premolar teeth to simulate natural attrition of the teeth.
HD Kesling was so impressed with Begg's cases that he was instrumental in Begg's presentation to the American Association of Orthodontists (AAO) in April 1960. Kesling was largely responsible for introducing Begg therapy to the USA.
The technique described in this paper uses Begg brackets in the upper jaw and makes use of the free tipping and uprighting system described by Begg. However, the basic idea is quite different from that of Begg therapy. It uses the highly resilient uprighting springs to distalize the upper arch.
Indications
This technique can be used for the treatment of Class II molars when the lower arch is not crowded or where the crowding is so mild that alignment will not lead to over-proclination of the lower incisors. At Queen's Hospital, Burton upon Trent, it has proved to be useful in the following situations:
Class II division 1 malocclusions with Class II molars and a well-aligned lower arch;
Class II division 2 malocclusions with Class II molars and a well-aligned lower arch;
Class II division 2 malocclusions with Class II molars and where the lower arch is crowded but it is felt that alignment will not cause excessive proclination of the lower incisors;
Unerupted maxillary canines and Class II molars. The aim is to open the space for the canines to 10 mm within 3 months of starting treatment. This treatment does not require the removal of premolar teeth, therefore it avoids the risk that premolars may be extracted and the canines subsequently prove to be ankylosed. The use of Begg brackets on the lateral incisors is reassuring because the root of the lateral incisor cannot be forced into the path of the erupting canine because it is always free to tip away;
Class I malocclusions with upper arch crowding and Class II molars;
Re-treatment cases where premolars have been lost but the molars remain Class II;
Functional appliance cases where full overjet reduction has not been achieved.
Method
Bonding of the appliances
Pre-adjusted edgewise brackets are bonded in the lower arch. Bands or tubes can be used on the lower first molars. It is important not to bond the second molars at this stage.
In the upper arch Begg brackets are bonded (TP Orthodontics 256–550 for flat bases and TP Orthodontics 256–650 for curved base brackets). Position the brackets in the long axis of the clinical crown, in a similar position to the pre-adjusted edgewise brackets. Bands must be used on the first molars. For this technique they do not need to have Begg tubes; pre-adjusted edgewise tubes are preferable. It is important to note the size of the bands fitted.
Phase A: alignment
Align the upper arch with a round NiTi wire, retaining the wire using brass pins. For classic Begg Therapy, a number of different pins are suggested for different stages but for this technique only two types of pin are needed; the hook pin (TP Orthodontics 207–341) can be used in all cases except where an additional attachment is needed for an elastic, when a high hat pin is used (TP Orthodontics 202–152).
It is necessary to close any space between the upper incisors. This can be done with a light elastic between the pins. In the lower arch it is necessary to work through the archwires to engage a thick steel wire fully.
Phase B: bite correction
The lower arch is now fully aligned and will act as an anchorage point for Class II elastics. A 0.019” x 0.025” steel wire should be placed with a lingual bonded retainer LR4 to LL4.
The upper arch should be 0.016” special or special plus wire with circle hooks just distal to the lateral incisors, molar offsets and 30° anchor bends. An important feature is the cement on the second molars, to remove any cuspal interference completely. It must be allowed to set hard before the patient leaves the surgery.
Distalization of the upper arch is achieved in three ways:
20–30° anchor bend in front of the upper molars tipping them distally;
Uprighting springs in Australian special plus on the premolars and canines tipping them distally (arms of the springs mesial to the teeth);
Strong Class II elastics (TP Orthodontics tru-force [orange] ¼” 4.5 oz).
Correction from Class II molars to Class I molars should be achieved within 12 weeks. Furthermore, the overjet should be normal before progressing to Phase C.
Phase C: cuspation
Take an upper impression over the appliance and place two new upper molar bands in the impression for a Nance button, using bands one size bigger than those used at bond-up. Cuspal locking hinders correction of the molars from Class II to Class I. This is why cement is used to free the occlusion during Phase B, but now that the buccal segments have been corrected it is necessary to remove the cement and use vertical elastics to pull the teeth into occlusion (upper canines to lower canines and first premolars, TP Orthodontics tru-force [red] 3/16” 4 oz).
Phase D: detailing
Cement the Nance button. It may be necessary to bend a new archwire if the ends are not long enough to bend up the ends securely, but often the same wire used in phase B and C can be re-used. If the teeth appear distally tipped, they can be uprighted using uprighting springs (arms of the springs distal to the teeth). If the upper incisors require torque, a two-spur torquing auxiliary can be fitted. A measure of Class II elastics will be required in this stage but the force varies a little, depending on the number of teeth that require uprighting.
Finishing
A few cases may require further detailing after the completion of phase D.
Practitioners who wish to avoid wire bending could consider replacing the anterior brackets with pre-adjusted edgewise brackets.
Clinical cases demonstrating the use of the Upper Begg Lower Straight Wire (SWA) technique
Case 1: Class II division 1
Figure 1.
(a–c) Class II division 1 malocclusion with Class II molars and well-aligned lower arch; (d–f) Phase A: upper and lower NiTi aligning archwires and light elastic upper UR2 to UL2 to close spacing; (g–i) Phase B: bite correction using special plus uprighting springs, cement on lower second molars, lingual bonded retainer LR4 to LL4 and Class II elastics; (j–l) Phase C: cuspation with vertical elastics; (m–o) Phase D: detailing using uprighting springs and Nance button for anchorage reinforcement; (p–r) Finish: Class I incisor and molar relationships.
Case 2: Class II division 2
Figure 2.
(a–c) Class II division 2 malocclusion with Class II molars and well aligned lower arch; (d–f) Phase D: detailing using an uprighting spring, torquing auxiliary and Nance button for anchorage reinforcement; (g–i) Finish: Class I incisor and molar relationships.
Case 3: Unerupted upper canines
Figure 3.
(a) Pre-treatment DPT showing bilaterally impacted upper canines; (b–c) Class II division 2 malocclusion with Class II buccal segments and unerupted upper canines; (d) Phase A: upper stainless steel archwire with push coil in upper three regions to create space for canines; (e–f): Finish: Class I incisor and molar relationships.
Case 4: Failed functional
Figure 4.
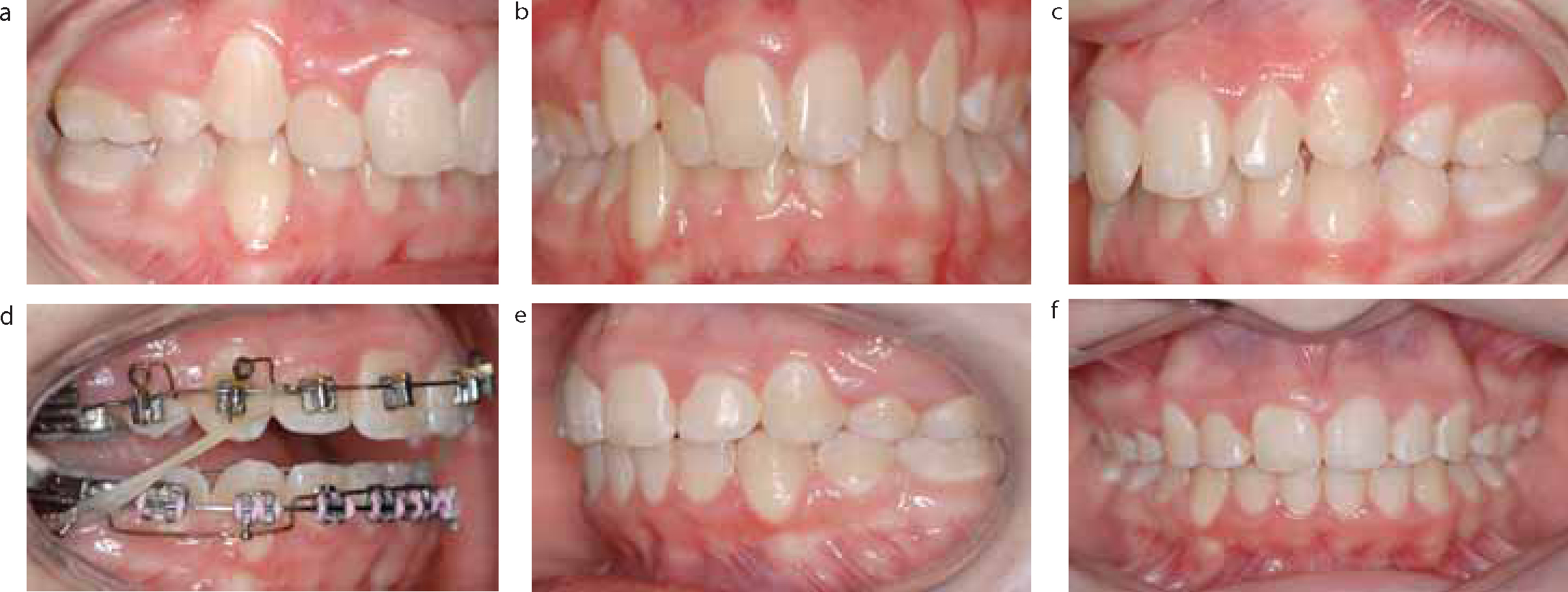
(a–c) Class II division 1 malocclusion with Class II molars and well aligned lower arch; (d) Phase B: bite correction using special plus uprighting springs, cement on lower second molars and Class II elastics; (e–f) Finish: Class I incisor and molar relationships.
Case 5: Previous orthodontic treatment
Figure 5.
(a–c) Class II division 1 malocclusion with ½ unit Class II buccal segments and previous loss of four premolars for orthodontic treatment; (d) Phase B: bite correction using special plus uprighting springs, cement on lower second molars and Class II elastics; (e–f): Finish: Class I incisor and molar relationships.
Conclusion
The technique outlined provides a predictable and reliable treatment method for patients not suitable or willing to have treatment with a functional appliance, headgear or temporary anchorage devices, for the correction of Class II buccal segments.
For further details or comments visit: www.burtonortho.co.uk